Derm: Bello
PH508 Non-Prescription Dermatology
Learning Objectives
Describe anatomy, pathophysiology, and immunology of the integumentary system
Assess patients presenting with self-limited skin disorders
Recommend appropriate non-Rx medications for treatment/prevention of self-limited skin disorders
Pharmacy & Skin Dx
Skin dx: low mortality
Treatments: OTC Skin Care
Community Pharmacists Provide:
Patient access & Facilitate (effective) self-care
Skin Structure and Function
Integumentary System
An organ system consisting of skin, hair, nails, and exocrine glands
Largest organ
Waterproof
Protects deeper tissues
Excretes wastes
Regulates body temperature
‘Sense’ organ
Layers and Structures of the Skin
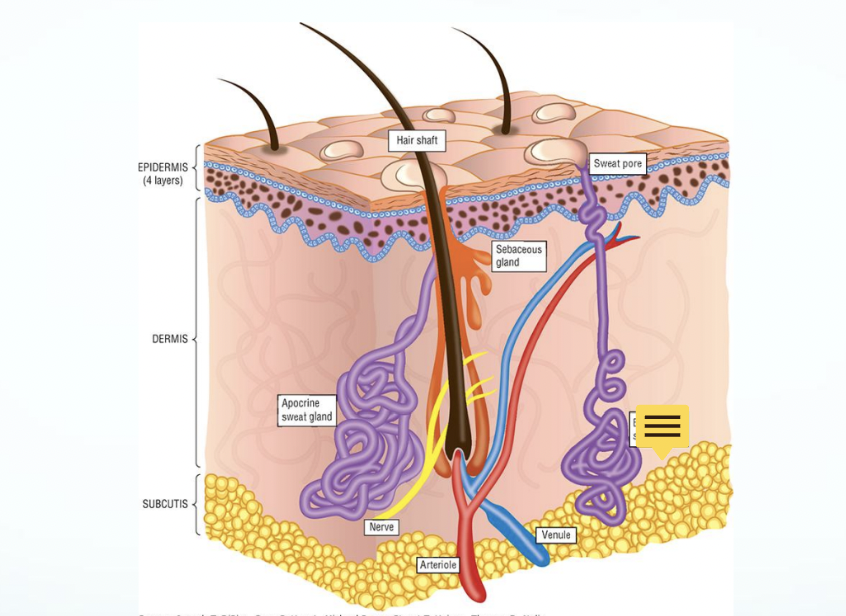
Subcut → Dermis → Epidermis
Psoriasis & Acne occur on the top layer on the epidermis*
A macule is a small, flat, and discolored spot on the skin that is typically less than 1 centimeter in diameter. It is characterized by a change in color or pigmentation, but does not involve any elevation or depression of the skin surface. Macules can be caused by various factors such as skin infections, allergic reactions, or certain skin conditions.
Structure of the Epidermis
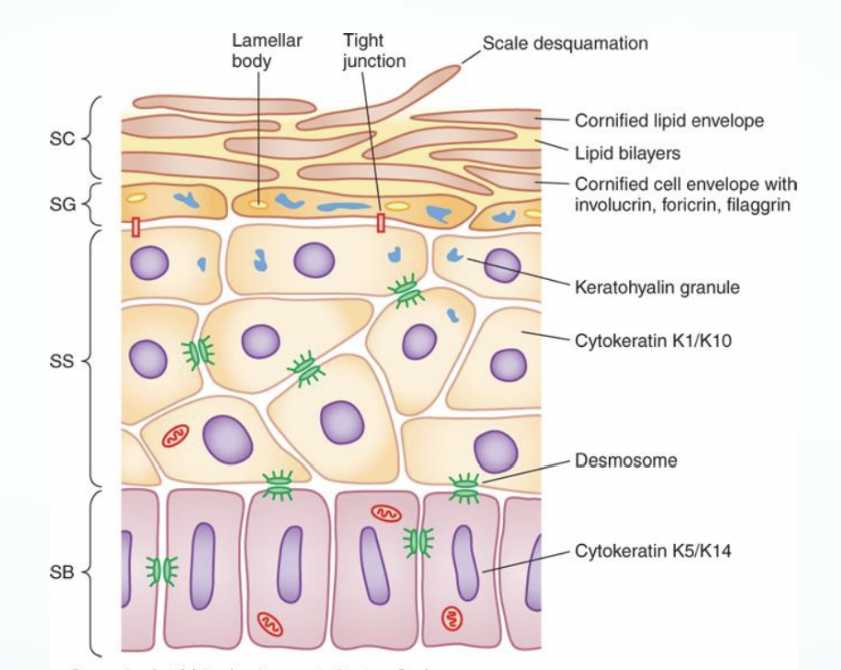
The epidermis matures progressively from the stratum basale (SB) to the stratum spinosum (SS), stratum granulosum (SG), and stratum corneum (SC)
Important structural and metabolic proteins are produced at specific layers of the epidermis
The cornfield lipid envelope, lipid bilayers, & cornfied cell envelope with Involucrin, foricrin, filaggrin
Important for the vehicle
TOP
stratum Corneum (SC)
stratum Granulosum (SG)
stratum Spinosum (SS)
stratum Basale (SB)
BOTTOM
“Come Get Sun Burnt”
Pharmaceutics
Skin normally acidic
"acid mantle" → helps repel bacteria and fungus
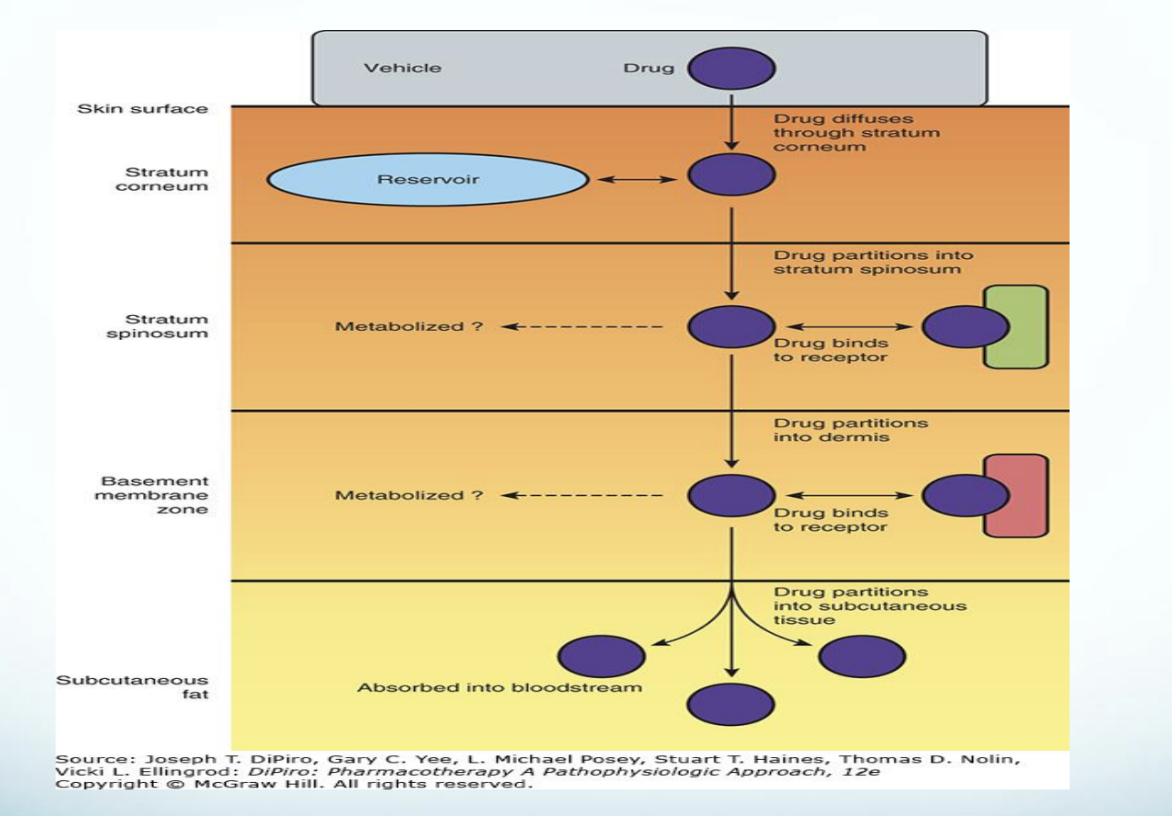
Key points – Absorption
Rates vary by anatomical skin sites
Lipophilic drugs absorbed faster due to lipid bilayers*
Occlusion affects absorption
Factors Influencing Drug Absorption through the Skin
Age-Related Skin Differences
Pediatric skin; Thinner
Barrier function not intact in pre-term baby
Potential for drug toxicity
Thinner skin → rapid absorption → potential for toxicity → new born babies
Systemic absorption
Absorbs topical drugs faster than adults*
Geriatric skin; Drier, Thinner, MORE Fragile
Prolonged healing time
Skin Care Basics
Skin health related to overall health
Nutrition
Fluid intake
Skin 10%-20% water by weight
If below then cracks form in skin (inflammation)
Skin hydration
Fragrance-free moisturizers
Bathing in lukewarm water
Non-soap cleansers
Minimize astringents and alcohol-containing products
Skin Assessment: Lesions
Macules: FLAT, distinct, discolored
Vesicles: small, fluid-filled sac
Bulla/Bullae: large, fluid- filled sac ; larger than vesicles
Caused by diaper dermatitis or severe rash, chickenpox, poison ivy
Papules: small, raised, solid bump
Nodules: small, solid, and abnormal growth or lump
Plaque: thick, sticky, or flaky layer
caused by buildup of substances such as dead skin cells, oils, and bacteria that accumulate on the surface of the skin.
Can lead to acne & psoriasis
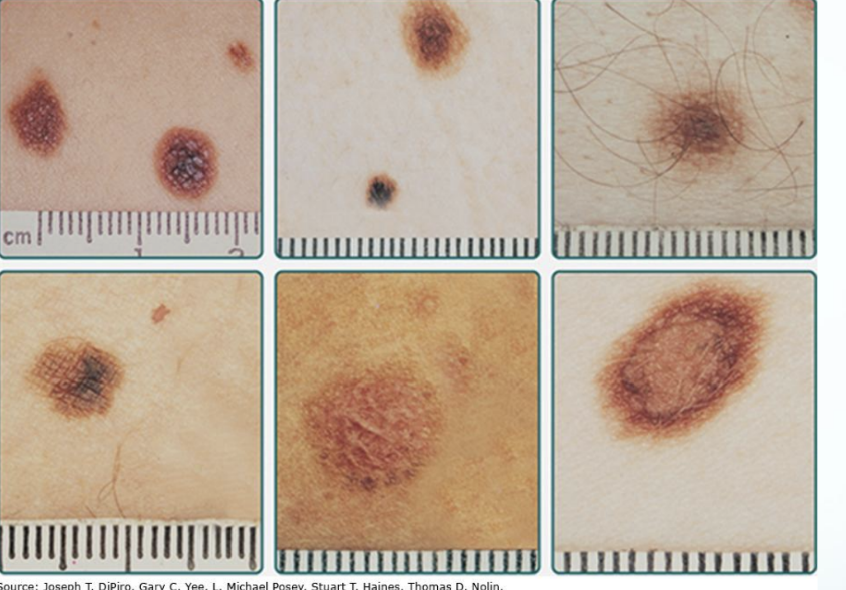
Nevi: black/brown moles or skin growths that appear anywhere on the body
Scale: dry, flaky, patches on skin that can appear white.
caused by ccumulation of dead skin cells on the surface of the skin
Macules

Vesicles & Bullae
 VESICLE & BULLAE
VESICLE & BULLAE
Nodules
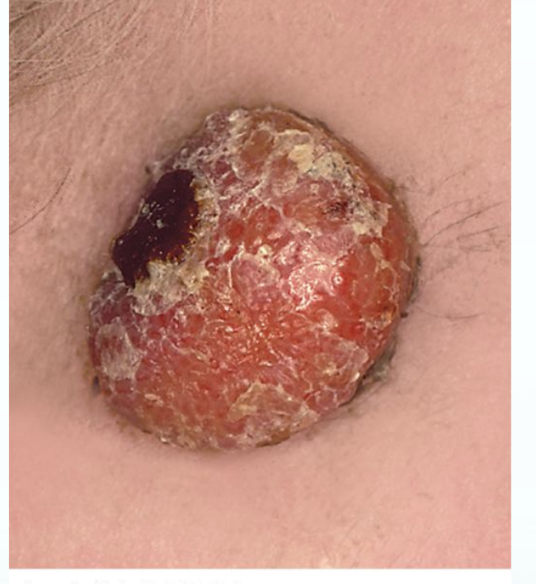
Papules

Psoriasis


Nevi
Xerosis
Dry Skin
Geriatric population
Environmental risk (arid / cold / windy)
Extremely dry skin
Skin cracks / fissures
Pruritus (itching)
Promote MOSITUREZERS*
Fissue

Diaper Rash
Adults with diapers for incontinence
Erythematous, severe rashes w/ vesicles and secondary infections
Candida albicans
Management
Frequent changes, nonsoap cleansers, lukewarm water
Zinc oxide
Can use as prophylaxis
Diaper Dermatitis:
Diaper Rash
Adults w/ diapers for incontinence
TREATMENT: Zinc oxide containing products
Desitin, A&D ointment
IF…Erythematous, severe rashes w/ vesicles and secondary infections then…
Fungus infection caused by Candida albicans
TREATMENT: Antifungal
Nystatin, clotrimazole, miconazole
Non-Pharmacy Management:
Frequent changes, non-soap cleansers, lukewarm water
When to refer
If not better after a few days/week
Ulcerations or any systemic signs: fever, skin lesions elsewhere on body
Sun Damage
Sunburn: 1 blistering sunburn before age 18 doubles your melanoma risk
UV radiation: photoaging and skin cancers
UVA – minimally filtered by ozone layer
UVB – 90% filtered by ozone later
*Promote sun protection & sunscreens
Sunscreens
2 types
Organic (chemical)
Absorb UVA or UVB
Inorganic (mineral)
Broad spectrum - both UVA/UVB
Titanium dioxide or zinc oxide
AVOID sunscreen use for kids under 6 months
FDA regulates sunscreen
Sunscreens that are not broad spectrum or that lack an SPF of at least 15 must carry the warning: "Skin Cancer/Skin Aging Alert: Spending time in the sun increases your risk of skin cancer and early skin aging. This product has been shown only to help prevent sunburn, not skin cancer or early skin aging.”
Non-Pharmacy Sun Protection
Limit time in sun
Protective clothing
Avoid tanning salons & tanning
Seek shade
How To Apply Sunscreen
BEFORE sun exposure
Reapply
Does sunscreen expire?
Yes, sunscreen does expire. Most sunscreens have an expiration date printed on the packaging. It is important to check the expiration date and replace sunscreen that has expired, as the effectiveness of the product may decrease over time.
A word about photosensitizing medications
Some medications lower threshold to develop sunburn
Antibiotics (tetracycline, minocycline, doxycycline)
Sulfa medications (Bactrim, HCTZ)
NSAID (non steroidal anti-inflammatory drugs)
Contact Dermatitis
Definition: inflammation of skin caused by an irritant or allergic sensitizer
5.7 million physician visits annually
Pharmacist consultations
85,000 chemicals considered skin irritant
Irritant Contact Dermatitis (ICD)
*STAYS
Allergic Contact Dermatitis (ACD)
*SPREADS
ICD/ACD Pathophysiology:
ICD: Pathophysiology
External substance that abrades, irritate or damages skin
Clinical result of direct inflammation from pro-inflammatory cytokines released from damaged skin cells
ACD: Pathophysiology
Type IV (delayed hypersensitivity reaction)
2 phases: initial sensitization phase then elicitation phase
Reactions may appear 18-24 hours after exposure
ICD: Poison Ivy
Inflammatory reaction caused by exposure to irritant: oil resin contains Urushiol
Symptoms:
Swelling
Weeping vesicles
Intense Pruritis
50 mcg (size of 1 grain of salt) may cause…
Exclusion to self care * SEND TO DR
Face or genital contact
Rash severity

ICD: Poison Ivy Treatment
WASH the SKIN (and clothes)
The longer on skin the more time for tissue penetration
Reactions typically develop in 12-48 hours and may be transferred to other areas
Zanfel (Lauroyl Sarcosinate)
OTC detergent that binds/lifts urushiol from skin
Fast relief but $
Topical Medications
Hydrocotisone
0.5% and 1% are OTC strengths
Anti-Pruritics
Calamine Lotion, Colloidal Oatmeal
Astringents
Calamine Lotion, Aluminum Acetate
Hydrocortisone
Topical corticosteroid
Non prescription: Lowest potency
Mechanism of Action:“..anti-inflammatory, antipruritic, and vasoconstrictive properties. May depress the formation, release, and activity of endogenous chemical mediators of inflammation (kinins, histamine, liposomal enzymes, prostaglandins) through the induction of phospholipase A2 inhibitory proteins (lipocortins) and sequential inhibition of the release of arachidonic acid. Hydrocortisone has low to intermediate range potency (dosage-form dependent)”
Hydrocortisone Adverse drug reactions:
Acneiform eruption, atrophic striae (stretch marks), burning sensation of skin, folliculitis, hypertrichosis (excess hair growth), hypopigmentation, maceration of the skin, pruritus, secondary skin infection, skin atrophy, skin irritation, xeroderma
Anti-Pruritics (Anti-Itch)
Calamine Lotion
MOA: (?)
converts to zinc oxide, astringent properties
Commonly used to relieve itching and irritation caused by minor skin conditions such as poison ivy, insect bites, and sunburn.
Brands: Caladryl & CVS Calamine Plus.
Colloidal Oatmeal
High concentration in starches & beta-glucan is responsible for the protective & water-holding functions of oat
Different types of phenols confer antioxidant and anti-inflammatory activity
Some oat phenols are strong ultraviolet absorbers
Cleansing activity of oat is mostly dye to Saponins
Avenanthramides inhibit activity of nuclear factor kappaB and release of pro-inflammatory cytokines and histamine
Key mechanisms in pathophysiology of inflammatory dermatoses
Used for: treating various skin conditions such as eczema, dry skin, and itching
Brands: Aveeno
Astringents
MOA: constricts blood vessels, relieves inflammation
“TRING” → “CONSTRICT”
Aluminum acetate (Burow solution)
Produced when aluminum sulfate & calcium acetate are mixed in water
Topical solution acts astringent by constricting blood vessels
Relieves inflammation & itching: cools & dries skin & wet or weeping skin lesions
Brand: Domeboro Soak
Allergic Contact Dermatitis
Difficult to distinguish from ICD
Common reasons for ACD:
Fragrance & Nickels
Testing for allergies
Atopic Dermatitis
Chronic skin disorder involving inflammation and intense pruritis
Itching is responsible for disease burden
Often referred to as eczema
“The itch that rashes”
The Atopic Triad:
Atopic dermatitis
Allergic Rhinitis
Asthma
AD: Epidemiology
Most cases manifest before age of 1 year
85%-95% of patients develop symptoms before 5 years of age
10%-30% will continue with symptoms through adulthood
Periods of exacerbations (flare ups) and remission
Prevalence: 15-30% of children; 2-10% of adults
$5 billion dollar health care burden
AD: Etiology
Clinical diagnosis
No biomarker / no lab test
Genetic predisposition
T-helper predominance (Th2)
Mutation in Filaggrin (FLG) gene (key structural protein in epidermal differentiation)
AD = epidermal barrier dysfunction / enhanced allergen absorption through the skin
AD: Pathophysiology
Unknown MOA, trigger inflammatory changes in the skin
Predisposing factors: climate, infection, genetics diet, family history
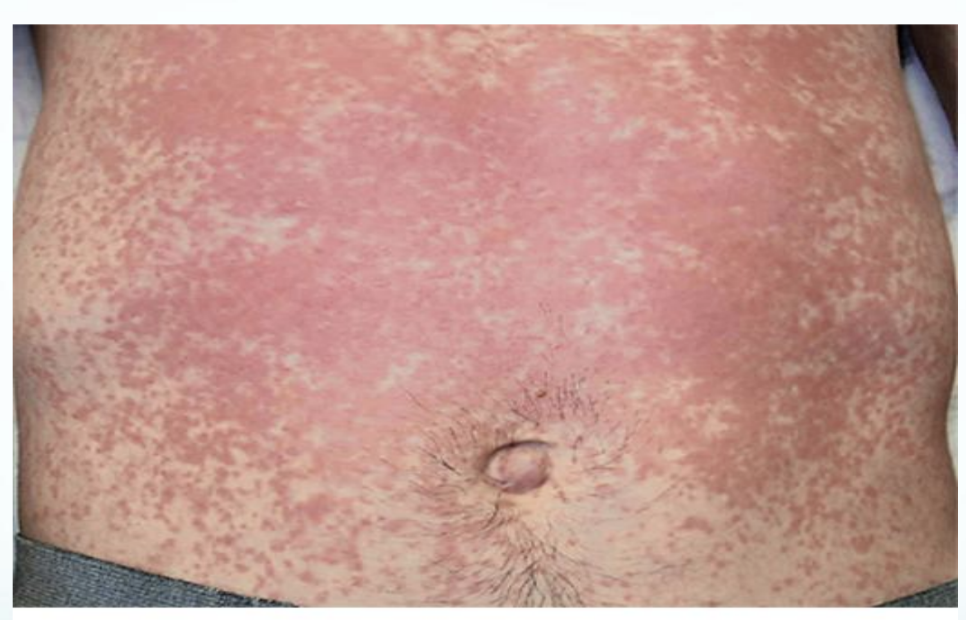
AD: Clinical Presentation
Infancy: Erythematous papular skin eruption on cheeks/chin, patchy facial areas
Lesions on flexor surfaces (Antecubital & Popliteal fossa)
Dry, flaky, rough, cracked skin
Lichenification: occurs from repeated rubbing of the skin
Prone to skin infections: Staphylococci aureus
Impetigo
Non-Rx Therapy
Apply Moisturizer
Standard of care
May reduce disease severity and need for RX
Improves AD associated xerosis
May be steroid sparing
Lukewarm bath with application of moisturizer after bathing once or twice daily
Keep humidity at home at or above 50%, cool room temps
Nonsoap cleansers like Cetaphil
Stress relief
Cotton sheets
Wear loose fitting clothing
Aviod high heat
Moisturizers
Occlusives: form a film to reduce the loss of water from the skin
Petrolatum, mineral oil
Humectants: attract and bind water from surroundings
Urea, alpha hydroxy acid
Emolients: lubricate the skin
Lanolin, glyceryl stearate, soy sterols
Moisturizers Formulation Characteristics
Cream: less greasy than ointment, preferred for AD
Lotion: less greasy than cream, quicker to be absorbed
Ointment: best for thick/extremely dry areas (lichenified)
Gel: quick drying
Solutions: quick drying
Foams: use for scalp
Hydrocortisone
Topical corticosteroid
Non prescription: Lowest potency
Mechanism of Action:
Anti-inflammatory, antipruritic, and vasoconstrictive properties
May depress the formation, release, and activity of endogenous chemical mediators of inflammation
Hydrocortisone has low to intermediate range potency
Hydrocortisone Adverse drug reactions:
Acneiform eruption, atrophic striae, burning sensation of skin, folliculitis, hypertrichosis, hypopigmentation, maceration of the skin, pruritus, secondary skin infection, skin atrophy, skin irritation, xeroderma
At increased risk of adrenal suppression with higher potency
Administration
Fingertip rule
Only thin layer necessary
Squeeze a ribbon of medication onto index finger
Amount should cover both palms of hand
Length of treatment
Use for short duration: AD
What goes first?
general guideline is to apply products from thinnest to thickest consistency.
foam, solution, gel, lotion, cream, & ointment
Topical Corticosteroids
Class 1: Superpotent
Betamethasone dipropionate 0.05% ointment (Diprolene and Diprosone ointment)
Clobetasol propionate 0.05% lotion/spray/shampoo/foam (Clobex lotion/spray/shampoo, OLUX-E foam)
Clobetasol propionate 0.05% cream and ointment (Cormax, Temovate, Dermovate)
Desoximetasone 0.25% spray (Topicort)
Fluocinonide 0.1% cream (Vanos)
Halobetasol propionate 0.05% cream, lotion, and ointment (Ultravate)
Flurandrenolide tape 4 mcg/cm2 (Cordran)
Class 2: Potent
Amcinonide 0.1% ointment (Cyclocort ointment)
Betamethasone dipropionate 0.05% cream/gel (Diprolene cream, gel, and Diprosone cream)
Desoximetasone 0.25% cream, ointment (Topicort)
Diflorasone diacetate 0.05% ointment (Florone, Psorcon)
Fluocinonide 0.05% cream, gel, ointment (Lidex)
Halcinonide 0.1% cream (Halog)
Class 3: Upper mid-strength
Amcinonide 0.1% cream (Cyclocort cream)
Betamethasone valerate 0.1% ointment (Betnovate/Valisone ointment)
Diflorasone diacetate 0.05% cream (Psorcon cream)
Fluticasone propionate 0.005% ointment (Cutivate ointment)
Mometasone furoate 0.1% ointment (Elocon ointment)
Triamcinolone acetonide 0.5% cream and ointment (Aristocort)
Class 4: Mid-strength
Betamethasone valerate 0.12% foam (Luxiq)
Clocortolone pivalate 0.1% cream (Cloderm)
Desoximetasone 0.05% cream, ointment, and gel (Topicort LP)
Fluocinolone acetonide 0.025% ointment (Synalar ointment)
Fluocinolone acetonide 0.2% cream (Synalar-HP)
Flurandrenolide 0.05% ointment (Cordran)
Hydrocortisone valerate 0.2% ointment (Westcort ointment)
Mometasone furoate 0.1% cream (Elocon cream)
Triamcinolone acetonide 0.1% ointment (Kenalog)
Class 5: Lower mid-strength
Betamethasone dipropionate 0.05% lotion (Diprosone lotion)
Betamethasone valerate 0.1% cream and lotion (Betnovate/Valisone cream & lotion)
Desonide 0.05% lotion (DesOwen)
Fluocinolone acetonide 0.01% shampoo (Capex shampoo)
Fluocinolone acetonide 0.025%, 0.03% cream (Synalar cream)
Flurandrenolide 0.05% cream and lotion (Cordran)
Fluticasone propionate 0.05% cream and lotion (Cutivate cream and lotion)
Hydrocortisone butyrate 0.1% cream (Locoid)
Hydrocortisone valerate 0.2% cream (Westcort cream)
Prednicarbate 0.1% cream (Dermatop)
Triamcinolone acetonide 0.1% cream and lotion (Ke
Class 6: Mild
Alclometasone dipropionate 0.05% cream and ointment (Aclovate)
Betamethasone valerate 0.05% cream and ointment
Desonide 0.05% cream, ointment, gel (DesOwen, Desonate, Tridesilon)
Desonide 0.05% foam (Verdeso)
Fluocinolone acetonide 0.01% cream and solution (Synalar)
Fluocinolone acetonide 0.01% FS oil (Derma-Smoothe)
Antipruritics
Calamine lotion
MOA: (?), converts to zinc oxide, astringent properties
Colloidal oatmeal
High concentration in starches and beta-glucan is responsible for the protective and water-holding functions of oat
Different types of phenols confers antioxidant and anti-inflammatory activity
Some of the oat phenols are also strong ultraviolet absorbers
The cleansing activity of oat is mostly due to saponins
“Avenanthramides” inhibit activity of nuclear factor kappaB and release of proinflammatory cytokines and histamine
well known key mechanisms in the pathophysiology of inflammatory dermatoses
Antihistamines
MOA: block histamine (H1)
Oral formulations
Diphenhydramine
Loratadine
Cetirizine
Topical antihistamines should be avoided
Yes, an antihistamine can have antipruritic properties. Antihistamines work by blocking the effects of histamine, a chemical released during an allergic reaction that can cause itching (pruritus) and other symptoms. By reducing histamine activity, antihistamines can help relieve itching and provide antipruritic effects.
Atopic Dermatitis: Exclusions to Self Care:
Infants less than 1 year old
Signs of active infection
Large body surface area involvement
Face
Atopic Dermatitis Case
A parent comes to your community pharmacy complaining “My child constantly wants to scratch her skin, and she can’t sleep well during the night.” What information would you collect from the parent?
To properly assess the situation, you would collect the following information from the parent:
Age of the child: This helps determine if the symptoms are age-related or if they could be due to a specific condition.
Duration of symptoms: Knowing how long the child has been experiencing these symptoms can provide insights into the possible causes.
Any known allergies: Allergies can often cause skin itching and disrupt sleep, so it's important to inquire about any known allergies.
Recent changes in environment or routine: Changes in detergents, soaps, or other environmental factors can trigger skin irritation.
Other accompanying symptoms: Inquire about any other symptoms the child may be experiencing, such as redness, rash, or fever.
Family history: Ask if there is a history of skin conditions or allergies in the family, as these can be hereditary.
Atopic Dermatitis Case
What are the clinical signs and symptoms of AD
Clinical signs and symptoms of Atopic Dermatitis (AD):
Itchy skin: Intense itching is a hallmark symptom of atopic dermatitis.
Dry skin: Skin may appear dry, rough, and scaly.
Redness and inflammation: Affected areas of the skin may be red, swollen, and inflamed.
Rash: A rash may develop, typically in the folds of the skin, such as behind the knees or in the crook of the elbows.
Cracked and thickened skin: Over time, the skin may become thickened, cracked, and leathery.
Blisters or oozing: In severe cases, blisters or oozing may occur, leading to crusting and weeping of the skin.
Skin discoloration: The affected skin may become lighter or darker in color.
Sleep disturbances: Itching can disrupt sleep, leading to fatigue and irritability.
Emotional distress: The chronic nature of atopic dermatitis can cause emotional distress, including anxiety and depression.
Secondary infections: Scratching can lead to open sores, increasing the risk of bacterial or viral infections.
AD: Case
What non-pharmacologic therapy would you recommend?What moisturizer would you recommend? How often to apply? What is best time to apply?
Non-pharmacologic therapy for atopic dermatitis includes:
Moisturizing regularly: Use a fragrance-free moisturizer to hydrate the skin and prevent dryness.
Avoiding triggers: Identify and avoid irritants or allergens that can worsen symptoms.
Gentle skincare routine: Use mild, non-irritating cleansers and avoid excessive scrubbing or hot water.
Moisturizer recommendation: A thick, emollient moisturizer with ingredients like ceramides or petrolatum is often recommended.
Frequency of application: Apply moisturizer at least twice daily, or as directed by a healthcare professional.
Best time to apply: Apply moisturizer immediately after bathing or showering to lock in moisture.