MOD 7 - Measuring and Minimizing Radiation Exposure
Learning Objectives
identify methods of measuring and quantifying radiation exposure
describe the role of exposure monitoring devices
describe the use of exposure monitoring devices
describe the method of measuring and reporting exposure from monitoring devices
state the SC35 requirements ('must') and recommendations ('should') that limit exposure to personnel and radiation workers
state the risk/benefit requirement for radiation exposures
identify the SC35 requirements of the responsible user/operator
Radiation Exposure Measurement
Absorbed Dose (D) / Air Kerma / Surface Skin dose
most current method of measuring radiation exposure
D = amount of energy absorbed by material per unit mass through interaction with ionizing radiation
provides entrance dose value to the exposed PT / amount of energy the PT receives
does NOT describe the potential for biologic effect
“D” Method of measurement:
Using ionization chambers, the energy of exposures is measured and quantified as joules/kilogram (J/Kg) and expressed by the unit Gray (Gy)
1 Gy = 1 Joule of energy absorbed per kg of material (units of Air Kerma)
Effective Dose (EfD)
takes in account of the absorbed dose (Gy or J/Kg) and the tissue types exposed (accounting for radiosensitivity, cancer and genetic risk) to convert this into an equivalent whole body exposure to estimate risk
can be calculated from a single imaging exam but results are correlated to population risk, not an individual's risk (as late effects are stochastic)
application of the radiation type
Calculation:
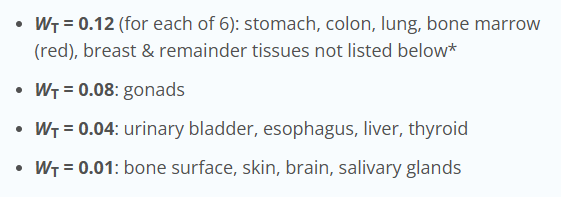
absorbed dose x tissue weighting factor x quality factor = radiosensitivity of the region to produce an estimated whole body equivalent dose (Sv)
EfD (Sv) = D x WR x WT
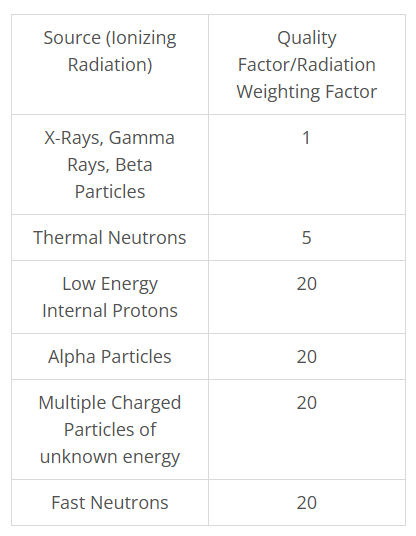
Quality Factor
NOTE: sources of high LET radiation deliver increased energy to tissues that in turn, lead to more biologic damage
same as the Radiation Weighting factor
provides a weighting system that takes into account the degree of biologic damage (RBE) related to the various sources of radiation
allows for various sources of ionizing radiation to be compared and evaluated based on the potential for biologic damage (RBE)
Equivalent Dose
= absorbed dose x quality factor
allows exposures to be compared between the various sources of radiation
expressed in Gray (Gy)
Dose Area Product (DAP)
modern method of measuring and recording patient exposure that is built into current radiography and fluoroscopic equipment
measure of the total radiation administered to the patient
DAP (mGy-cm2) = air kerma (Gy) x exposure field size (cm2)
shows how reducing field size with collimation reduces PT dose
highly dependent on individual characteristics, such as dimensions, BMI and weight distribution and gender
takes into account of the area we’re exposing on partial body
an ionizing chamber that measures the dose before collimation
DAP and Fluoro Exams
takes in account of the time that the x-ray beam was energized known as fluoro time
however it is missing important information such as the Air kerma
cumulative air kerma (CAK)
takes into account the DAP and the dose measured at the interventional reference point (IRP)
expression of dose accumulated from an entire fluoroscopy procedure (mGy)
Current Standards of Radiation Protection
Safety Code 35: Radiation Protection in Large Facilities
outlines the “safety procedures for the installation, use and control of x-ray equipment in large medical radiological facilities
application:
large medical radiological facilities
NOT to radiation therapy, dental, mammography, or small radiological facilities\
Close cooperation between technologists, medical professionals, medical physicists, and other support staff will allow a facility to achieve an effective radiation protection program
safety:
SC35 provide recommendations
four main safety principles
PT should not be subjected to unnecessary radiological procedures
PT should be protected from excessive radiation during exam
workers should be protected from excessive exposure to radiation during work
Personnel and the general public in the vicinity of such facilities require adequate protection
Roles and Responsibilities
Owner Responsibility
Equipment and install meet safety standards
Radiation safety program developed, implemented and maintained
Responsible User
Monitor/manage radiation safety program including
Personnel requirements, equipment performance
Safety procedures and program communication to staff
Radiation Technologist Responsibility
possess required qualifications and be certified by the CAMRT
maintain training and knowledge as required
possess documentation of training in safe operation, procedures performed (including positioning), equipment operation and radiation protection methods
have access to equipment user manuals
possess knowledge of radiation hazards and steps to mitigate these hazards
monitor personal exposure
have thorough knowledge of safe work practices including the use of personal protective equipment
strive to eliminate repeat patient exposures and reduce all exposures to the lowest practical value (ALARA) this is an important requirement
participate fully in QA processes
understand the recommendations of SC35
Exams are performed in a manner that does not cause unnecessary exposure to patient’s, self or others
Possess and maintain recognized qualifications and documented training- CAMRT (or Royal College of Physicians)
Recognize radiation hazards and take steps to minimize
Monitor personal exposure (uses dosimeter if likely to receive 1/20th of a radiation worker limit)
Have a thorough understanding of safe working methods, * including appropriate techniques, PPE and procedures
Referring Practitioner
Authorized to prescribe diagnostic or interventional x-ray procedures
Responsible to ensure the prescribed procedure is JUSTIFIED based on professional experience, judgement and common sense
Give consideration to alternative non-ionizing diagnostic procedures
Be aware of risks/benefits to inform patient
Radiation Detection and Measurement
SC35 states
when staff is likely to receive more than 1mSv per year they are required to wear a personal dosimeter
Ion Chambers
most common type of radiation measurement tool
used to accurately measure diagnostic x-ray beams
portable versions can be used when exposure levels exceed 1mR/hr
being replaced by solid-state detectors which are smaller and provide increased sensitivity to radiation levels
Personal Monitoring Devices
if a protective lead apron is worn, the dosimeter must be worn beneath the apron at waist level
devices include
Film badges
Thermoluminescent dosimeters (TLD)
Optically stimulated luminescence (OSL)
functions to erasure the amount of radiation a worker receives over a regulated period of time
used one is sent for evaluation (usually to Landauer)
NOTE: All personal dosimeter records must be maintained for the lifetime of a facility
Dose Limits
annual acceptable dose limits for occupational radiation workers = 20mSv (whole body equivalent exposure)
NOTE: Technologists regularly working in interventional, fluoroscopy rooms and OR imaging should wear lead glasses and thyroid shields, as well as be assigned a second OSL that is worn at the collar level on the outside of the lead apron/thyroid shield → provides measurement data related to the unprotected regions of the neck and head (including the lens of the eye)
Film Badges
not commonly used in the clinical environment as they are not useful beyond three months and they tend to fog
inexpensive
have been replaced by TLDs and OSLs
Thermo-luminescent Dosimeters (TLDs)
expensive method of measuring occupational exposure
single-use but accurate over a small energy range of 20-250keV
Dosimetry Process
After three months of use, the TLD device will be sent to the provider to process
uses heat that causes the energy absorbent luminescent phosphor in the TLD to release the stored energy in the form of light
photomultiplier tube then measures the amount of light emitted
amount of light signal recorded is then converted to the estimated radiation dose
can be incorrect due to multiple factors (putting it in washer, dryer, exposed to scatter)
Optically Stimulated Luminescent Devices (OSLs)
most common radiation monitoring device used in British Columbia
Dosimetry Process
After up to 1 year of use, the OSL will be sent to the provider for testing
laser will stimulate the OSL material and cause excitations within the device
causes stored energy to be released as emitted light
intensity of the light signal is analyzed by a photodiode
information is related to a radiation dose
highly sensitive device can record exposures as low as 10microSieverts and as high as 10 Sv
New Techonolgy
allows dosimetry info to be accessed instantly
worn as a regular OSL but is connected to the Internet through a USV key for a radiation dose reading
Minimizing Radiation Exposure
Procedures for Minimizing Personnel Exposure
X-ray rooms are used for one exam at a time
All persons must leave the room during exposures unless they their presence is essential
All personnel must maximize their distance from the x-ray beam. Direct exposure of personnel must never be allowed.
Irradiation of an individual for training purposes or equipment testing must never occur
All personnel must use protective devices
Personal dosimeters (Wearing and Storing Criteria)
Pregnancy: once declared must not exceed 4 mSv
Mobile Equipment Guidelines
Must be disabled when left unattended
Are only performed when patient condition precludes transfer to the department
Primary beam is directed away from occupied areas
Every effort is made to avoid irradiating other persons in the vicinity
Operator must not stand in the path of the CR
Operator must stand at least 3m away from source (or wear protective equipment)
Procedures for Reducing Patient Dose
Justification: Review history and correlate with request to ensure the order is for the right patient, right part and appropriate for the hx
Optimization: Consider possible optimization strategies. These include • Consideration of pathologies that may require exposure reduction (osteoporosis) • Consider adjusting technical factors to reduce dose (decrease mAs with appropriate increase in kVp)
Repeat Reduction: Take the time to do it right the first time! Use positioning aids and immobilization devices, preset techniques, etc. Rushing doesn’t help.
Distance/Shielding: Be sure to use the maximum SID for the equipment and exam. This reduces skin entrance dose significantly. As well use of proper collimation to reduce exposure to unnecessary tissues is a dose reducing practice.