Ninja Nerd- Renal
Glomerular Filtration Video 1/9
Definition of Renal Corpuscle:
Composed of two parts:
Glomerulus: A tuft of capillaries, specifically designed for filtration.
contains endothelial lining and G.B.M
Bowman's Capsule: Also known as the glomerular capsule, collects filtrate from the glomerulus.
contains parietal and visceral layer (podocytes)
Glomerulus Structure
Glarus: The tuft of capillary vessels in the glomerulus.
Afferent Arteriole:
The blood vessel that supplies blood to the glomerulus.
Efferent Arteriole:
The resulting vessel that drains blood from the glomerulus; one of the few instances in the body where a capillary bed is supplied by an arterial and drained by another arterial.
Capillary Types in the Glomerulus
Fenestrated Capillaries:
Characteristics:
Endothelial cells have numerous small pores (finestra) that allow for filtration.
Pores are approximately 50 to 100 nanometers in diameter.
Filtration Capacity:
Formed elements (e.g., red blood cells, white blood cells, platelets) cannot pass through due to size.
Small proteins, electrolytes (sodium, potassium, calcium, chloride), water, nutrients, and waste products can pass through.
Glomerular Basement Membrane (GBM)
Definition:
The critical filtration barrier of the glomerulus comprising three layers:
Lamina Rara Interna:
The side nearest the endothelial cells.
Composed of proteoglycans (e.g., heparan sulfate), which are negatively charged (critical for filtration).
Lamina Densa:
Consists of type IV collagen and laminins (lamins= proteins), dense structure.
Lamina Rara Externa:
The outer side toward the podocytes, also rich in heparan sulfate.
Filtration Process
Charge Interaction:
Negatively charged particles (e.g., plasma proteins like albumin) are repelled by the negatively charged GBM, while positively charged particles pass through easily.
Neutral particles: May pass through but not as efficiently as positively charged particles.
Ex. positive substance: electrolytes Na, K, etc
Filtration Slits:
Formed by podocytes (foot cells) in the Bowman's capsule; spaces between foot processes are 25 to 30 nanometers wide.
Néphrine Protein:
Forms the slit diaphragm, only permitting particles around 7 to 9 nanometers to pass through.
Very important for controlling what enters fenestration pores, negatively charged GBM, and <25-30nm will make it through
Nephrine only allows <7-9 nm to pass
Bowman's Capsule
Layers of Bowman's Capsule:
Parietal Layer:
Forms the capsule surrounding the glomerulus.
Visceral Layer (Podocytes):
Formed by foot cells (podoctyes).
Filtration Outcome
Commonly Filtered Substances:
Water, glucose, amino acids, electrolytes (sodium, potassium, calcium, magnesium), urea, creatinine, vitamins.
Exclusions:
Plasma proteins (e.g., albumin, immunoglobulins) due to size and charge properties (repelled from GBM).
Key Cells Associated with Filtration
Mesangial Cells:
Function:
Can phagocytose trapped molecules in the slit diaphragm and regulate blood flow via contractile activity from A arteriole to glomerulus
Juxtaglomerular (JG) Cells:
Baroreceptors that produce renin, important for blood pressure regulation.
Net Filtration Pressure (NFP)
Definition:
The driving pressure of filtration in the glomerulus.
Formula for NFP:
Pressures Involved:
Glomerular Hydrostatic Pressure (P_{glom}):
Average of 55 mmHg, pushes fluids out from capillaries into Bowman's capsule.
Colloid Osmotic Pressure (P_{osmotic}):
Average of 30 mmHg, exerted by plasma proteins (albumin) to retain fluid in the blood.
Capsular Hydrostatic Pressure (P_{capsular}):
Average of 15 mmHg, back pressure of fluids in Bowman's capsule to capillary (adding too much water to funnel)
Calculation of Net Filtration Pressure:
Average NFP = 55 mmHg (hydrostatic) - 30 mmHg (osmotic) - 15 mmHg (capsular)
NFP = 10 mmHg.
NFP= PRESSURE PUSHINHG IN - PRESSURE PULLING IN
(GHP) - (COP + CHP)
NFP DIRECTLY RELATED TO GFR
NFP INC→ GFR INC
Glomerular Filtration Rate (GFR)
Definition:
The volume of plasma filtered per minute, ~125 mL/min.
1200 ml passed through A. arteriole.
625 ml is going to filtered (other 575 passes by)
20% of the 625 is going to be filtered (125ml/min)
Factors Affecting GFR:
Net filtration pressure and filtration coefficient
(KF = surface area x permeability).
Increased surface area increases GFR; decreased area leads to lower GFR.
Permeability= alterations can further impact filtration rates (e.g., diabetic nephropathy affects thickness, glomerulonephritis affects porosity l/t proteinuria).
Clinical Correlations to GFR
High Blood Pressure: —> Increases glomerular hydrostatic pressure.
Low Blood Protein Levels (Hypoproteinemia):—> Decreases colloid osmotic pressure l/t more filtration into Bowman's capsule ( can’t hold onto water)
High protein (multiple myeloma) =protein retains fluid in the bloodstream—> increase in colloid osmotic pressure and reducing the amount of fluid filtered into Bowman's capsule.
Obstructions (e.g., Kidney Stones/ hydronephrosis): —> stone will push back into glomerulus which l/t Increased capsular hydrostatic pressure, reducing net filtration rate.
Proximal Convoluted Tubule Video 2/9
Glomerular Filtration Process
Location of Filtration
Glomerulus acts as the filtration site.
Filtering various substances from blood into the Bowman’s capsule.
Filtered Substances
Water
Electrolytes including:
Sodium (Na⁺)
Potassium (K⁺)
Chloride (Cl⁻)
Calcium (Ca²⁺)
Magnesium (Mg²⁺)
Nutrients such as:
Glucose
Amino acids
Vitamins
Lipids
Very small proteins like insulin and hemoglobin.
Osmolality and its Importance
Definition of Osmolality
Measures the volume of particles per kilogram of solvent.
Distinction from molality:
Molality is defined as moles of solute over kilograms of solvent.
Osmolality is relevant in assessing kidney functions:
Normal Blood Osmolality Values
Typically around 300 milliosmoles per liter (mOsm/L).
Filtrate into the PCT remains at about 300 mOsm/L.
Tubular Processes: Secretion and Reabsorption
Definitions
Tubular Secretion: Movement of substances from blood into kidney tubules; requires ATP. because its active process
Tubular Reabsorption: Movement of substances from kidney tubules back into the blood; may be active or passive (depends on what molecule it is)
Tubular Reabsorption Mechanisms
Transport Processes
Sodium-Potassium ATPase Pumps:
Pump 3 Na⁺ out and 2 K⁺ into the cell against their concentration gradients using ATP.
Result: Low sodium concentration inside cells, high potassium concentration.
Specialized Transporters
Sodium-Glucose Co-transporter= Secondary active transport
Transports sodium (which moves in from the tubule) and glucose (which moves against its gradient).
Mechanism:
Sodium moves down its concentration gradient (passive).
Glucose moves against its gradient (active) using energy from sodium.
Type of Transport: Secondary Active Transport.
Amino Acids
Similar process with sodium-Amino acid co-transporters.
Na in cells is low
A.A are also transporting in (low out, high inside cells)
normally would need ATP to go from low to high concentration gradient. However, since Na is moving across concentration gradient, A.A can tag along
Example of secondary active transport
REMEMBER: 100% of glucose, A.A & lactate are reabsorbed from kidneys tubules to blood stream
Bicarbonate Reabsorption
Reaction involving CO₂ and water forming carbonic acid via Carbonic Anhydrase.
CO2 +H20 ←→ H2CO3 Because of Carbonic Anhydrase
Carbonic acid (H2CO3) dissociates into protons (H⁺) and bicarbonate (HCO₃⁻).
The bicarbonate (approx 90%) then enters the renal tubule cells, where it is further processed and ultimately reabsorbed into the bloodstream, contributing to the regulation of blood pH and maintaining acid-base balance.
Sodium-H⁺ Antiporter:
Sodium enters the cell while H⁺ is secreted.
Bicarb & H combine to form carbonic acid (H2CO3)
carbonic anhydrase converted H2CO3 into CO2 + H2O to be secreted
About 90% of bicarbonate is reabsorbed into the blood.
Ex of secondary active transport
Obligatory Water Reabsorption
Definition
Water follows sodium during reabsorption (obligatory), primarily by osmosis.
Reabsorption Rates
~65% of filtered sodium and 65% of filtered water reabsorbed at the PCT.
Para-Cellular Transport
Definition: Transport occurs between cells to move into blood stream, essential for reabsorption of:
Calcium
Magnesium
Potassium
Chloride
Approximate reabsorption rates:
Potassium: 55%
Chloride: 50%
Chloride Transport Mechanisms
Use of Sodium-Chloride Co-transporter: (symporter)
Sodium and chloride enter the cell and subsequently pushed in the bloodstream.
Transport of Lipids
Lipids
Lipid-soluble substances pass directly through phospholipid bilayer membranes into blood
Urea partially reabsorbed.
Small Proteins Reabsorption
Mechanism for Proteins
Small proteins (e.g., insulin, hemoglobin) may be filtered and reabsorbed through receptor-mediated endocytosis.
Normally proteins aren’t filtered, but can be if small
Proteins engulfed by clathrin-coated vesicles, proteins are broken down in lysosomes to amino acids, and A.A reabsorbed/ pushed into the bloodstream.
Influence of Parathyroid Hormone (PTH)
PTH Effects
Binds receptors on PCT cells, affecting sodium-phosphate transporter.
PTH is Gs —> adenylate cyclase activation leads to an increase in cAMP levels,
which subsequently enhances the reabsorption of calcium and promotes the excretion of phosphate in the kidneys.
Glutamine and Ammonium Secretion
Glutamine: Undergoes deamination to produce 2 ammonium (NH₄⁺) and 2 bicarbonate (HCO₃⁻).
2 bicarbonate ions in blood raise pH during metabolic acidosis.
Cl is then coming into the cells as exchange
Ammonium is actively secreted into kidney tubules using ATP.
Can dissociate into NH3 & H+ (ammonia & hydrogen)
H gets pushed out of the cells and Na enters as exchange
Tubular Secretion of Drugs
Active Secretion of Drugs
Substances like penicillin, cephalosporins, methotrexate, morphine, and organic bases & organic acids (e.g., uric acid), bile salts/ acids are actively secreted into the proximal convoluted tubule, requiring ATP.
Loop of Henle Video 3/9
Introduction to the Loop of Henle
The video focuses on the Loop of Henle, a key component of the nephron in the kidneys.
Viewers are encouraged to watch related videos on glomerular filtration and proximal convoluted tubule (PCT) before watching this one for better understanding.
Structure of the Loop of Henle
Comprises two main parts:
Descending limb: The part that descends into the renal medulla.
Ascending limb: The part that ascends back towards the cortex.
Nephrons
Definition of Nephron: The functional unit of the kidney, responsible for filtering blood and forming urine.
Composed of:
Renal Corpuscle:
Glomerulus: A network of capillaries.
Bowman's Capsule: Surrounds the glomerulus.
Proximal Convoluted Tubule (PCT): Reabsorbs nutrients, water, and electrolytes.
Loop of Henle: Divided into descending and ascending segments.
Distal Convoluted Tubule (DCT): Filters additional minerals and also adjusts pH and electrolyte concentrations.
Number of Nephrons:
~ 1.2 million nephrons in each kidney so 2.4 million in two kidneys.
Overview of Functions
Filtration Process
Glomerular Filtration: Blood is filtered through the glomerulus, forming a filtrate that enters Bowman's capsule.
Tubular Reabsorption: Substances needed by the body are reabsorbed from the filtrate back into the blood.
Tubular Secretion: Additional substances are secreted into the filtrate from the blood.
Osmolality in the Loop of Henle
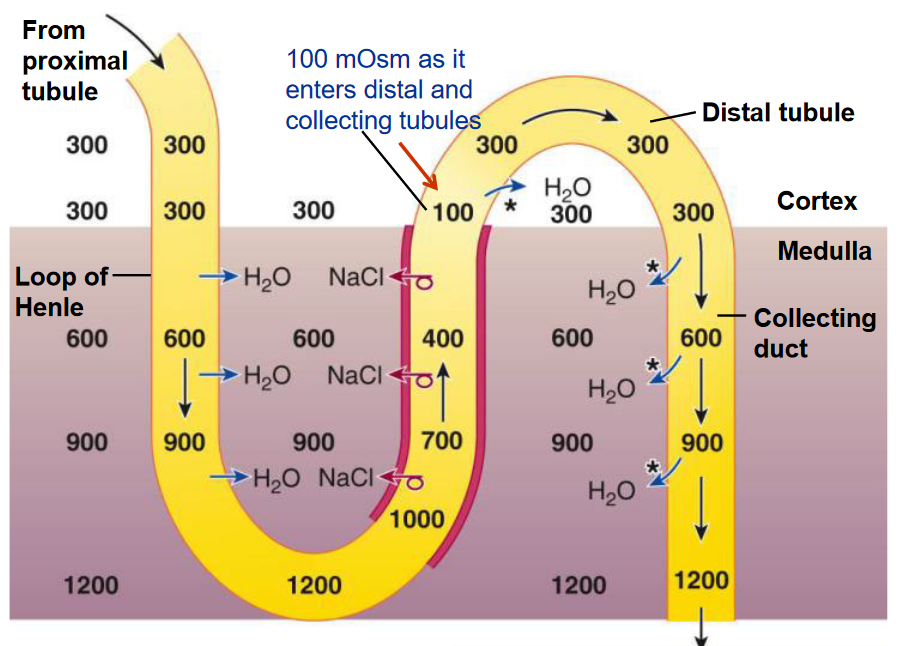
Initial Osmolality:
In the glomerulus, Bowman's capsule, and PCT, the osmolality is ~300 milliosmoles (mOsm/l). (isotonic with blood plasma)
Osmolality Changes in the Descending Limb:
Starts at 300 mOsm at the top and increases as it descends:
500 mOsm at a shallow depth,
700 mOsm at mid-depth,
900 mOsm further down,
reaches peak at 1,200 mOsm at the bottom of the loop.
As the descend, the fluid becomes hypertonic (increased solute concentration).
Osmolality Definitions
Hypertonic: High solute (NaCl) concentration, low water content.
Hypotonic: Low solute (NaCl) concentration, high water content.
Isotonic: Equal solute and water concentrations.
Mechanisms in the Loop of Henle
Countercurrent Multiplier Mechanism
Function: Establishes a gradient in osmolality in the renal medulla, enhancing water reabsorption.
Process in Ascending Limb:
Sodium Potassium 2 Chloride (Na-K-2Cl) Cotransporter: Transports sodium, potassium, and chloride ions into the cells from the filtrate.
Therefore Na & Cl are pumping out
Some K is leaking out, some is staying in
K gets repelled because there are a lot of positive chargers
Ca & mag also move paracellularly
This is why increases osmolality as going down LOH. its getting saltier
Ascending limb is impermeable to water and actively pumps out sodium and chloride, thus increasing osmolality in the renal medulla.
Water Movement: Water moves out due to the osmotic gradient established via obligatory water movement, leading to further concentration of sodium and chloride outside.
Process in Descending Limb:
Aquaporin-1 channels allow water to re-enter the renal medullary interstitial space bc it wants to dilute it. via countercurrent multiplier mechanism
The descending limb is permeable to water but completely impermeable to solutes (NaCl and other ions).
Once turns the DLOH to ALOH, osmo decreases because solutes (Na & Cl) are leaky into medullary interstitial space
The Role of Vasa recta
Definition: A branch of the peritubular capillaries within the kidney; branch of the efferent arteriole
Function of Vasa Recta= Countercurrent Exchanger:
As blood flows down, it picks up sodium and chloride ions; simultaneously, water is lost to the renal medulla, maintaining osmotic balance (sluggish flow to prevent washout of salts).
When returning, it pushes sodium chloride out and reabsorbs water, maintaining the osmotic gradient of the renal medulla.
Significance: Prevents rapid removal of sodium chloride, ensuring the medullary interstitial gradient remains.
2nd function is provides oxygen to tissue cells
Summary of Mechanisms at Work
Descending Limb:
Water is reabsorbed (permeable), solutes are retained (impermeable).
Aquaporin-1 channels facilitate water movement into the medullary interstitium.
Ascending Limb:
Sodium, potassium, and chloride ions are actively pumped out into the interstitium, making it hypertonic.
Countercurrent Multiplier Mechanism:
Water exits the descending limb while ions are secreted from the ascending limb, establishing gradients that allow for concentrated urine formation.
Vasa Recta:
Functions as a countercurrent exchanger, which aids in maintaining the medullary gradient and supplying nutrients and oxygen to renal tissues.
Distal Convoluted Tubule (DCT) Video 4/9
The distal convoluted tubule (DCT) is the part of the nephron following the loop of Henle.
Understanding the DCT requires prior knowledge of the proximal convoluted tubule and loop of Henle, so it's recommended to observe those sections first.
Overview of Mechanisms in the DCT
Two main processes occur in the DCT: tubular reabsorption and tubular secretion.
Tubular Reabsorption: The movement of substances from the kidney tubules back into the blood.
Tubular Secretion: The movement of specific solute molecules from the blood into kidney tubules.
Loop of Henle Connections
In the loop of Henle, two key segments exist: the descending limb and the ascending limb.
The ascending limb contains specialized transporters that pump sodium (Na⁺), potassium (K⁺), and chloride (Cl⁻) ions into the cells.
Basolateral membrane features channels to pump sodium out and chloride ions out, contributing to the medullary interstitium gradient.
This creates a highly concentrated interstitial fluid (salty), affecting osmolarity as follows:
Starts at 300 mOsm/L and can reach 1200 mOsm/L in the deepest renal regions.
Osmolarity and Reabsorption Percentages
Absorption percentages at various renal sites:
PCT: 65% sodium and 65% water absorption.
Descending Loop of Henle: 15% water absorption.
DCT= Remaining ~20% water entering the DCT:
25% of remaining sodium is reabsorbed in the DCT.
Ultimately, 10% sodium remains after reabsorption processes.
This is part of the countercurrent multiplier mechanism and supported by the vasa recta to prevent major loss of NaCl
Distal Convoluted Tubule Structure
The DCT can be subdivided into early DCT and late DCT.
Early DCT (10% Na remaining)
Specialized transporters in the early DCT function:
Sodium-Potassium ATP pumps move 3 sodium out and 2 potassium in, requiring ATP -bc its pumping against concentration their gradient.
High sodium concentration in filtrate draws sodium ions into the cells via sodium-chloride transporters, bringing chloride ions along with it. because of NaCL symporter (same direction)
Reabsorption Rate:
About 5-6% of sodium is reabsorbed in the early DCT. (4-5% sodium remaining)
Calcium ions also present in this section, with parathyroid hormone stimulating reabsorption when blood calcium levels are low.
Hormonal Mechanism for Calcium Reabsorption
Parathyroid hormone (PTH) is released in response to low blood calcium levels:
It activates receptors in the DCT to stimulate a second messenger system.
G stimulatory protein and adenylate cyclase, converting ATP to cyclic AMP.
cAMP further activates protein kinase A (PKA). PKA stimulates calcium channels in the luminal membrane.
Calcium is transported from the tubular fluid into the cells and then into the bloodstream.
Some calcium binds to calbindin, while the majority re-enters the blood to increase blood calcium levels.
Secondary active transport occurs where sodium moves into the cells while calcium is forced out. (ATP dependent process)
Late Distal Convoluted Tubule (DCT)
Cells in this segment respond to aldosterone, a steroid hormone from the adrenal cortex:
Stimulated by factors including angiotensin II, low sodium, and high potassium levels; and small amounts of corticotropin-releasing hormone.
Aldosterone stimulates gene expression leading to the formation of proteins involved in sodium and potassium transport (Na/K):
Proteins allowing sodium influx (increased blood sodium and decreased potassium), promoting excretion into the urine.
ADH (antidiuretic hormone) MAKES LATE DCT permeable to water via aquaporin channels to follow Na, increasing reabsorption and thus blood volume and pressure.
Key Drug Interaction
Thiazide Diuretics: These medications inhibit the sodium-chloride co-transporters (symporter), affecting sodium and water reabsorption, leading to diuresis.
Intercalated Cells, and Collecting Ducts Video 5/9
Principal Cells: Principal cells are specialized epithelial cells that play a crucial role in balancing mineral and water levels in the body. They are responsible for regulating water reabsorption and sodium/potassium exchange.
Functions:
Maintain mineral balance.
Regulate water balance.
Intercalated A and B Cells
Function: Intercalated cells primarily function in maintaining acid-base balance in the body.; intercalted cells are found in late DCT and CD
Intercalated A Cells (for Acidosis)
Conditions Managed: These cells respond to conditions of acidosis, including respiratory and metabolic acidosis.
Mechanism:
High levels of CO₂ in blood enter the intercalated A cells and react with water in the presence of carbonic anhydrase to form carbonic acid (H₂CO₃).
Carbonic acid dissociates into bicarbonate (HCO₃⁻) and protons (H⁺).
Increased protons lead to lower pH (acidosis). The bicarbonate serves as a weak base, neutralizing the protons.
A specific channel protein facilitates the exchange of protons and potassium ions, requiring ATP:
Protons exit the cell, while potassium ions (K⁺) enter, which requires ATP.
This process is ATP-dependent, aimed at buffering the blood pH.
Ammonia (NH₃) secretion occurs in acidosis, where ammonia can bind to protons that were pumped out to form ammonium (NH₄⁺), a weak acid that contributes to urine acidity and aids in buffering.
Bicarbonate Transport: Bicarbonate ions exit through the basolateral membrane into the bloodstream, raising pH back to normal.
Chloride ions enter the cells to maintain ionic balance due to bicarbonate’s exit.
Intercalated B Cells (for Alkalosis (Basic conditions)
Conditions Managed: These cells respond to alkalosis, including metabolic and respiratory alkalosis.
Mechanism:
CO₂ enters the cell and combines with water to form carbonic acid via carbonic anhydrase.
Bicarbonate is transported out of the cell, contributing to the urine and decreasing bloodstream bicarbonate levels.
Chloride ions enter the cells to maintain charge balance as bicarbonate exits.
Protons are reabsorbed into the blood, assisting in lowering the pH to homeostatic levels, which requires ATP for transport processes.
Antidiuretic Hormone (ADH) and its Action
Function: ADH (also known as vasopressin) primarily regulates the kidney’s ability to reabsorb water and maintain blood volume and pressure.
Mechanism of Action:
Stimuli for Release: ADH is released when plasma osmolality increases or in response to angiotensin II, indicating a need to conserve water.
It binds to specific vasopressin receptors on principal cells in the collecting ducts and late distal tubules, activating the G-stimulatory protein, which in turn stimulates adenylate cyclase.
cAMP Production: The activation of adenylate cyclase converts ATP into cyclic AMP (cAMP), l/t activation of protein kinase A (PKA).
PKA promotes the fusion of vesicles containing aquaporin-2 channels via phosphorylation with the luminal membrane, increasing water permeability and allowing water to flow from the renal tubules, aquaporin 3 & 4 channels into the bloodstream.
As water reabsorbs into the bloodstream, blood volume and pressure increase while plasma osmolality normalizes, returning to isotonic levels (~300 mOsm).
20% of water remaining depends on ADH; Calcium relies on PTH; Remaining 4-5% of Na depends on aldosterone
Collecting Duct Functions
Secretion Processes:
Collecting ducts can also secrete various substances: drugs, toxins, creatinine, ammonia, protons, and bicarbonate, contributing to the fine-tuning of blood chemistry.
Counter-Current Exchange Mechanism and Vasa Recta
Role of Vasa Recta: Specialized capillary network that runs parallel to nephron tubules.
It helps maintain the osmotic gradient in the medulla, essential for water reabsorption.
Prevents rapid NaCl removal (starts 300 osm→ ends in 325 osmo) while providing oxygen to renal tissues with its slow blood flow.
Importance: Contributes to urine concentration and the medullary interstitial gradient, facilitating obligatory water movement out of nephron structures into the bloodstream.
Urea Recycling
Urea aids in creating a hyperosmotic environment in the medullary interstitial space through urea recycling:
After water reabsorption in the collecting duct, urea concentration rises, leading to its passive diffusion into the interstitium and aiding in maintaining osmolarity (urea= solutes).
Contributes to the generation of concentrated urine & contribute to medullary gradient, vital for bodily homeostasis.
Filtration, Reabsorption, and Secretion Overview (Video 6/9)
Glomerular Filtration Process
Afferent Arteriole:
Brings blood to the glomerulus.
The glomerulus is a network of capillaries that performs filtration.
**Filtration Pressures: **
Glomerular hydrostatic pressure - pressure from systemic blood pressure pushing fluid out into the Bowman's capsule.
Osmotic pressure - exerted by proteins in the blood that pull water back into the bloodstream.
Capsular hydrostatic pressure - pressure exerted by the filtrate in the capsule pushing fluid back into the glomerulus.
Capsular osmotic pressure - typically zero as plasma proteins like albumin should not filter through.
Net Filtration Pressure (NFP):
The overall result of the pressures involved; approximately 10 mmHg.
Glomerular Filtration Rate (GFR):
Directly proportional to NFP.
Normal GFR is about 125 mL/minute.
Nephron Structure
Definition: Nephron = Glomerulus + Bowman's capsule + PCT + LOH + DCT.
Nephrons in Kidney: Approximately 1.2 million per kidney → 2.4 million in two kidneys (unless renal agenesis occurs).
Proximal Convoluted Tubule (PCT)
Major site of reabsorption.
Substances reabsorbed include:
Sodium: ~65% reabsorbed; water follows due to osmotic gradient.
Bicarbonate: ~85-90% reabsorbed; depending on body needs.
Potassium: ~60% reabsorbed.
Chloride: ~50-60% reabsorbed.
Calcium: ~60% reabsorbed.
Magnesium: Varied depending on sources, but questionable.
Urea: ~50% reabsorbed; contributes to osmotic gradient.
Glucose & Amino Acids: 100% reabsorbed under physiological conditions (dependent on sodium).
Transport Mechanisms:
Sodium-glucose co-transporters bring glucose into the blood.
Small proteins (e.g., albumin, insulin) reabsorbed by endocytosis.
Lipids passively diffuse through the membrane.
Tubular Secretion
Defined as the process of moving substances from blood into the filtrate.
Substances Secreted:
Drugs and metabolic wastes (e.g., ammonium, creatinine).
Requirement of ATP: Useful for pumping protons and other substances depending on ATP.
Loop of Henle
Osmolality Changes: As filtrate descends, osmolality increases from 300 mOsm/kg to 1200 mOsm/kg.
Descending limb allows water reabsorption; impermeable to solutes.
Ascending Limb Characteristics:
Sodium-potassium-chloride co-transporter responsible for moving solutes out (~25% sodium, ~30% potassium, ~30% chloride).
Contributes to medullary interstitial gradient facilitating countercurrent multiplication.
Distal Convoluted Tubule (DCT)
Two parts: Early and Late distal tubule.
Early DCT: Sodium and chloride reabsorption through specific transporters.
Hormonal Regulation: Influenced by PTH activating cAMP pathways affecting calcium reabsorption.
Late DCT:
Aldosterone: Promotes sodium reabsorption and potassium secretion through its action on sodium-potassium pumps.
Stimulated by low sodium or high potassium levels.
Antidiuretic hormone (ADH): Increases aquaporin expression in collecting duct to concentrate urine and increase blood volume.
Collecting Duct
Final adjustments to urine composition:
Urea Recycling: Contributions lead to concentrated urine and maintain osmotic gradient.
ADH enhances water reabsorption.
Metabolic Regulation: Intercalated cells function in acid-base balance during acidosis (A cells) and alkalosis (B cells).
Conclusion and Key Metrics
Remaining Filtrate Composition:
Water: ~20% (variable based on ADH).
Sodium: ~5%-10% (dependent on aldosterone).
Calcium: Reabsorption dependent on parathyroid hormone.
Overall, these mechanisms ensure fluid, electrolyte regulation, and acid-base balance in the body.
Note: Key hormone influences and physiological implications in renal function are highlighted throughout each nephron structure.