Renal System
Kidney Function and Anatomy
Humans have 2 kidneys, each about the size of a fish that sit in the midsection (distally)
Kidneys receive blood from the heart, filter it, and reabsorb what is needed, then produces urine with the waste products to expel from the body
Kidneys can hold about 22% of body’s blood supply
Each kidney has an oxygenated blood vessel (renal artery) and a renal vein
- artery holds onto everything in the blood, from nutrients, to oxygen, to waste products
* too much of a nutrient becomes a waste product - vein takes filtered blood, which still has the nutrients and some oxygen away
Kidneys are critically important in maintaining homeostasis by regulating pH level (via H+ ions), blood pressure (via Na+ and Cl- ions) as well as osmolarity and expulsion of waste. It also makes hormones
- Homeostasis is done through the 2 capillary beds present in each kidney:
* Vasa Recta delivers oxygen to kidney tissue
* Peritubular capillaries recollect nutrients to filter and return via the veins
kidney functions:
- filtration (rids blood of waste)
- collection (collects waste products into the urine)
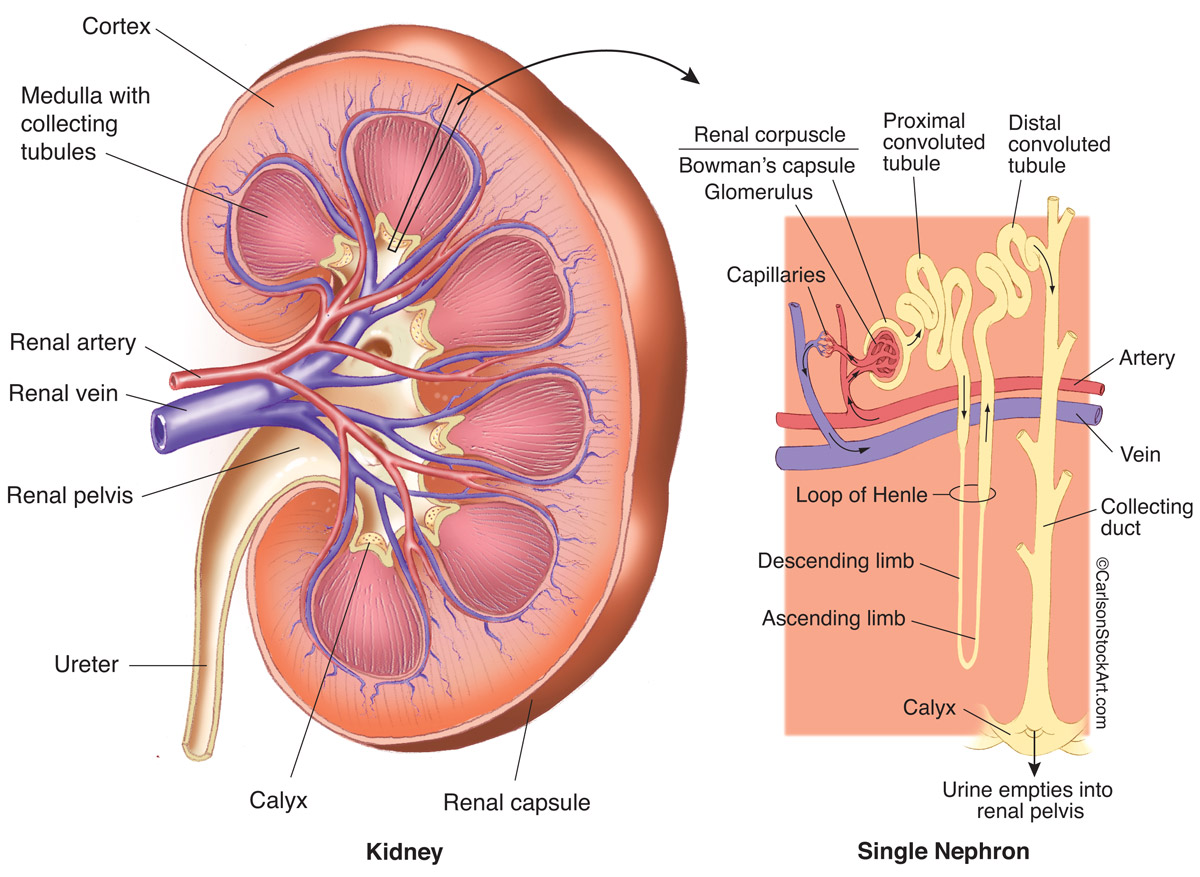
The nephron is the functional unit of the kidney and is responsible for both functions
- situated in both renal cortex and renal medulla
* renal calyx: part of the nephron that is situated in the renal medulla and is the first part where urine is present
* renal pelvis: where all the calyces collect together
Urine exits the kidney through the ureter off the renal pelvis and sends it to the bladder
- any organ with tubes, the tubes are collectively known as helium
Filtration Process Overview
Occurs within the nephrons
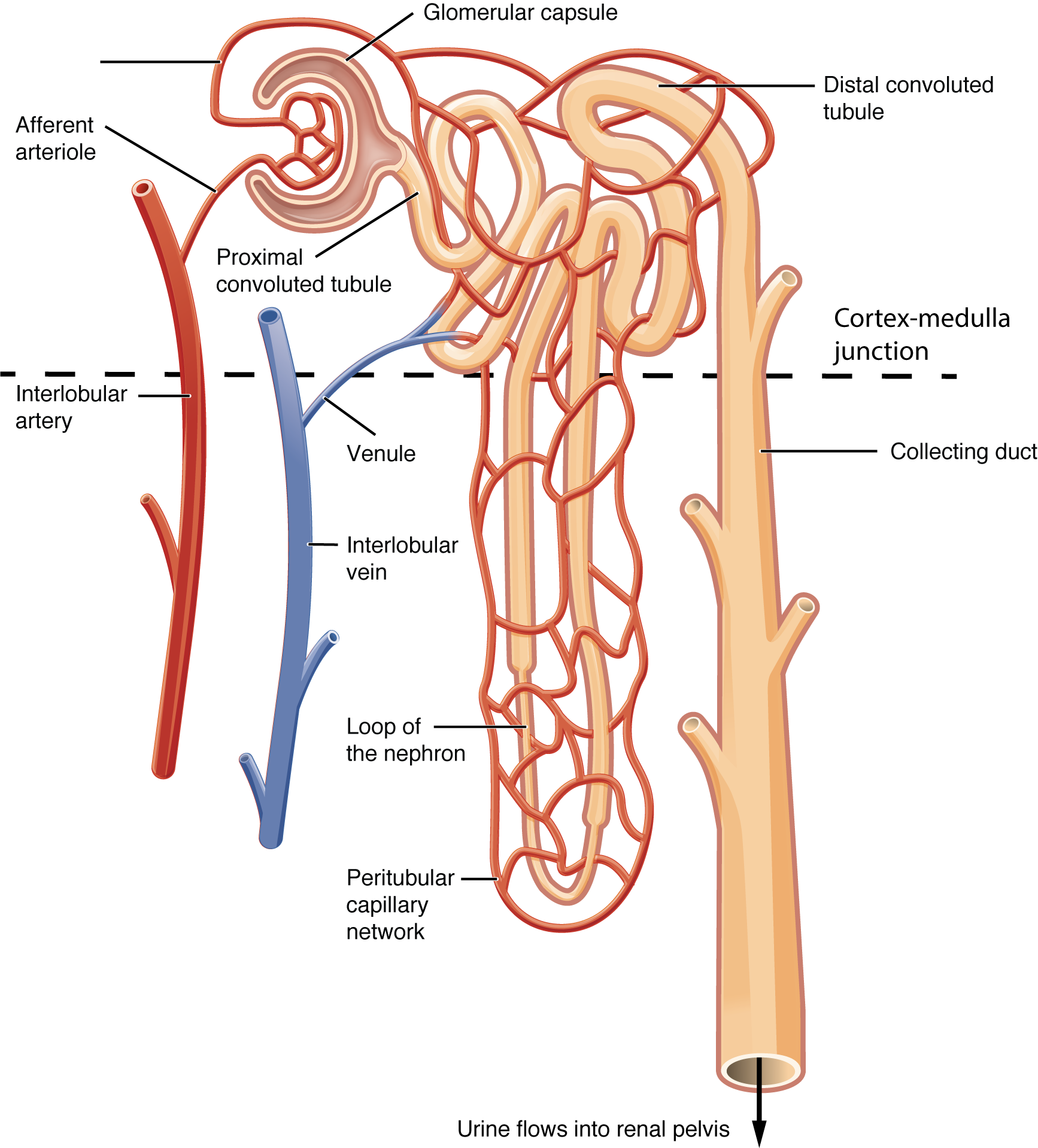
- blood enters the kidney through the kidney through the afferent arteriole and goes into the glomerulus
1. eventually blood leaves through the efferent arteriole (allows for maintaining pressure)
- blood enters the glomerulus, with a fifth of it going into the Bowman’s space
1. fluid is the filtrate and contains things that are easily dissolved (sodium, glucose, amino acids, etc.) and things that do not dissolve easily (RBCs) are filtered by the liver
- filtrate enters the proximal tubule where important nutrients are reabsorbed
1. ATP is used to pump out sodium, which helps bring in other things
- the capillary system that lines the tubule that pumps blood that doesn’t go into filtrate back into the body
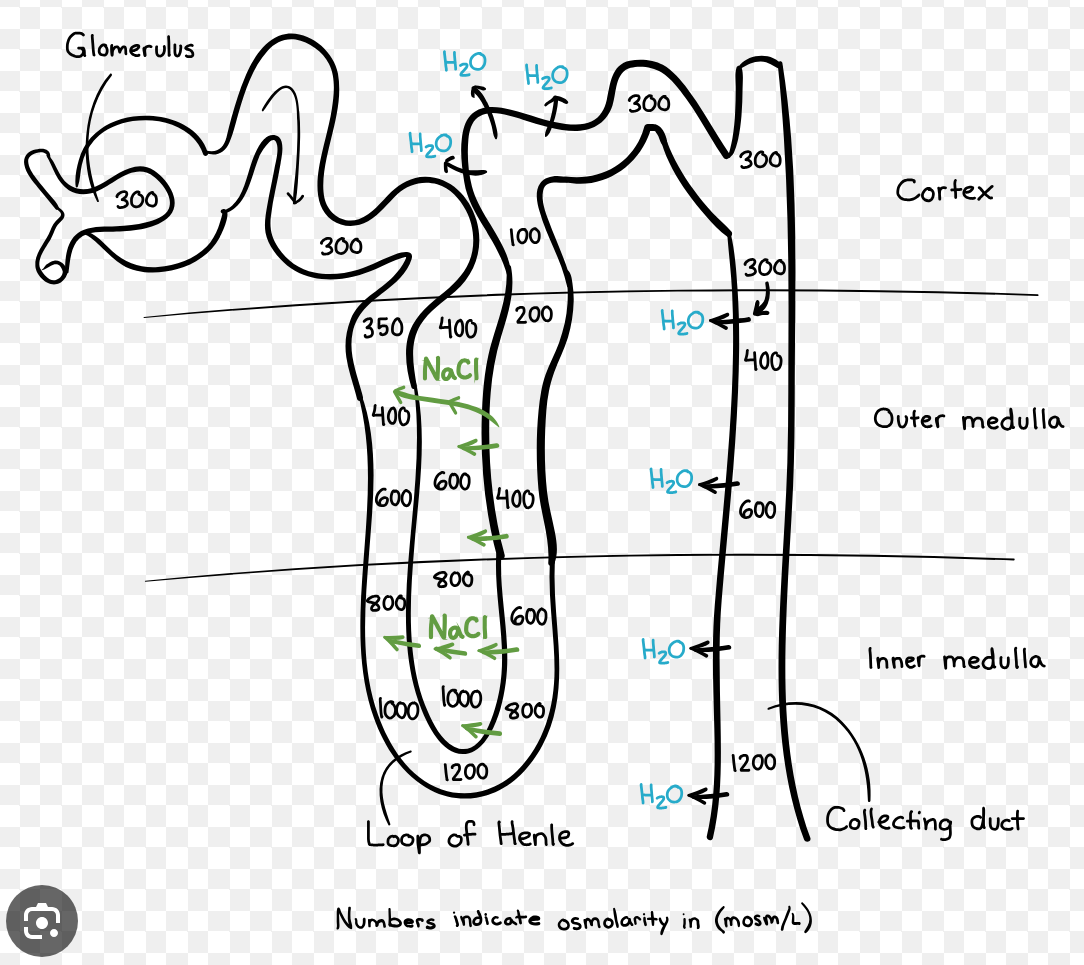
- filtrate then enters the loop of henle, which makes up most of the nephron and extends into both the renal cortex and medulla
1. loop of henle makes the renal medulla space hypertonic/salty by actively pumping out salts by using ATP
2. ascending part of the loop is only permeable to salts, where the descending part is only permeable to water
1. the descending loop is where water molecules diffuse out and its where filtered water from the Bowman’s space is gained back
- after the loop of henle, the filtrate reaches the distal convoluted tube where more nutrients and some water are reabsorbed
- filtrate is now processed and dumped into collecting ducts which go back down into the medulla
1. ADH dictates how porous the collecting duct is. The more porous= more water reabsorption
2. filtrate is even more concentrated
- Eventually collecting ducts dump filtrate into ureter where it exits the kidney
Main substances that are excreted in urine are:
- metabolic waste products (urea, creatinine)
- electrolytes/inorganic compounds (used to control fluid levels)
- water
Vital for keeping homeostasis and ensures body’s physiological processes continue operating effectively
Glomerular Filtration in the Nephron
The first step in making urine is for the glomerulus to separate the liquid part of your blood from your blood cells and turn it into filtrate, and allow the rest of the blood go on
- Filtrate contains all sort sort of ions and nutrients, basically anything that can be dissolved in water
- things that cannot be dissolved in water, do not leave the capillary
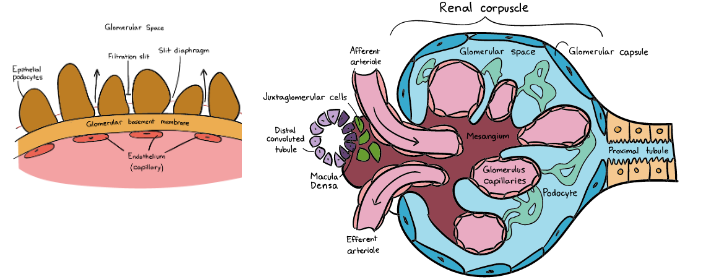
Blood that is about to be filtered enters the glomerulus, which is a tuft of of blood capillaries
- the glomerulus is nestled within the Bowman’s capsule or glomerular capsule
How does the glomerulus capillary actually determine what is filtered and how much is filtered into the Bowman’s capsule. The capillary walls are made up of 3 layers of filtration:
- Endothelium: relatively large pores which solutes, plasma proteins, and proteins can pass through
- Basement membrane: also made up of three layers and is fused to the endothelial player. It prevents plasma proteins from being filtered out of the blood stream
- Epithelium (Tubular cells): consists of specialized cells called podocytes which are attached to the basement membrane by foot processes (pedicels)
1. podocytes wrap around the capillaries and contain filtration slits between them
2. a thin diaphragm between the slits acts as a final filtration barrier before fluid enters the glomerular space to the Bowman’s capsule
Together the glomerulus and Bowman’s capsule filtering unit are known as a renal corpuscle
In addition to the glomerular capillary bed, the kidneys contain vasa recta and peritubular capillaries that concentrates urine
Changing Glomerular Filtration Rate
The glomerulus contains two arterioles that its sandwiched between- afferent and efferent arterioles
- both are high in pressure but can change in size to increase or decrease blood pressure in the glomerulus
- this allows for control over increasing or decreasing filtration
- the efferent arterioles are smaller in diameter than afferent arterioles, which means blood is more pressurized as it exits and can allow for more filtration
- high glomerular capillary pressure filtration is maintained regardless in fluctuations in blood flow
Glomerular Filtration Rate= rate at which kidneys filter blood
The main driving force for the filtering process, or the outward pressure, is the blood pressure as it enters the glomerulus. This is counteracted to some extent by inward pressure due to the hydrostatic pressure of the fluid within the urinary space, and the pressure generated by the proteins left in the capillaries that tend to pull the water back into the circulatory system (colloidal osmotic pressure)
The net filtration pressure is the outward pressure minus the inward pressure
Regulation of glomerular filtration rate: it’s normal for your blood pressure to fluctuate throughout the day, but it has no effect on the glomerular filtration rate… how?
- Renal autoregulation: the kidney itself can adjust the dilation on constriction of the afferent arterioles, which counteracts changes in blood pressure (intrinsic factor)
* works over a large range of blood pressure, but can malfunction if you have kidney disease - Neural control and hormonal control: (extrinsic factor) can override renal autoregulation and decrease the glomerular filtration rate when necessary
- Hormonal control: ANP (atrial natriuretic peptide) can increase your glomerular filtration rate.
* produced in the heart and is secreted when plasma volume increases, which increases urine production
Glomerular filtration rate (GFR) can be estimated using creatinine
- creatinine is a waste product made in muscle when it is metabolized to generate energy
- is exclusively filtered through kidneys, its rate of excretion from your blood is directly related to how efficiently kidney filtration is
- GFR can be estimated by amount on creatinine in a blood sample as well as age, ethnicity, gender, height, and weight
Countercurrent Multiplication
Countercurrent multiplication in the kidneys is the process of using energy to generate an osmotic gradient that enables the reabsorption of was from the tubular fluid and produced concentrated urine
The kidney contains two types of nephrons, superficial cortical nephrons (70-80%) and juxtamedullary nephrons (20-30%)
- the names refer to the location of the glomerular capsule, which is either in the outer cortex of the kidney or near the corticomedullary border
- Loop of Henle of the cortical nephrons penetrates only as far as the outer medulla of the kidney, but that of the juxtamedullary nephrons penetrate deep into the inner medulla
* the juxtamedullary nephrons are largely responsible for countercurrent multiplication (although both types regular solute/water levels)
Overview of Countercurrent multiplication
The loop of Henle has ascending and descending limbs that go in opposite directions and have different permeabilities:
- descending limb: passively permeable to both water and small solutes (ions, urea, etc.)
* water and solutes move down their concentration gradients until their concentrations within the descending tubule and the interstitial space have been equilibrated
* water flows out of descending limb and into the medullary tissue, causing the filtrate to become further concentrated - thin ascending limb: passively permeable to small solutes, but impermeable to water, which means water cannot escape from this part of the loop
* solutes/ions passively leave the loop and filtrate into the medullary tissue/interstitium - thick ascending limb (diluting segment): actively transports salts (Na+, K+, and Cl+) out of the filtrate and into the medullary interstitium. Impermeable to water
The medullary interstitium becomes very salty, which causes the medulla to suck water out of the collected duct by osmosis when the collecting duct is permeable to water (in the presence of ADH)
Longer loops=greater osmotic gradients
The vasa recta that surrounds the loop is equally important for creating the gradient because it returns absorbed water into the circulatory system
- vasa recta are long, hairpin shaped capillaries that run parallel to the loop
* the hairpin turns present on the capillaries slow the rate of blood flow so any solutes that are reabsorbed into bloodstream have time to diffuse back into the interstitial fluid, maintaining the hyperosmotic medulla for water reabsorption
Urination
After urine concentration in the nephrons, it flows through the collecting duct to the renal calyx at the tip of the medulla.
Several renal calyces come together to make the renal pelvis, and from there the urine flow out of the ureter into the bladder
- ureters attach to the back of the bladder and have have valves that prevent backflow of urine up the ureter towards the kidneys
- ureters spray urine into the bladder with the ureter jet
The bladder is lined with transitional epithelium, which is structurally somewhere between flat squamous epithelium and columnar epithelium
- transitional epithelium allow the bladder to expand
The bladder then funnels into the urethra, controlled by the internal urethral sphincter, which is made of smooth muscle (involuntary movement)
In women: after the IUS, there is an external urethra sphincter, a membranous part surrounding the urethra
- the EUS is made of skeletal muscle and control of it is learned during potty training
- after the EUS is the urethra (which is fairly short) and then urine is excreted
In men: after the IUS there is a prostatic urethra (passes through the prostate which circumscribes the urethra) and then to the EUS
- after the EUS, the urine will travel through a urethra section called the spongy urethra, located in the penis
- after traveling through the spongy urethra, the urine is excreted
Renal Regulation of Blood Pressure
Overview of RAAS System and Renin Production
RASS= renin angiotensin aldosterone system
- Renin is an endocrine peptide hormone that helps raise blood pressure
* it is secreted by the juxtaglomerular apparatus (which is made of the afferent and efferent arterioles that contain mesangial cells for structure, endothelial cells and smooth muscle, clusters of juxtaglomerular cells, and a tunica externa layer which has nerves connected to the sympathetic nerve)
* it is released into the afferent arteriole, goes through the glomerulus, and exits through the efferent arteriole
* triggers for renin release include
* low blood pressure sensed in the afferent arteriole
* sympathetic nerve stimulation which fires on afferent arteriole
* low sodium concentration in distal tube sensed by macula densa cells - Angiotensinogen is released by the liver and is a large inactive hormone (450 a.a’s)
* Angiotensinogen reacts with renin present in the blood and angiotensinogen converts into angiotensin 1 (renin catalyzes conversion)
* Angiotensin 1 is then converted by ACE (angiotensin converting enzyme) that is present within the endothelial cells of capillaries into Angiotensin 2
* Angiotensin 2 ultimately raises the blood pressure by causing a few changes:
1. Vasoconstriction: increases resistance and blood pressure (angiotensin= blood vessel tension)
2. Increases sodium reabsorption in the kidneys: also causes more water reabsorption
3. Aldosterone release/secretion
4. ADH release
5. Increases blood osmolarity and volume
- In turn, glomerular filtration rate is also increased along with systemic blood pressure
Details of Aldosterone Function in Raising BP
Aldosterone is released by the adrenal cortex.
- adrenal cortex cells are provided nutrients/oxygen by small capillaries and they’re filled with cholesterol, which is useful in in making aldosterone
Triggers for aldosterone production:
- angiotensin 2
- increase in potassium concentration
Aldosterone affects the late distal convoluted tubules and the collecting ducts near the nephrons
- these tubules are lined with principal cells, which are adjacent to peritubular capillaries
- there are lots of potassium ions inside the principal cell and lots of sodium in the blood flowing through the capillaries. These ions are exchanged through the sodium-potassium pump on the basolateral surface of the capillaries
Aldosterone works by:
- making the sodium-potassium pump in the tubule/duct work harder
- opening potassium channels on the apical surface of the capillary so potassium flows out of the principal cells into the fluid (soon to be urine) flowing through the tubule. This increases drive to get potassium into the cell
- opening sodium channels, moving sodium into the principal cell from the urine, which makes the pump work harder to pump sodium out of the principal cells (in the tubules) and into the capillaries
All of this causes a water gain and increased stroke volume and blood pressure
Acid Removal in Blood by Aldosterone
Acid is removed from the blood by bringing in HCO3- from alpha-intercalated cells to neutralize it but the reaction causes hydrogen to remain within the alpha-intercalated cells (located in collecting duct). The hydrogen is removed from the cells by several transporters, two of them (secondary transport of hydrogen by sodium gradient and active transport) are driven by aldosterone
When pH is too high, HCO3 is excreted in the urine.
When pH is too low, H+ is excreted in the urine
Carbonic anhydrase catalyzes the conversion of carbon dioxide into carbonic acid, which dissociates into bicarbonate and a proton. The kidney can then excrete the bicarbonate or proton or reabsorb the molecules.
ADH
ADH/vasopressin/anti-diuretic hormone is a hormone released by the posterior pituitary when blood volume is low and the solute concentration is high which can occur when dehydrated
- prevents diuresis (water loss in urine) by increasing water reabsorption in distal nephron (mostly collective duct) by making it water permeable (without ADH, this region is water impermeable)
- water is picked up from the tissue of the kidney by peritubular capillaries and returned to the blood
Drinking too much water stops the secretion of water so the collecting duct is impermeable and excess water is lost in urine
Aldosterone can trigger ADH secretion
- aldosterone causes sodium reabsorption which results in increase plasma osmolarity
- this causes ADH to be secreted to increase water reabsorption and plasma volume
Increase volume but maintain osmolarity: increase ADH
Increase volume, regardless of osmolarity: increase osmolarity
Decrease osmolarity, regardless of volume: ADH
Decrease osmolarity, maintain volume: increase ADH, decrease aldosterone