HTN Vasc Problems Student Outline1 (1)
Care of Patients with Vascular Problems
Presented by: Shannon Daly, DNP, MSN-Ed., RN
IGGY Chapter 33, ATI Chapter 35, 36, 38
Common Vascular Problems
Part 1: Hypertension (HTN)
Essential HTN: This is primary hypertension with no identifiable cause, which is most common in adults and often linked to lifestyle factors.
Secondary HTN: This occurs due to an underlying condition such as kidney disease or hormonal disorders.
Malignant HTN: A severe and rapid form of hypertension that can result in acute organ damage.
Part 2: Arteriosclerosis & Atherosclerosis
Arteriosclerosis: A general term for thickening and hardening of arterial walls.
Atherosclerosis: A specific type of arteriosclerosis characterized by the buildup of plaques composed of fat, cholesterol, and other substances.
Part 3: Peripheral Arterial Disease (PAD)
This can lead to decreased blood flow to the extremities, causing pain during activity (claudication) and risk of ischemia.
Acute Peripheral Arterial Occlusion: A sudden arterial blockage that can result in severe consequences like limb loss if not treated promptly.
Aneurysms: Bulging of the arterial wall which can rupture, leading to life-threatening bleeding.
Central Arteries: Aneurysms in major arteries (e.g., aorta).
Peripheral Arteries: Aneurysms in peripheral vessels that may require monitoring or surgical intervention.
Aortic Dissection: A serious condition in which the inner layer of the aorta tears, causing severe pain and potentially life-threatening complications.
Part 4: Venous Thromboembolism (VTE)
Venous Insufficiency: A condition where veins cannot pump enough blood back to the heart, leading to swelling and discomfort.
Hypertension (HTN)
Most Common Health Problem in Primary Care
Estimated 87.5 million adults <20 have high blood pressure (HBP).
Long-term effects can include:
Stroke: Increased risk of cerebrovascular accidents due to damage to blood vessels.
Myocardial Infarction (MI): Higher risk due to increased workload on the heart muscle, leading to ischemia.
Kidney Failure: Damage to blood vessels in the kidneys, affecting filtration.
Premature Death: Related to complications from unmanaged hypertension.
Categories of BP in Adults (per ATI):
Normal: <120/<80
Prehypertension: 120-139/80-89
Stage 1: 140-159/90-99
Stage 2: >160/100
Etiology of HTN
Essential HTN Risk Factors:
Family history of hypertension, particularly in close relatives.
Ethnic Factors: Higher prevalence in African-Americans due to genetic and environmental influences.
Lifestyle Factors: Hyperlipidemia, smoking, age (especially in individuals <60 or post-menopausal), excessive sodium and caffeine intake, obesity, physical inactivity, excessive alcohol intake, low dietary intake of potassium, calcium, or magnesium, and continuous stress.
Secondary HTN Causes:
Kidney conditions like chronic kidney disease that affect blood pressure regulation.
Hormonal disorders like primary aldosteronism or Cushing's disease.
Structural abnormalities including coarctation of the aorta.
Neurological issues such as brain tumors or encephalitis and complications during pregnancy.
Certain medications including hormonal contraceptives and glucocorticoids that impact blood pressure.
Pathophysiology of HTN
Hypertension results from conditions that increase Heart Rate (HR), Stroke Volume (SV), or Total Peripheral Resistance (PVR).
Key Physiological Equation:
Increased HR, SV, or PVR leads to Increased BP.
Decreased HR, SV, or PVR results in Decreased BP.
Control Systems: Include the Arterial Baroreceptor System, Regulation of Body Fluid Volume, Renin-Angiotensin-Aldosterone System, and Vascular Autoregulation to maintain hemodynamic stability.
Assessment of HTN
Patient History & Physical Assessment: Collect comprehensive health information and conduct a thorough physical examination.
Accurate BP Reading: Ensure proper technique and conditions for measuring blood pressure.
Check for Orthostatic Hypotension: Assess BP changes with position changes to evaluate autonomic function.
Evaluate factors affecting adherence to treatment plans, including psychological stressors.
Diagnostic Assessments: May include blood tests and imaging studies to rule out secondary causes.
Lifestyle Modifications to Improve BP
Weight Reduction: Aim for a BMI of 18.5-24.9 kg/m2 which may provide an average reduction of approximately 5 mm Hg.
DASH Eating Plan: A diet rich in fruits, vegetables, low-fat dairy with a potential reduction of 11 mm Hg.
Sodium Intake: Limit to <1500 mg/day possibly reducing BP by 5-6 mm Hg.
Physical Activity: Engage in moderate-intensity exercise 90-150 minutes/week, with a resultant decrease of 5-8 mm Hg.
Alcohol Consumption: Limit intake to a maximum of 2 drinks/day for men, 1 for women, as this may lower BP by approximately 4 mm Hg.
Common HTN Drug Therapy
Diuretics: First-line agents; help to reduce fluid volume in the body.
spironolactone (potassium-sparing) watch for hyperkalemia
furosemide, bumetanide (loop), watch for hypokalemia
hydrochlorothiazide, chlorothiazide ( thiazide) watch for hypokalemia
Beta-Adrenergic Blockers: Decrease heart rate and force of contraction.
Atenolol
metoprolol
ACE Inhibitors: Inhibit angiotensin II production leading to vasodilation.
lisinopril
enalapril
captopril
Calcium Channel Blockers: Relieve coronary artery spasms.
verapamil
amlodipine
diltiazem
Angiotensin II Receptor Blockers (ARBs): Similar effects as ACE inhibitors but may cause fewer side effects.
valsartan
losartan
Renin Inhibitors: Directly inhibit renin activity for a BP-lowering effect.
Alpha-Adrenergic Agonists: Decrease sympathetic outflow to the heart.
Aldosterone Receptor Antagonists: Important for patients with heart failure and hypertension.
Drug Classes for Managing HTN
Diuretics
first type of drug for managing hypertension
used to decrease blood volume (pre-load) such as treat HF by removing excessive extracellular fluid and lower BP.
Types:
Potassium-Sparing Diuretics: Relax blood vessels and conserve potassium.
teach pt to decrease intake of food high in potassium and get lab test for electrolyte levels
teach pt report weakness and irregular pulse to the provider because these symptoms may indicate hyperkalemia
Loop Diuretics: rapidly reduce fluid overload.
teach pt to eat food high in potassium and have a follow-up lab test to monitor electrolyte levels ( k and Mg)
use cautiously in pt with diabetes because glucose control can be affected.
use cautiously in pt with gout because uric acid retention can occur.
Thiazide Diuretics: Effective for long-term use in managing hypertension.
ACE Inhibitors (-pril)
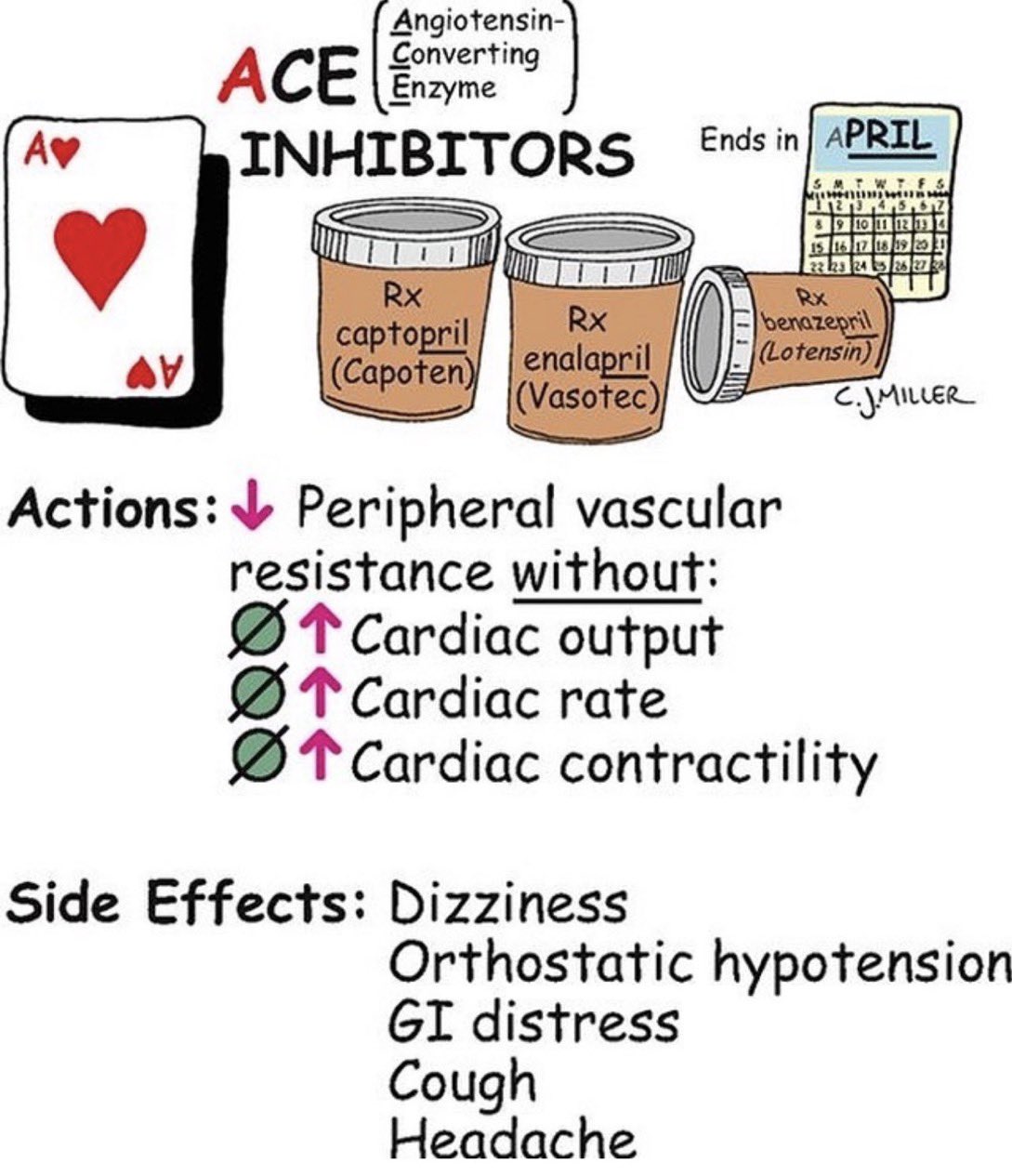
Help to decrease afterload and increase vasodilation, leading to lower BP.
report persistent, dry cough because this is a common side effect
monitor BP carefully, especially orthostatic pressure because these agents result in vasodilation and decreased BP
don’t give without checking systolic BP is below 100
assess for hyperkalemia.
Beta Blockers (-olol)
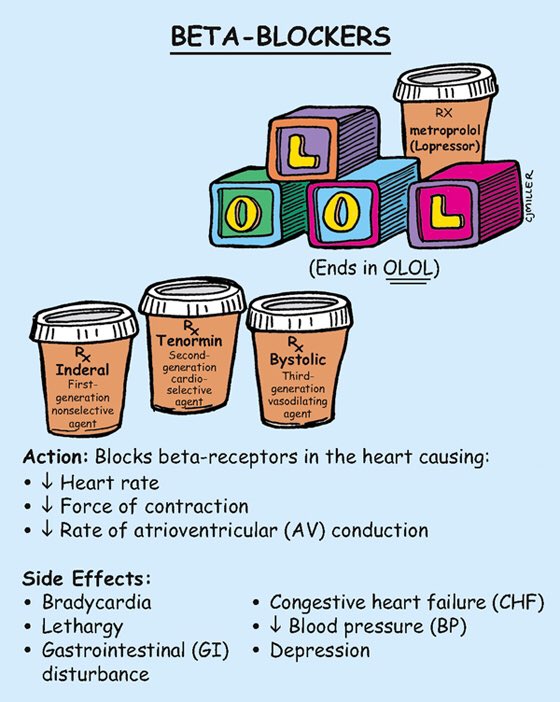
Monitor for potential side effects including hypoglycemia, particularly in diabetic patients. They are contraindicated in asthma patients due to bronchoconstriction effects.
don’t give if HR is below 50-60 bpm
hold if systolic is below 90-100 mmHg
monitor orthostatic hypotension
Atherosclerosis & Arteriosclerosis
Definitions
Arteriosclerosis: Thickening and stiffening of arterial walls, often associated with aging and contributing to cardiovascular disease.
Atherosclerosis: Characterized by plaque buildup in arteries, leading to narrowing and potential blockages that can result in ischemia.
genetic predisposition
diabetes
Risk Factors for Atherosclerosis
Items such as low HDL-C, high LDL-C, and high triglycerides contribute to increasing cardiovascular risk.
Additionally, genetic factors, sedentary lifestyle, smoking, chronic stress, and demographic factors (higher risk in African-American and Hispanic populations) increase susceptibility.
Physical Assessment
Monitor vital signs; assess BP in both arms
Palpate major body-site pulses; palpate each carotid artery separately.
assess lower extremities for temperature differences
prolonged capillary refill
bruits: indicative of turbulent blood flow.
Cholesterol Levels: Regularly gauge HDL versus LDL levels through laboratory assessments; aim for high HDL and low LDL to mitigate risks.
Interventions for Atherosclerosis
Nutritional and Lifestyle Changes: Engage patients in low-cholesterol diets, weight management, and smoking cessation.
Regular Exercise: Encouraged as part of overall cardiovascular health strategies.
Drug Therapy: Consider statins for patients unable to achieve targets through lifestyle changes alone.
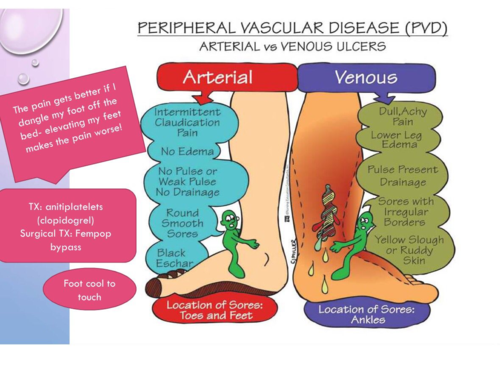
Peripheral Arterial Disease (PAD)
Leads to decreased blood flow through peripheral arteries, causing a spectrum of symptoms, including pain and cramps in the legs during exercise.
alters the natural flow of blood through arteries and veins of peripheral circulation
resulting of systemic atherosclerosis
inflow diseases: discomfort in the lower back, buttocks, and thighs
Outflow disease: burning or cramping in calves, ankles, feet, and toes.
Physical Assessment Stages
Stage I: Asymptomatic phase
no claudication
pedal pulses are decreased or absent
bruits or aneurysms may be present
Stage II: Claudication
muscle pain, cramping, or burning occurs with exercise and is relieved with rest
symptoms are reproducible with exercise
Stage III: Rest Pain
pain while resting commonly awakens the patient at night
pain is described as numbness, burning, toothache-type pain
pain usually occurs in the distal part of the extremity (toes, arch, forefoot, or heel) rarely in the calf or the ankle
pain is relieved by placing the extremity in a dependent position
Stage IV: Necrosis/Gangrene
ulcers and blackened tissue occur on the toes, forefoot, and heel
distinctive gangrenous odor is present
Physical assessment
hair loss and dry, scaly, pale, or mottled skin
thickened toenails
severe- cold extremity, gray-blue (cyanotic) or darkened
Pallor may occur when the extremity is elevated
dependent Rubor (redness) may occur when the extremity is lowered
palpate posterior tibial pulse- the most sensitive and specific indicator of the pad is the quality of this pulse; compare bilaterally.
Diagnostic Assessments for PAD
Magnetic Resonance Angiography (MRA) to visualize blood flow in peripheral arteries
Ankle-Brachial Index (ABI): A measurement of leg blood flow where <0.90 is diagnostic of PAD.
Exercise Tolerance Test: Used to evaluate claudication severity.
Non-surgical Management of PAD
Implement structured exercise programs and positioning strategies to promote vascular health are used to improve arterial blood flow through collateral circulation.
provide warmth and avoid long exposure to the cold
emotional stress, caffeine, nicotine cause vasoconstriction
aspirin or clopidogrel (anti-platelet agents)
Surgical Management
Consider arterial revascularization for critical conditions.
preoperative
document vital signs and peripheral pulses provide baseline
pt may have 1 or more IV lines, urinary catheters, central venous catheters, and/ or arterial line
antibiotic therapy is given to prevent post-op infection
intraoperative
anesthesia
postoperative
deep breathing every 1 to 2 hrs and using incentive spirometer
monitor for graft occlusion (emergency)
treatment for graft occlusion
monitor for compartment syndrome
assess for infection
mark the pulse
Acute peripheral arterial occlusion
embolus- pieace of a clot that travels and lodges in a new area. is the most commom cause of peripheral occlusions, although a local thrombus may be the cause.
emboli originating from the heart are the most common cause of acute arterial occlusions. most pt with an embolic pcclusion have had an acute MI or atrial fibrillation within the previous week.
drug therapy
UNFRACTIONATED HEPARIN- USUALLY FIRST INTERVENTION. to prevent further clot formation.
T-PA
surgical therapy
thrombectomy or embolectomy- small incision which is followed by an arteriotomy a surgical opening into thean artery
Nursing Care ( after an arterila thrombectomy)
Observe extremity for improvent in color, temp, pulse every hour for the first 24 hrs
monitor for evidence of new thrombi or emboli
CP, dyspnea, acute confusion ( older adults)
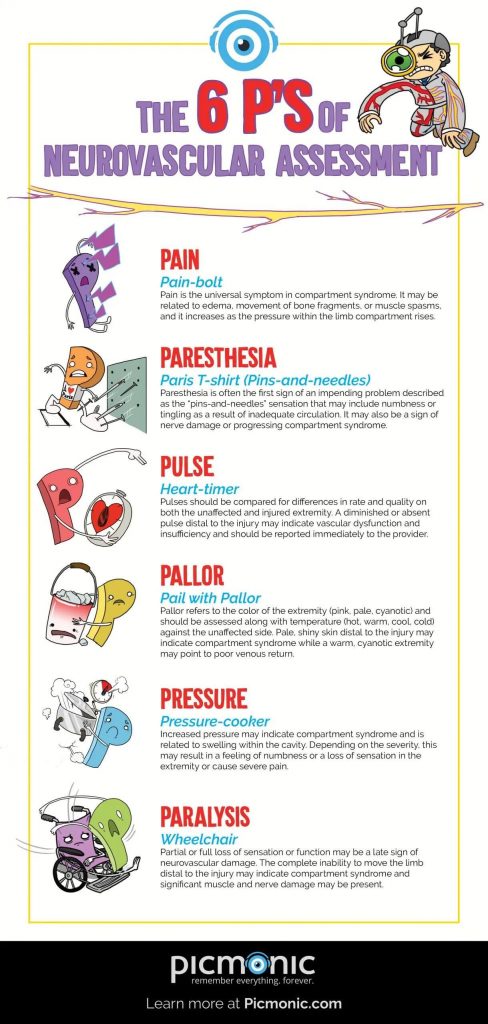
the 6’s ps of ischemia.
the effected extremity is cool or cold, pulseless, and mottled. small areas on the toes may be blackened or gangrenous due to lack of perfusion.
Peripheral Venous Disease (PVD)
Venous Thromboembolism (VTE)
Thrombus: A blood clot formed from elements like platelets and fibrin.
Virchow's Triad: Identifies three main risk factors leading to clot formation: stasis, injury to the vessel wall, and hypercoagulability.
Deep Vein Thrombosis (DVT): Common occurrence that poses a risk for pulmonary embolism (PE).
mostly in lower legs but can develop in uppeer arms
phlebitis- vein inflammation
thrombophlebitis- thrombus associated with inflammation
mostly occurs in deep veins of lower extremities
Pulmonary embolism- a dislodged blood clots travels to pulmonary artery. MEDICAL EMERGENCY
Assessment of VTE
Complete assessment of symptoms: Includes swelling, tenderness, and potential limb discoloration.
Diagnostic Tests: Utilize non-invasive imaging methods like venous duplex ultrasonography, alongside laboratory markers such as D-dimer.
localized edema
MRI noninvasive proximal deep veins
Nonsurgical Management of VTE
Encourage active leg movements, promote early ambulation, and ensure adequate hydration to prevent clot formation.
Implement compression devices and prescribe anticoagulation therapies as needed.
Surgical Management of VTE
Surgical options like thrombectomy- surgical procedure fro clot removal
inferior vena cava filtration- filter device into the femoral vein or jugular vein
trap emboli in inferior vena cava before they progress to lungs
Post-surgical monitoring for complications, particularly for bleeding or infection, is crucial.
Varicose Veins
Result from distended , protruding veins that appears darkened and tortuos often related to prolonged standing or other valvular insufficiencies.
Treatments: Should include conservative measures like elastic stockings, exercise, elevation, or in severe cases, surgical removal (stripping).
sclerotheraphy
an injection of a solution (generally a salt solution) directly into the vein. the solution irritates the lining of the blood vessel, causing it to collapse abd stick together and the blood to clot
endovenous ablation- catheter into the vein and injects an anesthetic agent.
venous Insufficiency
occurs as a result of prolonged venous hypertension, stretching veins and damaging valves
stasis dermatitis- reddish brown discoloration along ankles
stasis ulcers- typically occur of malleolus (medially)
chronic , difficult to heall
Goal/Outcomes
managemnt of edema-compression hose, elevate legs
managemnet of venous statsis ulcers
prevent reoccrrence
surgical mangagement- debridement
Aneurysms of Central Arteries
Aneurysm- permanent localized dilation of artery, enlarging artery of twice its normal diameter
types:
Fusiform- diffuse dilation affecting entire circumference of artey
Saccular- outpouching affecting only distinct portion of artery
dissecting (aortic dissection)- formed when blood accumulated in wall of artery
Abdominal Aortic- tend to occur in the abdominal aorta. are commonly asymptomatic and frequently rupture.
mostly located between renal arteries and aortic bifurcation (dividing area)
Thoracic Aortic- arent as common and frequently misdiagnosed.
commonly develop between the origin of the left subclavian artery and the diaphragn.
they are located in the descending, ascending, and transverse sections of the aorta.
Assessment of Abdominal Aortic Aneurysm
pain in abdomen, flank, back. the pain is usally described as staedy with a gnawing quality, unaffected by movement, and lasting for hrs or days
abdominal mass will pulsate; auscultate for bruits. DONT PALPATE.
assess for severe pain of sudden onset in the back or lower abdomen, which may radiate to the grion, buttocks, or legs.
Rupturing AAA pt are critically ill and are at risk fro hyovolemic shock caused by hemorrhage.
signs and symptoms
hypotension
diaphoresis
decreased LOC
oliguria (scant urine output)
loss of pulse distal to the rupture and dysrhythmias.
rupture into the abdominal cavity causes abdominal distension
assessment of Thoracic Aortic Aneurysm
assess for back pain and manifestations of compression of the aneurysm on the adjacent structures.
signs include
SOB
hoarseness
difficulty swallowing
not usually detected on physical assessemnt
mass may be visible above suprasternal notch
assess pt suspected rupture of a thoracic aneursm fro sudden and excruciating back or chest pain.
diagnostic appearance
XRAY- eggshell appearance
CT/ with Constrast- standard tool for assessing the size/location of ABD/Thoracic Aneurysm
ultrasonography
transesophageal echo (TEE)- done at bedside if pt unstable for other tests to confirm diagnosis of dissection
Nonsurgiacl Management
monitor
monitor aneursm growth
frequent CT or Ultrasound ( small or asymptomatic aneursms)
maintain
maintain BP at normal level to decrease risk of rupture
Educate
educate pt on signs and symptoms of rupture that should be reported IMMEDIATELY
pt with hypertension are treated with antihypertensive drugs to decrease the rate of enlargement and risk for early rupture
Surgical Treatment
Endovascular Stents- procedure of choice.
preoperative care-
operative procedure
stents (wirelike devices) are inserted percutaneously (through the skin), avioding abdominal incisions and therefore decreasing the risk for prolonged postop recovery
Postoperative Care
monitor vs including arterial pressure
may need bedside commode ( stair climbing restricted initially)
activity restrictions, wound care, pain managment
no heavy lifting (15-20 lb) for 6-12 weeks
caution with pulling, pushing, or straining
teach pt receiving treatment for hypertension about the importance of continuing to take prescribed drugs.
report S/S
abdominal fullness or pain or back pain
chest or back pain
SOB
difficulty swallowing or hoarseness
Aneurysms of Peripheral Arteries
Femoral and popliteal aneurysms
massess will pulsate. DONT PALPATE
symptoms- Limb ischemia, diminished or absent pulses, cool to cold skin and pain.
treatment for femoral and popliteal is surgery regarless of sizes'/location
postop - assess for signs of graft occlusion and lower-limb ischemia
palpate pulses below graft to assess patency
dopplar ultrasonography is necessary to assess blood flow when pulses are not palpable
report sudden pain or discoloration of extremity
Aortic Dissection
may be caused by sudden tear in aortic intima, opening way for blood to enter aortic wall
pain described as tearing, ripping, stabbing
life threatening
emergeny care goals
eliminate pain
reduce BP
diaporeis, N/V, fainting, pallor, rapid and weak pulse, and apprehension are common
nonsurgical treatment
uncomplicated distal dissections
SBP less 130-140
Beta blockers (propanolor) and Calcium channel antagonists ( amlodipine)
surgiacl treatment - proximal dissections
Buerger’s Disease
claudication in feet and lower extremities
worsens at night
auses ischemia and fibrosis or vessels in extremities with increased sensitivy to cold
ulcerations and gangrene on digits
causes unknown but associated with smoking
familial or genetic predispostion and autoimmune etiologic factors also possible
TREATMENT
Vasodilators ( nifedipine - procardial)
ulcer management
nursing implication
smoking cessation teaching
aviod cold ( wear gloves and warm clothes
maage stress
aviod caffeine
aviod grapefruit juice to prevent severve adverse effects including possible death
teach pt on vasodilators about side effects - facial flushing, hypotension, headaches
Raynaud’s Phenomenon
painful vasospasms of the arteries and arterioles in extremities (mainly digits)
unknown cause
may be autoimmune associated
occurs in women more than men
treatment
drug therapy- Nifedipine, cyclandelate, phenoxybenzamine
restrict cold exposure
nursing - reinforce pt education
same as buergers’s