Pupil Anomalies - Part 1
Pupil Anomalies
Assessment of the pupils is a key part of an examination.
Pupil anomalies may signify the presence of significant ocular or neurological pathology.
May indicate dysfunction in:
Iris
Optic nerve, retina
Anterior visual pathways
Parasympathetic innervation (third nerve – iris sphincter) to the eye
Sympathetic innervation (iris dilator) to the eye
Revision: Afferent and Efferent Pathways
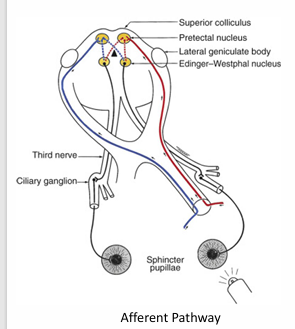
Afferent Pathway:
Optic Tract: Input from homonymous hemiretinas.
Pretectal Nucleus.
Efferent Pathway:
Parasympathetic Pathway:
Edinger-Westphal nucleus.
Oculomotor nerve (ACh "preganglionic neuron").
Ciliary ganglion (ACh "postganglionic neuron").
Short ciliary nerves.
Iris sphincter pupillae.
Sympathetic Pathway:
Hypothalamus (Arousal!).
Cilio-spinal center (Budge) (C8-T₁).
Cervical sympathetic ("preganglionic neuron").
Superior cervical ganglion (ACh "central neuron").
Carotid plexus.
Ophthalmic nerve.
Long ciliary nerves ("postganglionic neuron").
Iris dilator iridis.
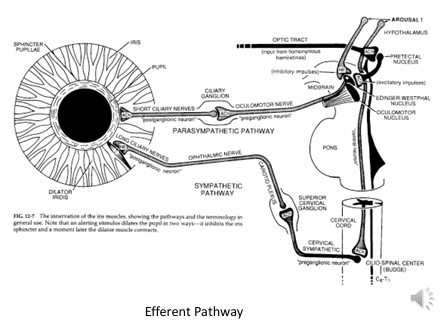
Alerting stimulus dilates the pupil in two ways:
Inhibits the iris sphincter.
Dilator muscle contracts.
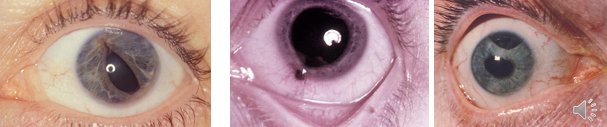
Pupil Shape and Position Anomalies
Shape: Dyscoria.
Position: Corectopia.
Causes:
Coloboma.
Tumours.
Trauma (including surgery).
ICE syndrome.
Angle dysgenesis.
Anterior segment inflammation.
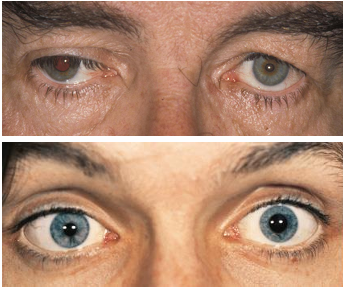
Unequal Pupils: Anisocoria
Physiological (20% of the population).
3rd Nerve paralysis, Adie’s tonic pupil, Horner’s syndrome.
Abnormal Reactions
Lesions of the afferent pathway (not usually associated with anisocoria).
Lesions of the efferent pathway (associated with anisocoria).
Pupil Assessment
Observe size, shape, and reactions of the pupils.
Are the pupils round and in the right place?
Are they equal in size?
Are the pupil reactions to light and near brisk and well-sustained?
Are reflexes equal between eyes?
Is there an afferent pupil defect?
Normal Findings
Normal light reflex is initial constriction followed by small secondary dilatation, and then stabilization of pupil size.
Pupil size is dynamic.
Pupillary unrest (small changes) seen in all normal individuals representing dynamic equilibrium between parasympathetic and sympathetic systems.
Exaggerated unrest is termed hippus (not pathologically significant).
No clinical condition where light reflex is present and near reflex is absent.
Light-near dissociation: Abnormal or absent light reflex and intact near response.
Pupils of premature infants may not react well.
Pupils of full-term infants slightly miotic, reactions present but probably less extensive than in adolescence.
Pupils larger in adolescence or early adulthood, smaller with old age.
Relative Afferent Pupillary Defect (RAPD, Marcus-Gunn pupil)
An objective sign of an asymmetric lesion in the afferent pathway (retina, optic nerve, chiasm, or optic tract).
Most commonly due to unilateral optic nerve disease.
RAPD seen with major retinal lesions or neurological lesions of the optic nerve and anterior visual pathway.
If chiasm or optic tract lesions are suspected, hemianopic pupil reactions can be searched for by stimulating homonymous and heteronymous halves of the retinae.
Opacities (e.g., cataract, vitreous hemorrhage) do not produce RAPD.
Presence of RAPD in absence of gross ocular disease indicates neurological lesion.
Absence of an RAPD can either mean that both optic nerves are healthy or that both optic nerves are equally diseased.
RE ON disease - stimulate light into the good eye, the pupil eye and fellow eye will constrict due to consensual response. If you move the light to the troublesome eye, both eyes will dilate, despite light shinning in.
Detecting RAPD
Detectable by Swinging flashlight test.
Dilatation when illumination transferred rapidly from normal to affected eye.
Swinging flashlight test very sensitive, present even in absence of reduced acuity.
Difference in extent of direct and consensual response in same eye.
e.g., pupils constrict more for Right direct and Left consensual than for Left direct and Right consensual (in a Left RAPD).
Patient with RAPD may also notice brightness difference.

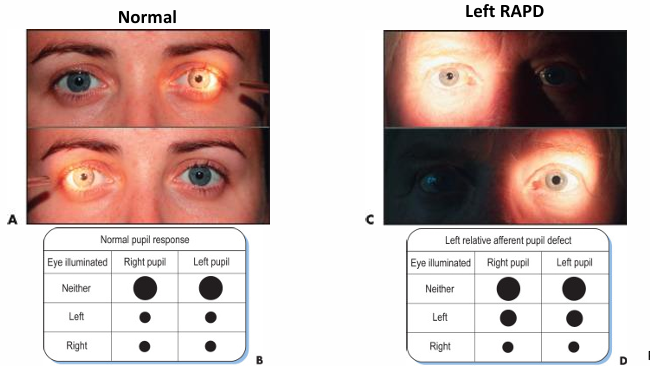
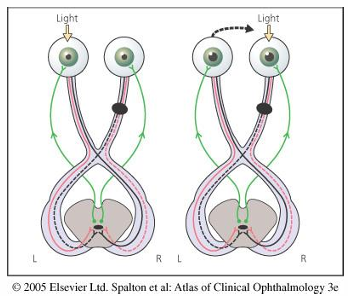
Swinging Flashlight Test
Normal pupil response:
Both pupils constrict when either eye is illuminated.
Left RAPD:
When light is shone into the left eye, both pupils constrict.
When light is rapidly transferred to the right eye, both pupils dilate.