Unit 4 - The Immune Response
Briefly characterize nonspecific defense and innate mechanisms and how they differ from the specific immune response or adaptive immunity
Cells sloughed from skin and mucous membranes routinely to remove foreign organisms
Slightly acidic pH which prevents growth of some organisms
Mucus secreted by digestive, urogenital and respiratory tracts = protective coating
Cilia = move foreign particles out of the respiratory tract
Cough mechanism = expel material (foreign particles) forcefully
Lysozomes (tears), acid (stomach) and digestible enzymes also help
Inflammation = nonspecific defense mechanism
neutrophils, macrophages, phagocytes = non-specific phagocytosis
Macrophages = important in both immune response
Major components = pattern recognition receptors that detect extracellular pathogens that display pathogen-associated molecular patterns
structural motifs that initiate immune responses
Release damage-associated molecular patterns
motifs released by dying or damaged cells
The ADAPTIVE response is specific
Memory = antigen is remembered and recognized
Amplification = Enhanced secondary response on second exposure to antigen
Antigen = molecules that evoke an antibody response
large molecules (protein or polysaccharide)
Haptens = become antigenic if they complex with larger carrier molecules
Foreign agent = bacteria, viruses, protozoa and funghi
binding of hapten/neoplastic transformation ( becoming cancerous) can show up as foreign bodies
Immunogen = molecules that elicit an immune response
Self-tolerance = natural tolerance or lack of response to one's own antigens
clonal deletion = during embryonic development lymphocytes go through a selection procedure in the thymus (those reacting to self-tolerance molecules are deleted
Describe the origin and generation of both B (humeral immunity) and T lymphocytes (cell-mediated immunity), their functions and the different classes of T lymphocytes
When an antigen enters the body it is
Processed by antigen-presenting cells such as dendrites
Presented to lymphocytes (major effector cells of immune system)
Lymphocytes then proliferate and transform
T CELLS = Cell-mediated immunity
transform into effector (Killer T cell) which destroy antigen-bearing cells
Lymphokines produced and influence interaction between cells
Helper and suppressor cells enhance and suppress the immune response
Characterized by T-cell receptor complex on the surface
interact with specific fragments of antigens that have been
digested through phagocytosis and present on surface
expressed abnormally (viral and tumor cells)
After interaction clonal expansion occurs
CD4 (60% mature T cells)
helper T cells which secrete cytokines
TH1-lymphocytes respond to activation through release of Interferon-Gamma
activates macrophages and B-cells
secrete antibody isotopes that mediate phagocytosis + activate complement
TH2-lymphocytes release IL-4
stimulates B cells to differentiate to IgE secreting plasma cells
IL-5 and IL-13 also released
activates mast cells and eosinophils
Produces a reaction resembling Type I hypersensitivity response
CD8 (30%)
cytotoxic = directly kill virus-infected cells/tumour cells
Lesser role in secretion of cytokines
Role of Activated T cells
Cell-mediated immunity
Cytotoxicity = direct killing of cells which is important in CD8 + T-cells
Kill any cell with a recognizable surface antigen (virus + transplanted + tumor)
Helper roles (regulation of B and T cell activity
produce cytokines (protein mediator) which influence functions of macrophages and lymphocytes
Help to synthesize B cells
Delayed hypersensitivity
B CELLS = Humoral Immunity
humoral immunity = transformation of B cells into antibody-producing plasma cells (antibodies = immunoglobulins)
Characterized by antibody-receptor complex on cell surface (interaction causes proliferation) and clonal expansion
Antibody/Antigen interaction causes clonal expansion (B-cell proliferation)
Plasma Cells = produce and secrete antibody that is specific for the antigen that originally triggered their differentiation
off-center nucleus + cartwheel chromatin pattern + abundant basophilic cytoplasm + obvious perinuclear clearing
IgG, IgM, IgA, IgE and IgD
Memory cells = smaller population but persist longer
provide B-cells that react to antigens and invoke a rapid immune response (MEMORY B CELLS)
Natural Killer Cell = INNATE LYMPHOCYTE
what are 3 features of NK cells?
Antigen - Presenting cells
Macrophages = derived from blood monocytes
Found in all tissues, concentrated in lymphoid tissues
Macrophages play a key role in early immune response
ANTIGEN PROCESSING ROLE
phagocytosis and internalization of Ag by macrophage
Ag is expressed a the macrophage surface with MHC molecules
Cell Type | FUNCTION |
|---|---|
Antigen Presenting Cells | |
Macrophages |
|
Interdigitating Dendritic Cells |
|
Follicular Dendritic Cells |
|
B-Cell Lineage | |
B-Cells/Memory Cells |
|
Plasma Cells |
|
T- Cell Lineage | |
CD8+ T Cells |
|
CD4+ T cells |
|
Other Types | |
Natural Killer Cells |
|
Describe antibody production by B cells and the immunoglobulin classes
After antigen recognition, activation, and presentation to the B-cell the antibody, B cells proliferate and differentiate
antibodies are then secreted from plasma cells and bind to and neutralize microbes
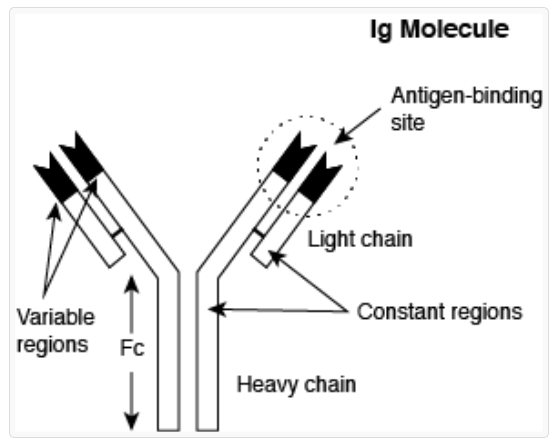
Immunoglobulins = a family of serum proteins (antibodies)
Immunoglobulin structure
heavy and light chains which each have variable and invariable sequences
Constant part is the same in all members of similar Ig class (white)
Variable = variable in amino acid sequences and gives antigen specificity
ANTIBODY PRODUCTION
Lymphocytes are derived from steel cells in bone marrow
those which migrate and develop further in the thymus = T lymphocytes
those that develop independently from the thymus (they develop in the bursa of Fabricius in birds or BONE MARROW) = B cell
From bone marrow, they travel to peripheral lymphoid tissues (lymph nodes, spleen, tonsils, gut, and mucosal)
Development of Antibodies
newborns rely on passively acquired IgG through the placenta in utero
In the first few weeks of life, lymphoid tissue develop and immunoglobulins are produced (synthesized at different rates)
age 3-4 months = lowest immunoglobulin levels (maternal levels decrease, actively produced antibodies are low
colostrum = source of antibodies
Describe the components of the adaptive immune response including antigens, antibodies, B and T lymphocytes, agglutination, opsonization and complement fixation and their interactions with each other and macrophages
Within lymph nodes the antigen is processed by macrophages and presented to T and B cells leading to T cell transformation
T cell → activated T cell, B cell → plasma cell
antibody secreted into lymphatic vessels and leave the node, entering blood plasma through the thoracic duct
stimulation of lymph node = enlargement (reactive or hyperplastic nodes)
T and B cells = arranged in follicles
Agglutination
formation large aggregates or clumps of Ag and Ab
occurs because the two binding sites on antibody molecules cross-link a number of antibody and antigen molecules
Makes it easier for phagocytes to trap and consume
Neutralizes toxin
Opsonization
coating antigen with antibody = increased phagocytosis by leukocytes with receptor for antibody
Immune phagocytosis seen in unit 3
Complement Fixation
outcome of complement activation
Complement = system of 9 plasma proteins (C1-C9) which similar to the clotting cascade, react sequentially
C56789 or MAC punches holes in cell membranes due to phospholipase activity
Ag/Ab complex initiates complement cascade = formation of cytotoxic complex and lysis of the cell
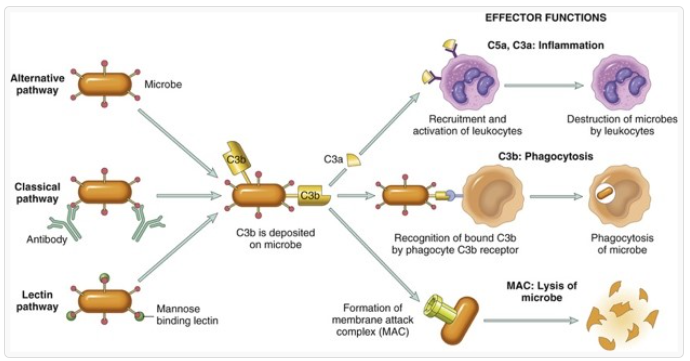
NOTE: Complement is also associated with the inflammatory response
C3a and C5a contribute to vasodilation and increased permeability + chemotactic for neutrophils
C3b acts as opsonin = inducing immune phagocytosis by neutrophils and macrophages
Agglutination + opsonization occur when the antigenic stimulus is cellular
Macromolecule = Ag and Ab complexes form a larger macromolecular complex for easy phagocytosis
The formation of immune complexes in vivo lead to:
inactivation of the antigen or lysis if cellular
phagocytosis of the antigen by scavenger cells
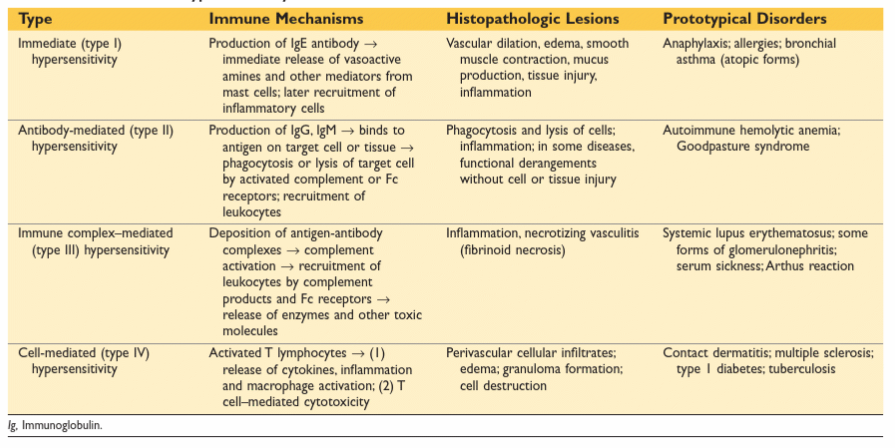
Outline the mechanisms of the four types of hypersensitivity reactions and give clinical examples of each
Hypersensitivity = state of reactivity in which the immune response leads to tissue injury
Type of Hypersensitivity | Disorder of disease | Immune Mechanism and Cells Involved | Lesion |
|---|---|---|---|
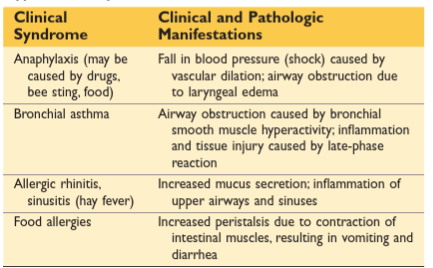
Type I - Immediate | Localized = Hay Fever/Irritating allergies/Asthma
Systemic = Anaphylaxis
| Release of mediators from mast cells which are activated by cross-linking of IgE bound to surface by Fc receptors
| Vascular dilation, edema, |
Type II - Antibody Mediated | Localized = Auto-immune diseases Systemic = | ||
Type III - Immune Complex Mediated | Localized = Arthus reaction
Systemic = Serum sickness
| ||
Type IV - Cell-mediated |
TYPE I
Primary vasoactive mediators
released from mast cell granules and responsible for early events of Type I Hs
Secondary generated lipid mediators
activated of phospholipase A which acts on mast cell membrane phospholipids to produce arachidonic acid and metabolites
Increase vascular permeability and chemotactic effects
Cytokine synthesis
secreted cytokines and chemokines released from mast cells recruit + amplify the response (result in recruitment of inflammatory cells + eosinophils and neutrophils)
Describe the sequence of events that occur in a sensitive individual both on first exposure and on subsequent exposure to the antigen?
First exposure to allergen
Activation of TH2 cells and IgE class switching in B cells
Production of IgE
Binding of IgE to FceRI on mast cells (receptor)
Repeat exposure to allergen
Activation of Mast cell, release of mediators
Vasoactive amines, lipid mediators
immediate hypersensitivity reaction
Cytokines
late phase reaction (2-4 hours)
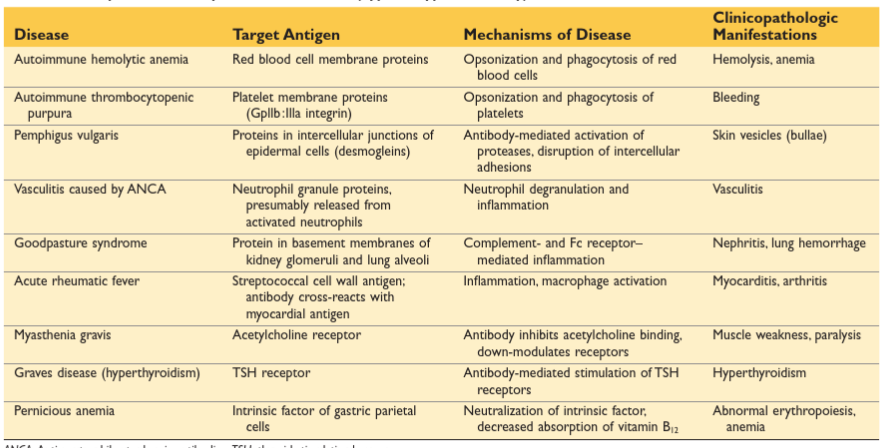
TYPE II
Opsonization and Phagocytosis
coated with Ab are opsonized (more susceptible to phagocytosis)
Body mistakes normal cell surface component as foreign and reacts against self-antigen
Inflammation
antibodies activate complement system
products recruit neutrophils and monocytes + trigger inflammation in tissues
Antibody-Mediated Cellular Dysfunction
antibody is formed against cell surface molecule or receptor, inhibiting/stimulating cell function without necrosis
Myasthenia gravis = antibodies formed to acetylcholine receptors, binding and rendering non-functional
Graves = bind to TSH receptor and stimulate the release of thyroid hormones
TYPE III
Ab/Ag interaction forms intravascular immune complexes that are deposited in walls of small vessels
Fibrinoid necrosis of small vessels (Acute vasculitis)
Formation of immune complexes
Deposition of immune Complex
Immune complex-mediated inflammation and tissue injury
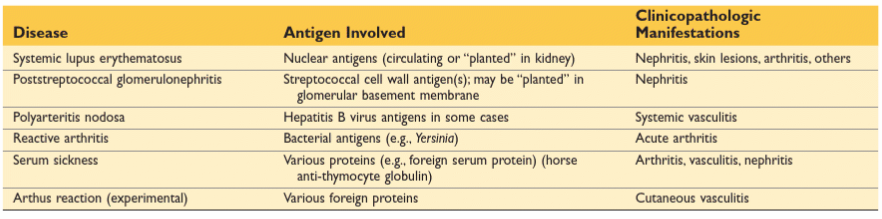
Type III causes tissue injury because of the recruitment of neutrophils. Phagocytosis of immune complexes by neutrophils leads to?
Immune complex-mediated inflammation and tissue injury
depletion of opsonized cells
Why do most forms of Type III hypersensitivity take several days to become clinically apparent?
takes about 1 week after protein antigen is injected for it to trigger an immune response and the production of antibodies
What are the favored sites for immune complex deposition?
Organs where blood is filtered at high pressure to form other fluids (during and synovial fluid) , glomerulus, and joints
Describe what causes tissue injury following immune complex deposition.
complement activation and engagement of leukocyte c receptors
Type IV
mediated by T cells:
directly cytotoxic
secrete cytokines which recruit other cells and cause injury
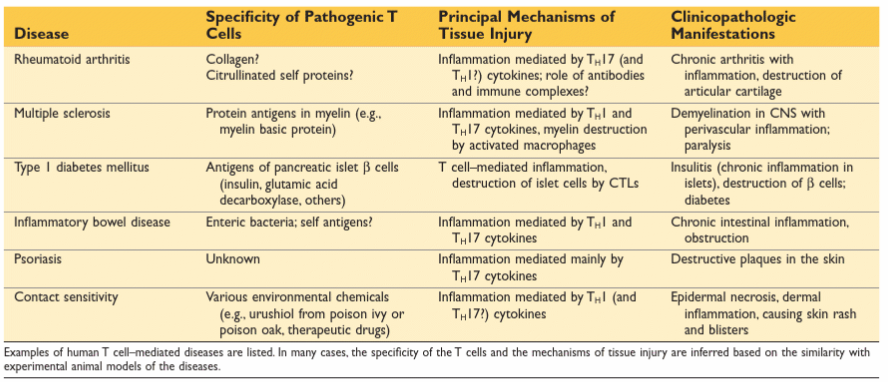
Delayed-type hypersensitivity is characterized by the presence of?
CD4+ T cells (cytokine-mediated inflammation)
CD8+ T cells (direct cell cytotoxicity)
Poison ivy dermatitis is a good example of delayed hypersensitivity/ What would happen when a sensitive person undergoes first and second exposure?
1st = alters self-proteins and neoantigens are recognized as foreign by T cells
What is the main cytokine responsible for the development of DTH response?
CD4 _ T cells → IFN gamma
Differentiate the concepts of self-tolerance, passive and active immunization, primary and secondary immune response
Self Tolerance
Passive Immunization
Transfer of pre-formed antibody from one person to another (temporary and useful for emergency treatment)
Transplacental Immunity = natural acquisition of antibodies across the placenta in utero
Colostral Immunity = acquisition of antibodies through colostrum
Therapeutic Immunity = medical administration of antibodies against particular agent, toxin, or byproduct to an individual that is known or suspected to have been exposed
Active Immunization
Development of antibodies in response to an antigen
Vaccination = artificial active immunization
inactive form/altered pathogen is used
has antigenicity but not pathogenicity
Vaccine acts as primary exposure
Serology = study of antigen-antibody reactions in lab setting
test for antibodies in a patient’s serum
Titer = dilution at which Ag/Ab reactivity still occurs
Serologic tests used to aid in diagnosis of certain infectious diseases = systemic fungal infections, bacterial infections and viral diseases (measured to determine adequacy of response to vaccine)
Primary Immune Response
occurs following first exposure to antigen
lag period between entrance of antigen into body and antibody appearance in the bloodstream
B cells with receptors for that antibody undergo clonal expansion
IgM first, followed by IgG and other immunoglobulins
Secondary Immune Response (Anamnestic response)
Accelerated response (no lag period)
memory = increases response time
Principal immunoglobulin secreted is IgG (peak is higher and decline is slower than primary response)
Describe how the immune system is involved in transplant rejection, autoimmune diseases and immunodeficiency syndromes
Allograft = graft of tissue between two individuals of the same species with different genotypes
Histocompatibility = function to bind peptide fragments of foreign proteins for presentation to appropriate antigen-specific T-cells
RBC antigens need to be considered
Nucleated cell antigens (HLA/histocompatibility antigens)
coded for my MHC (major histocompatibility complex) or chromosomal site containing histocompatibility genes
Class I = found on all tissues
Class II = restricted (presented on antigen-presenting cells)
Note the polymorphism at major HLA loci (each individual expresses a unique MHC antigen profile)
T-Cell mediated rejection
Describe how Type IV hypersensitivity (DTH and CTL leads to classic acute rejection)
CTL’s directed against histocompatibility antigens
CD8+ CTLs kill antigen-expressing target cells
Antibody-Mediated
How does hyperacute rejection differ from acute antibody-mediated rejection?
Hyperacute = mediated by preformed antibodies specific for antigens on graft endothelial cells
Acute = mediated by T cells and antibodies that are activated by alloantigens in the graft
acute antibody = antibodies bind to vascular endothelium and activate complement via classical pathway
What characterizes chronic rejection and how does it differ from acute rejection?
Chronic = indolent form of graft damage that occurs over months or years
manifests as interstitial fibrosis and narrowing of graft blood vessels
T cells apparently react against graft alloantigens and secrete cytokines
Autoimmune Diseases
Develops because the clonal deletion phase in embryonic development is somehow faulty so an individual is born with clones of lymphocytes capable of reaction against normal tissue components
Normally suppressor T cells suppress the clones of lymphocytes for self-antigens
ANERGY = inactivation of lymphocytes that is induced by exposure to antigens under certain conditions
How does immunologic tolerance differ from self-tolerance?
Self-tolerance = lack of immune responsiveness to one’s own tissue antigens
Immunologic tolerance = unresponsiveness to an antigen that is induced by exposure of antigen-specific lymphocytes
When do autoimmune diseases develop?
What are the principle mechanisms for inactivation of T cells in central and peripheral tolerance?
Central tolerance = antigen-induced deletion of self-reactive T lymphocytes and B lymphocytes during maturation in central lymphoid organs
Peripheral tolerance = Anergy (functional inactivation of lymphocytes that is induced by an encounter with antigens under certain conditions)
Suppression by regulatory T cells (the ones responsible for preventing self-reactions)
Deletion by apoptosis
What is molecular mimicry?
Viruses and other microbes might share cross-reacting epitopes with self-antigens
Responses indeed by the microbe may extend to self-tissues
Primary Immunodeficiency
Inherited genetic disorders that impair mechanisms of innate immunity (phagocytes, NK cells, or complement) OR humoral and cellular arms of adaptive immunity
SCID = group of genetically distinct syndromes that show defects in both humoral and cell-mediated immunity
What age group is primarily affected by SCID and why?
infants present with thrush and severe diaper rash
maternal T cells transferred across the placenta and attack the fetus
SCID is due to impairment of what cell types? How does this differ from defects of innate immaturity
impair the development of mature T lymphocytes and or B lymphocytes
defects in humoral and cell-mediated immunity
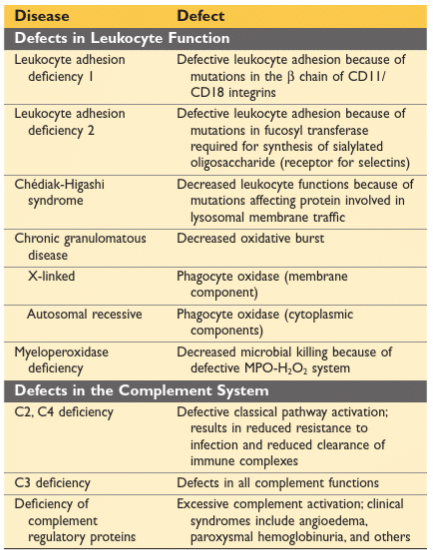
Innate Immunity Defects = affect leukocyte functions or complement system and lead to increased vulnerability to infections
Leukocyte adhesion deficiencies
Chronic granulomatus disease
Secondary Immunodeficiency
occur more frequently than primary immunodeficiencies
AIDS
retrovirus enters cell, RNA is transcribed into DNA via reverse transcriptase
Viral DNA integrated into cellular DNA
IMMUNOSUPPRESSION
CDR+T cells as well as macrophages and dendritic cells
anything that promotes T cell activation will promote the death of HIV-infected cells
CD4+ loss = defining characteristic of AIDS
death of CDR+ leads to increased susceptibility to viruses, fungi, protozoa and some bacteria
Early acute = self-limited illness (virus-specific immune response)
chronic phase = HIB is positive but few signs of disease (viral replication continues in lymphoid tissues)