Chapter 6: Demand for Health and Medical Care
Production of Health
Health Production Function
Health production is a derived demand for medical care (Grossman, 1972).
Net investment in health of individual j:

where = Level of health
= Investment in health,
= Rate of Depreciation.
Medical care and other inputs contribute to good health.
Gross investment in health during period t:

I = Investment in health
= Medical care services,
= Time spent improving health,
= Human capital stock,
= Age,
= Behavior (lifestyle).
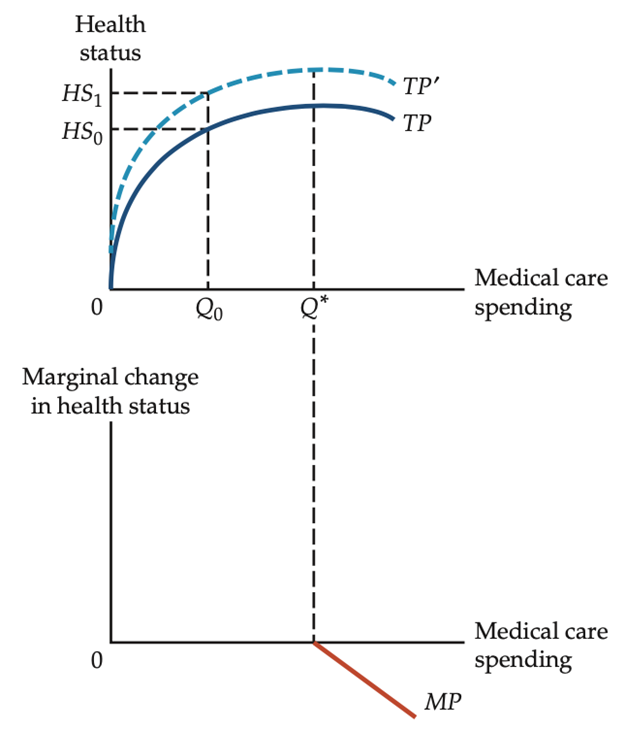
Health-Status and Medical Care Spending
Hypothesized relationship yields a positively sloping function.
Health status increases with medical care spending
However, the function displays diminishing returns.
Increasing medical care spending moves along function.
Change in other inputs causes the total product curve to shift.
After level Q* of spending, the production function has a negative slope.
Medical care spending beyond this point yields net harm to patient.
Determinants of Health (Overview)
Deteminants of Health (1 of 5) – Factors Other Than Medical Care
1. Income and Education:
Higher socioeconomic status often indicates better access to medical care and better health outcomes.
Low socioeconomic status does not automatically imply poor health.
Nutrition, housing, environment, and other factors play direct roles.
Empirically:
Low-income Americans experience higher mortality (Pappas et al., 1993).
Education is associated with better longevity and life expectancy (Guralnik et al., 1993).
Higher education increases production efficiency of health (Grossman, 1972).
Determinants of Health (2 of 5)
2. Environment and Lifestyle:
Environmental pollution has a strong negative effect on human life and the quality of life.
Estimated 65 percent of all cancer in the United States associated with lifestyle and environmental factors (American Cancer Society).
Correlation exists between exposure to environmental toxins and illness in children (Note: correlation does not imply causation).
Personal behavior also strongly affects health, including:
Diet, exercise, sexual behavior, smoking, substance abuse, violence.
Determinants of Health (3 of 5)
3. Genetics
There is a risk of exposure to a disease (public health) as well as the ability to resist and recover from the disease (genetics)
Hereditary factor in predisposition to certain diseases
e.g., women with family history of ovarian cancer places them at a 40 percent risk of developing the disease, whereas the general population faces a risk of only 7 percent.
Strong family predisposition a significant factor in allergies, hypertension, obesity, cystic fibrosis, sickle cell anemia, and snoring.
Determinants of Health (4 of 5)
Public Health
The state provides services important to health, such as:
Water purification, sewage treatment, immunization programs, quarantines, clean air standards, food safety.
McKeown (1976) attributed historical decline of mortality in North America and Europe to four major sources in order of significance:
Living standards, public health intervention, disease decline, and advancements in medical science.
Deteminants of Health (5 of 5)
Beginnings of Public Health
London cholera pandemic (1846–1860):
Two outbreaks, ~250,000 cases and ~75,000 deaths.
John Snow (obstetrician) identified water as the source:
Waterborne disease, not airborne .
Used mapping to determine the exact location of the water source:
Measures of Health (1 of 3)
Quantifiable measures of health are important, but those existing are limited
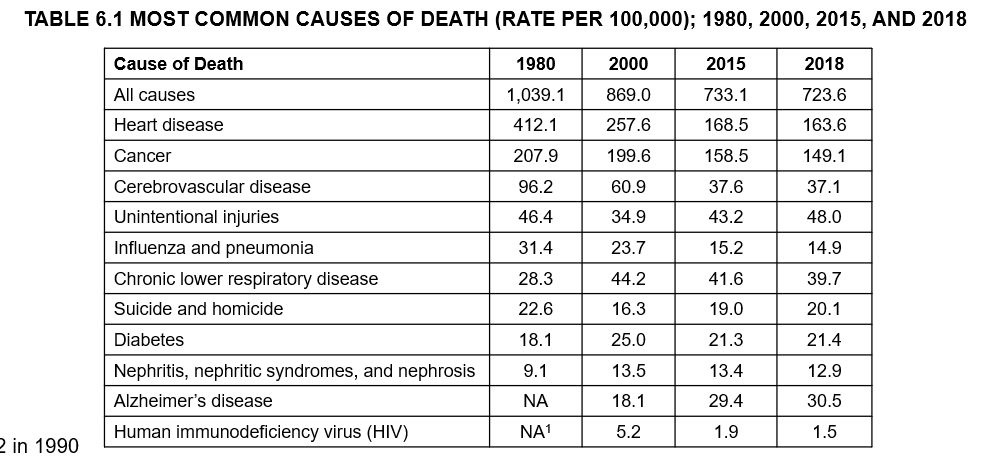
Mortality Rates
Defined as number of deaths per 100,000.
Often reduced to subgroups of age, sex, and race for comparison.
Male and female life expectancies at birth and infant mortality other common indicators.
Overall poor indicator of quality of life.
Low crude mortality rate does not always reflect a healthy population.
Measures of Health (2 of 5) – Table: Common Causes of Death (Rate per 100,000)
Measures of Health (3 of 5)
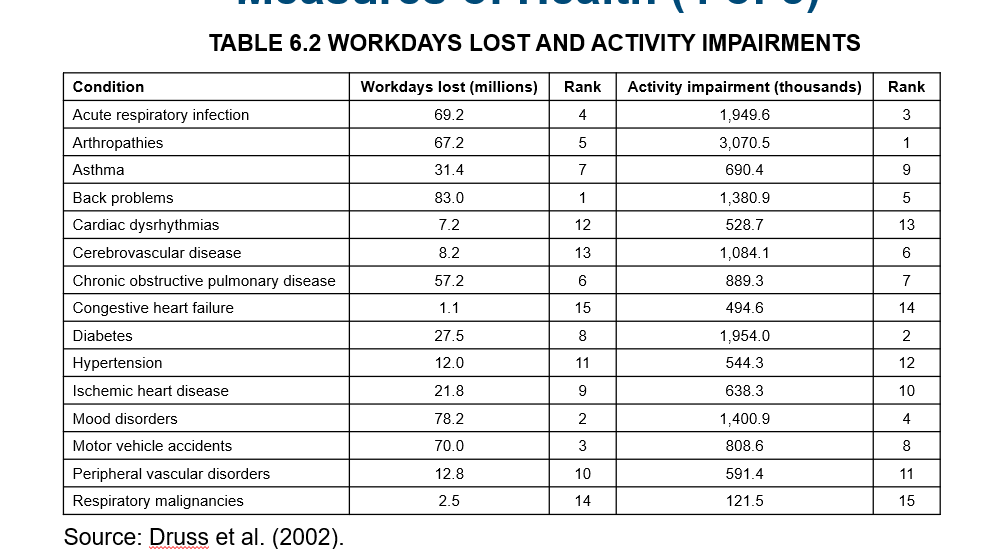
Morbidity Rates
Prevalence of certain diseases or medical conditions
Common measures include restricted activity days due to illness, the incidence rate of certain chronic conditions, and a self-assessment of health status.
Newhouse and Friedlander (1980) used six measures to analyze the health status of a region in relation to the medical services available:
Diastolic blood pressure, serum cholesterol concentration, and electrocardiogram abnormalities (reflect cardiovascular disease).
Abnormal chest X-rays (cancer), varicose veins (condition of connective tissue), and periodontal index (preventive-care practices)
Measures of Health (4 of 5) – Workdays Lost and Activity Impairments
Measures of Health (5 of 5)
3. Quality of Life Metrics
Quality-adjusted life years (QALY):
Index combining quality of life and survival duration
Can be used to set allocation priorities within a program (e.g., waitlist for a kidney).
Disability-adjusted life expectancy (DALE):
Measures time spent living with a health condition considered less than optimal, plus time lost due to premature death.
More simply, the number of years living in poor health or lost to illness or injury.
Commonly used in cross-country comparisons.
Demand Factors (1 of 5) – Demand for Medical Care as Investment
Medical care is an investment in human capital.
Function for medical care demand:

= health stock,
= demographic characteristics,
= socioeconomic standing,
= physician factors.
Demand for medical care is derived from the demand for health.
Affected by factors related to both patients and physicians.
Demand Factors (2 of 5) – Patient Factors
Health stock
Seek medical care to prevent disease or in response to an illness or injury.
Demographic characteristics
Demand varies according to population growth and age, between sexes.
Economic standing
Better access, better consumers, insurance coverage
Demand Factors (3 of 5) – Effect of Insurance on Demand
Insurance changes patient price exposure and can increase demand due to lower out-of-pocket costs; creates moral hazard.
Insurance design (deductibles, copayments) and coverage levels influence the quantity and type of care sought.
Demand Factors (4 of 5) – Provider-Induced Demand
Physician as agent: physicians largely determine medical spending.
Demand creation concept: Roemer’s Law – a built bed is a filled bed.
Third-party insurance introduces moral hazard affecting both patients and providers.
Myth: Increasing capacity automatically expands sales without bound; reality: evidence shows hospital capacity is often underutilized, limiting unconditional capacity-driven demand.
Demand Factors (5 of 5) – Demand Inducement Related to Increased Supply
Increases in supply can induce higher demand, through mechanisms such as advertising, technology diffusion, and physician practice patterns.
Measuring Demand (1 of 4) – Basic Relationships and Elasticities
Relationship between demand for medical care and out-of-pocket payments varies by:
Insurance status (insured vs uninsured),
Deductibles and copayments among insured individuals.
Key determinants of demand include:
Price, income, insurance coverage, time cost.
Demand is typically estimated via regression analysis.
Elasticities studied:
Price elasticity, income elasticity, insurance elasticity, time-cost elasticity, cross-price elasticity.
General finding: demand for medical care is relatively inelastic with respect to price.
Measuring Demand (2 of 4) – Elasticities (Selected Studies)
Table: Price and Income Elasticities (selected studies)
Davis and Russell (1972):
Dependent variable: Outpatient visits; Elasticity: price ≈ −1.00
Hospital admissions: price ≈ −0.32 to −0.46
Rosett and Huang (1973):
Hospital and physician spending: price ≈ −0.35 to −1.50
Newhouse and Phelps (1976):
Hospital length of stay: price ≈ −0.06 to −0.29
Physicians’ office visits: price ≈ −0.08 to −0.10
Manning et al. (1987):
Overall spending: price ≈ −0.22
Hospital care: −0.14
Preventive care: −0.43
Wedig (1988):
Level of care: price ≈ −0.16 to −0.23
Eichner (1998):
Medical care: price ≈ −0.62 to −0.75
Contoyannis et al. (2005):
Pharmaceuticals: price ≈ −0.12 to −0.165
Income elasticities (selected studies):
Newhouse (1977): Per capita medical spending: 1.15 to 1.31
Parkin, McGuire, and Yule (1987): Per capita medical spending: 0.80 to 1.57
Gerdtham and Jönsson (1991): Per capita medical spending: 1.24 to 1.43
Moore, Newman, and Fheili (1992): Short-run per capita spending: 0.31 to 0.86; Long-run per capita spending: 1.12 to 3.22
Murray, Govindaraj, and Musgrove (1994): Total health expenditures: 1.43
Manning and Marquis (1996): Medical expenditures: 0.22
Fogel (1999): Health care expenditures: 1.60
Okunade and Murthy (2002): Per capita real health care spending: 1.29 to 1.64
Herwartz and Theilen (2003): Growth rate per capita health spending: 0.74
Dormont et al. (2010): Per capita health spending: 0.75 to 1.59
Acemoglu et al. (2013): Per capita health spending: 0.72 to 1.13
Measuring Demand (3 of 4) – RAND Experiment (1971–1982)
Design:
Randomly assigned ~2,000 non-elderly families to insurance plans with two characteristics:
Coinsurance rate: 0–95%
Deductible: 5, 10, or 15% of annual income
Annual spending cap: $1,000
Measured outcomes:
Health spending and health outcomes.
Measuring Demand (4 of 4) – RAND Conclusions
Demand for medical care appears relatively price-inelastic:
Overall price elasticity ≈ −0.2
Hospital care elasticity ≈ −0.15
Preventive care elasticity ≈ −0.4
Income elasticities (individual): approximately +0.22, suggesting medical care is a normal good and may be a necessity.
Aggregate income elasticities tend to be higher, indicating medical care may be a superior good (some would call it a luxury) at the population level.
Additional Notes: Practical and Ethical Implications
Moral hazard in insurance: insurance coverage can increase utilization beyond the amount chosen by patients, creating cost pressures on payers and potential overuse concerns.
Provider-induced demand: physicians’ practice patterns and incentives can drive utilization; policy implications include capacity management and payment reform to align incentives.
Public health investments: historical evidence emphasizes living standards and public health interventions as major contributors to mortality declines, sometimes more than medical care innovations alone.
Measurement limitations: many health outcomes (quality of life, DALE, QALY) require careful interpretation, cross-country comparability, and may reflect value judgments about quality and duration of life.
Ethical considerations in allocation: QALYs and DALEs influence resource allocation decisions; trade-offs between extending life, preserving quality of life, and equity across populations must be considered.