Anxiety
Fear and Anxiety
- Anticipation of danger or discomfort
- Tense apprehensiveness
- elevated arousal
- negative affect
- uneasiness
- accompanied by bodily sensations
Fear
- Present orientated (Robinson et al., 2019; Barlow, 2002)
- Danger is imminent, unambiguous and mobilises the organism to take immediate action.
- Rapid behavioural response that leads to active avoidance (e.g. fight-or-flight) or other automatic responses, such as freezing.
- Observed with in specific phobias, and in vivo experience of panic attacks.
Anxiety
- Future orientated (Robinson et al., 2019, Barlow, 2002)
- Threat is more diffuse and uncertain.
- A lasting state of apprehension of potential future threats,
- Accompanied by negative affect, autonomic symptoms, worry, increased vigilance and passive avoidance.
- Excessive anxiety symptoms can be found in GAD and panic disorder (PD)
DSM-5 Anxiety Disorders
- Separation Anxiety Disorder
- Selective Mutism
- Specific Phobia
- Social Anxiety Disorder (Social Phobia)
- Panic disorder
- Agoraphobia
- Generalized anxiety disorder
- Substance/Medication-Induced Anxiety Disorder
- OCD
- PTSD
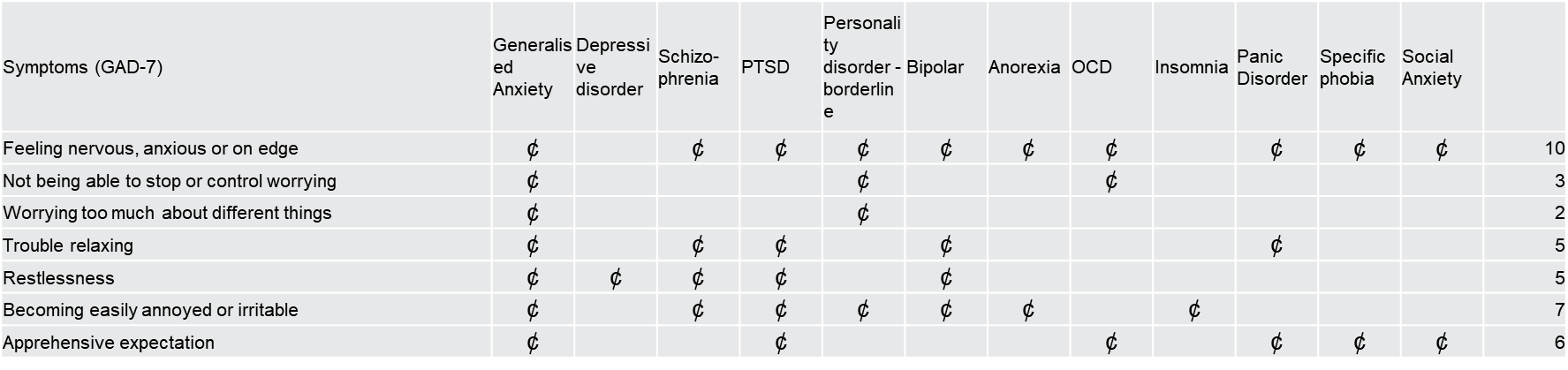
Symptom Overlap
- There is symptom overlap between anxiety disorders, and co-morbidity is common.
- Differentiation relates to antecedents, close examination of the type of situations/objects that are feared or avoided and the content of the thoughts and beliefs
 Epidemiology
Epidemiology
(Somers et al. 2006; Remes et al., 2016; Baxter et al, 2014)
- epidemiology → the study of the distribution and determinants of health-related states or events in specified populations
- Prevalence:
- One-year 10.6%
- Lifetime 16.6%
- Highest
- GAD 6.2%
- Specific phobia 4.9%
- Lowest
- Panic disorder 1.2%
- Cultural Differences
- East Asia 2.8%
- North America 7.7%
- Female : male ratio → 1.9 : 1
- < 35 years most affected by anxiety disorders, irrespective of culture, except Pakistan, midlife (Mirza and Jenkins 2004).
Cultural Variability
- Cultural beliefs\orientation\norms can exacerbate, ameliorate, or alter the symptom presentation and experience.
- Mismatch with DSM criteria (Lewis-Fernández et al., 2011).
- E.g. what is considered “excessive worry” in GAD.
- Expression of distress (i.e. focus on different symptoms)
- Cultural differences in attitudes to anxiety (stigma) “weak-not-sick” (Curcio & Corboy, 2020)
- Panic attacks example (Park & Kim, 2020)
- Cambodia:
- Khyal attacks (involving dizziness, tinnitus, and neck soreness)
- Vietnam:
- Trung gio attacks (involving headaches),
- Latin cultures:
- Ataque de nervios (involving trembling, uncontrollable screaming, crying, aggressive or suicidal behaviour, and depersonalization or derealization).
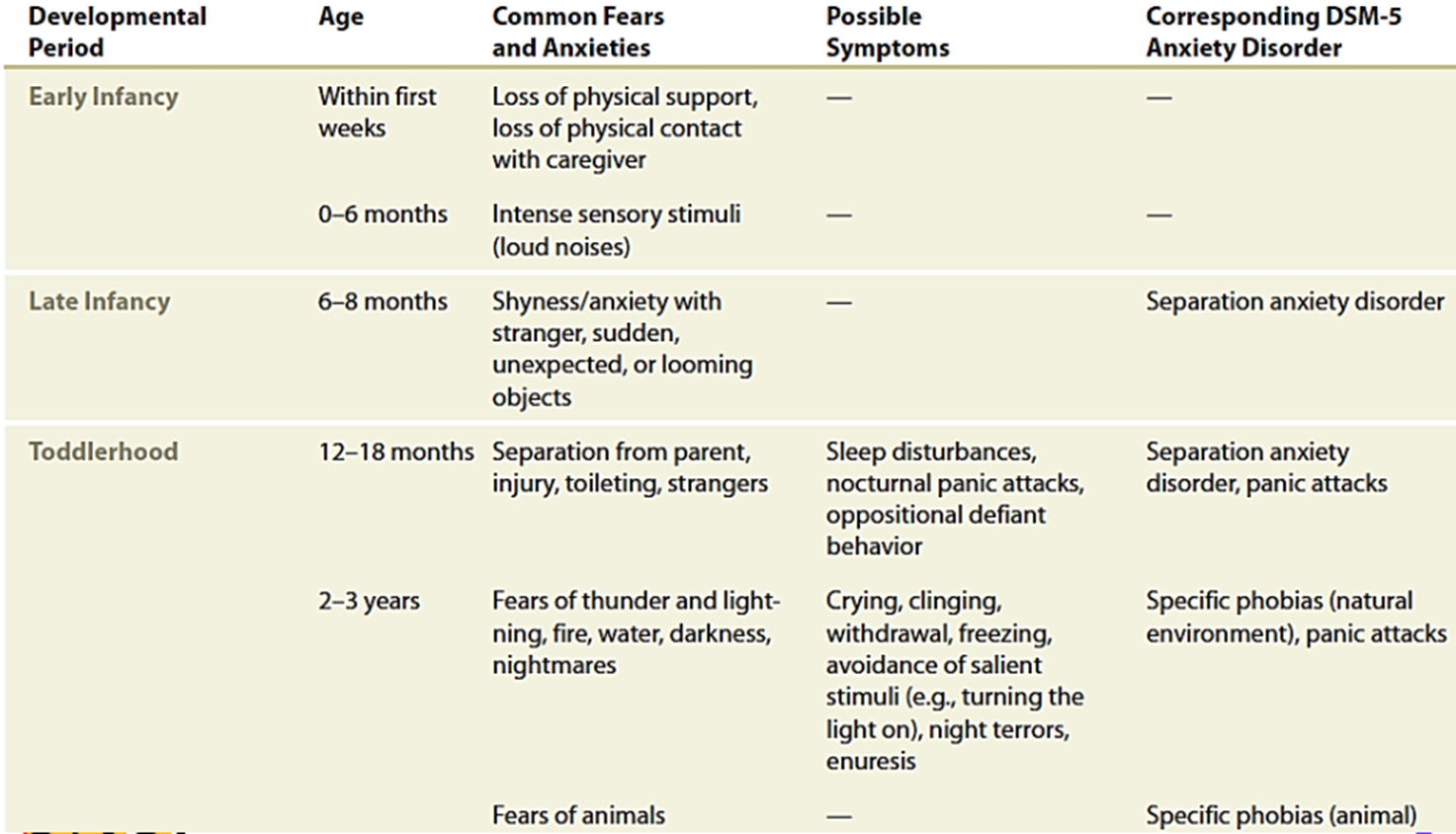
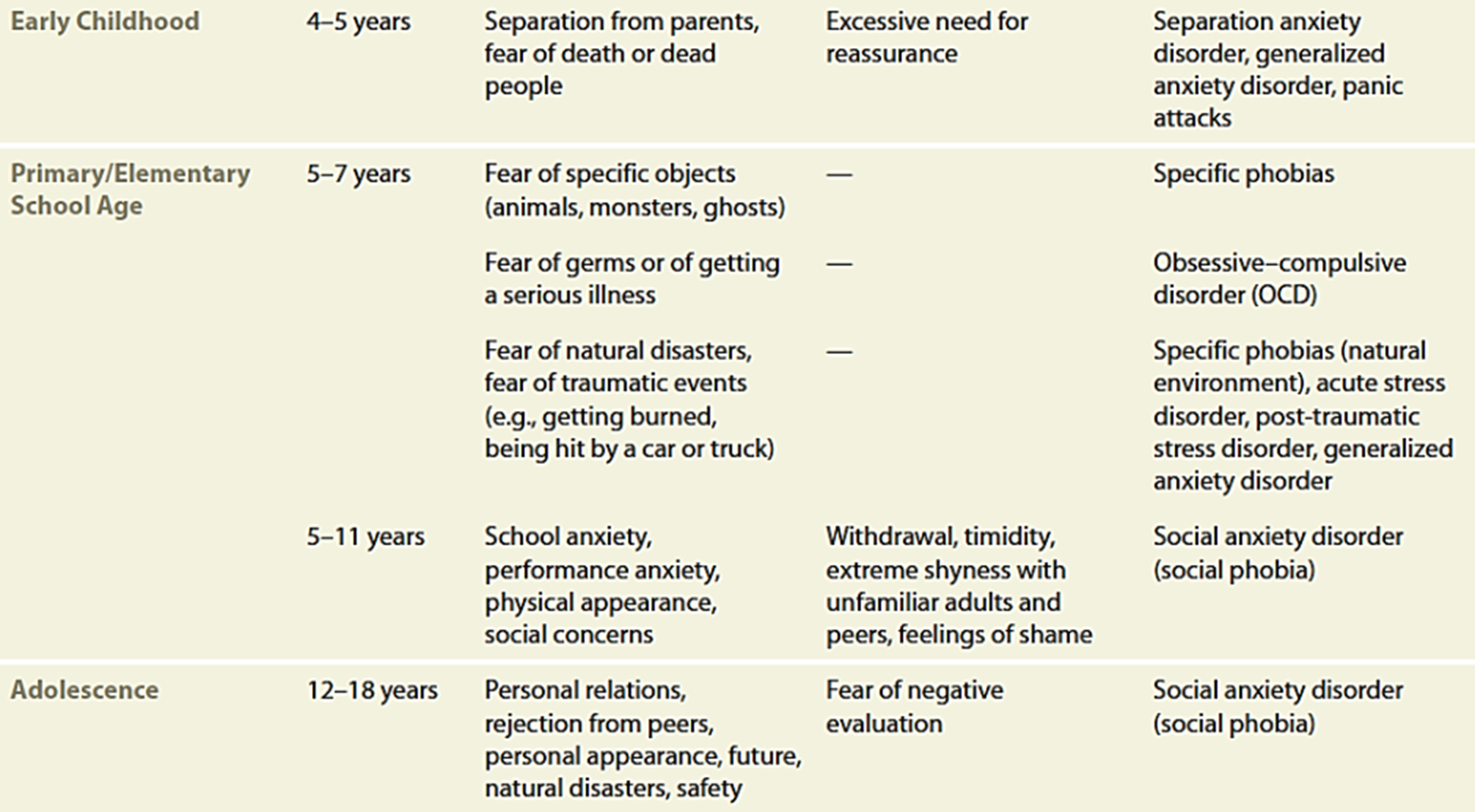
Fears and Anxieties - development
Physiology
- Panic disorder:
- Lactic acid infusion and carbon dioxide inhalation bring out → suffocation response.
- Structures
- Reticular Activation System (RAS) → “suffocation response.”
- HPA axis → downregulation → reduced cortisol (developmental)
- Respiratory system → abnormal responses → low CO2 → greater vasoconstriction → hyperventilation (overcompensation)
- Neurotransmitters
- Catecholamine → “flight or fight reaction” → sensitivity in response to hyperventilation
- GABA receptor → modulation of arousal and anxiety
Early vulnerability factors
Genetic factors and childhood adversity
- Example: Shyness → ‘personality trait’ → temperament
- strongly influenced by genes, combined with childhood experiences that inhibited development of confidence = Heightened rejection sensitivity.
- These play out over the life course – compounding and cumulative experiences.
- Temperamental trait of shyness -> poorer socioemotional functioning
- Shyness strong predictor of social anxiety (Clauss & Blackford, 2012)
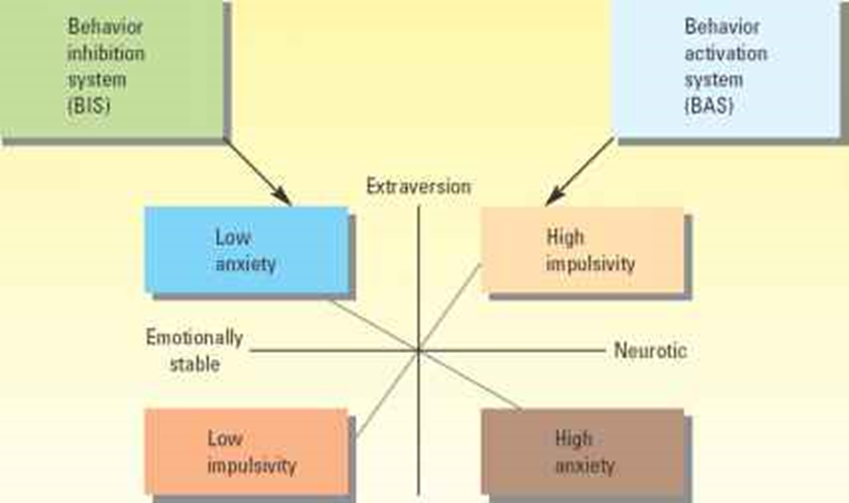
Personality - Eysenck (1967)
- Introverted individuals:-
- Easily aroused (sensitivity of their ARAS).
- Seek less stimulation than extraverts.
- More easily acquire conditioned responses.
- Extraverted individuals in contrast have lower cortical arousal and are less easy to condition.
- However, introverts show weaker classical conditioning under conditions conducive to high arousal
- Impulsivity, not sociability (defining extraversion), is often found to be associated with conditioning effects.
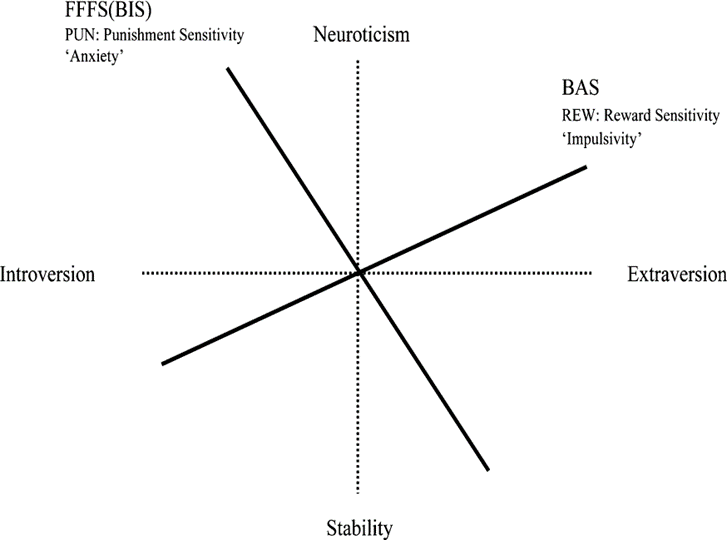
Gray’s Reinforcement Sensitivity Theory (RST)
Innate mechanism, the behavioural inhibition system, leads to development of anxiety
Contrary to Eysenck, extrovert are not slow in conditioning in general but only to fears
Neuroticism indicates heightened sensitivity to reinforcing events
Introversion represents increasing sensitivity to signals of punishment rather than signals of reward
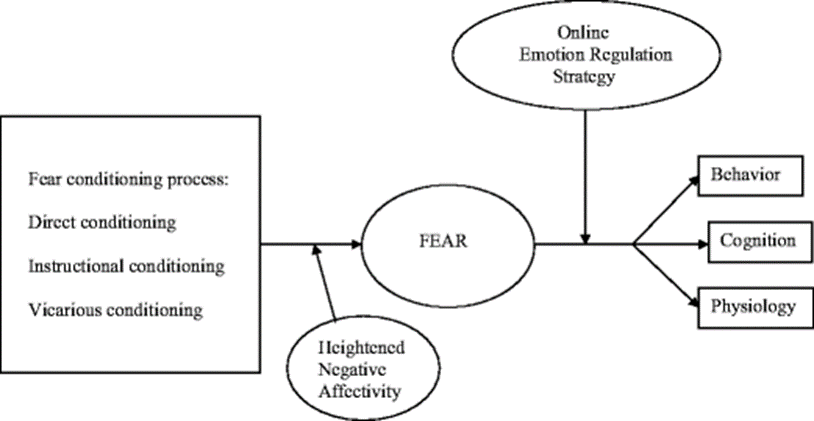
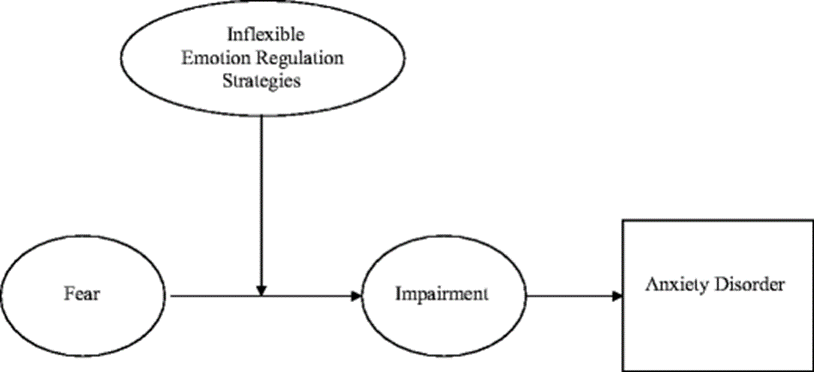
Emotional Regulation
- How one manages negative affects → behaviour (or strategies) are employed to rebalance when experiencing negative affect
- Distraction, avoidance, escape, suppression, emotion and problem-focused coping, and use of substances
- A combination of proneness to negative affect and poor ability to regulate would confer vulnerability to anxiety.
Cisler et al., 2012
Parental influences on emotional regulation
- Parental monitoring and reactivity to infant’s signals enables the infant to learn contingencies between response and outcome
- This provides a foundation for sense of predictability
- Attachment work of Bowlby
- Parental modelling
- Parenting influences the child’s ability to moderate threatening interpretations and approach rather than avoid potential problems
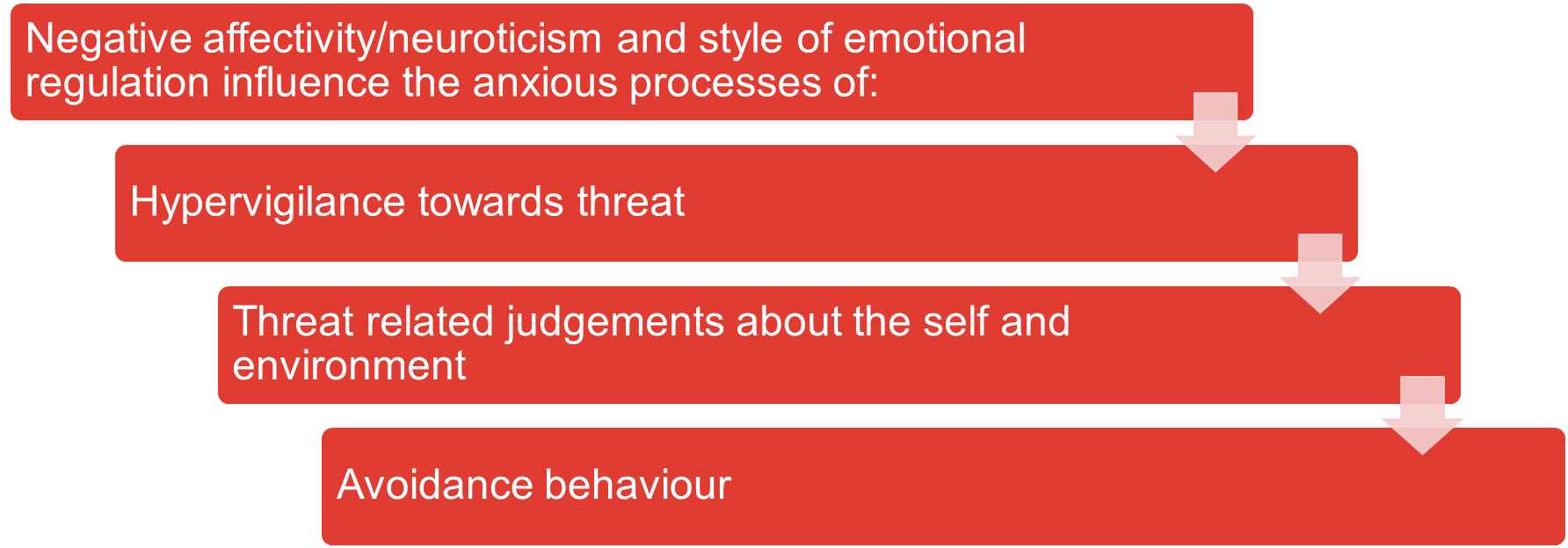
Attention and hypervigilance
- Attentional processes are central to emotional regulation
- Attention bias for threatening stimuli has long been associated with pathological anxiety (Bar-Haim et al., 2007).
- It reflects the propensity to rapidly detect and react to threat, Bias operates at very initial stage of attention to stimuli
- Hypervigilance → a state of high alert, constantly tense and ‘on guard’ and always on the lookout for hidden dangers, both real and presumed
Anxiety Processes - What keeps anxiety going?
Anxiety and attentional bias
- The stroop task
- The emotional stroop task
- Anxiety impedes speed of colour naming of threat words
Evolutionary Perspective
- Being able to efficiently and adequately handle variety of threats is important for our survival.
- A fear system should motivate us to escape or avoid sources of imminent danger
- fast activation of defensive behaviours
- Fear behaviours - moderately imminent threat
- Panic behaviours - immediately imminent threat
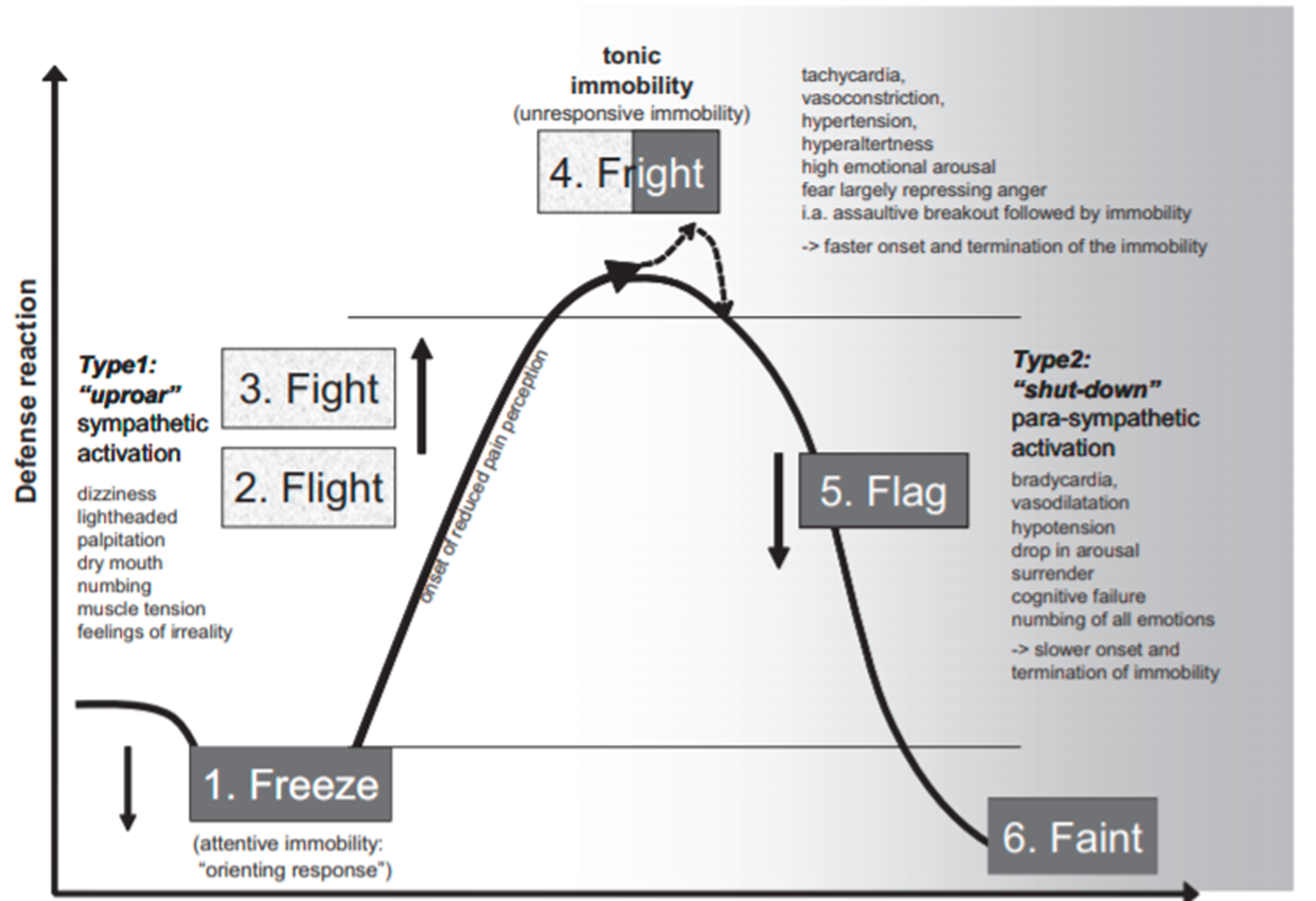
Protective functions
- Freezing/immobility → aids location and assessment of the danger and concealment
- Escape (flight) or avoidance distances an individual from certain threats
- Aggressive defense - harm the source of the danger
- Submission/appeasement is useful depending on probabilities of harm
Fight-Flight-Freeze System Defence Cascade
How are phobias acquired?
- classical conditioning
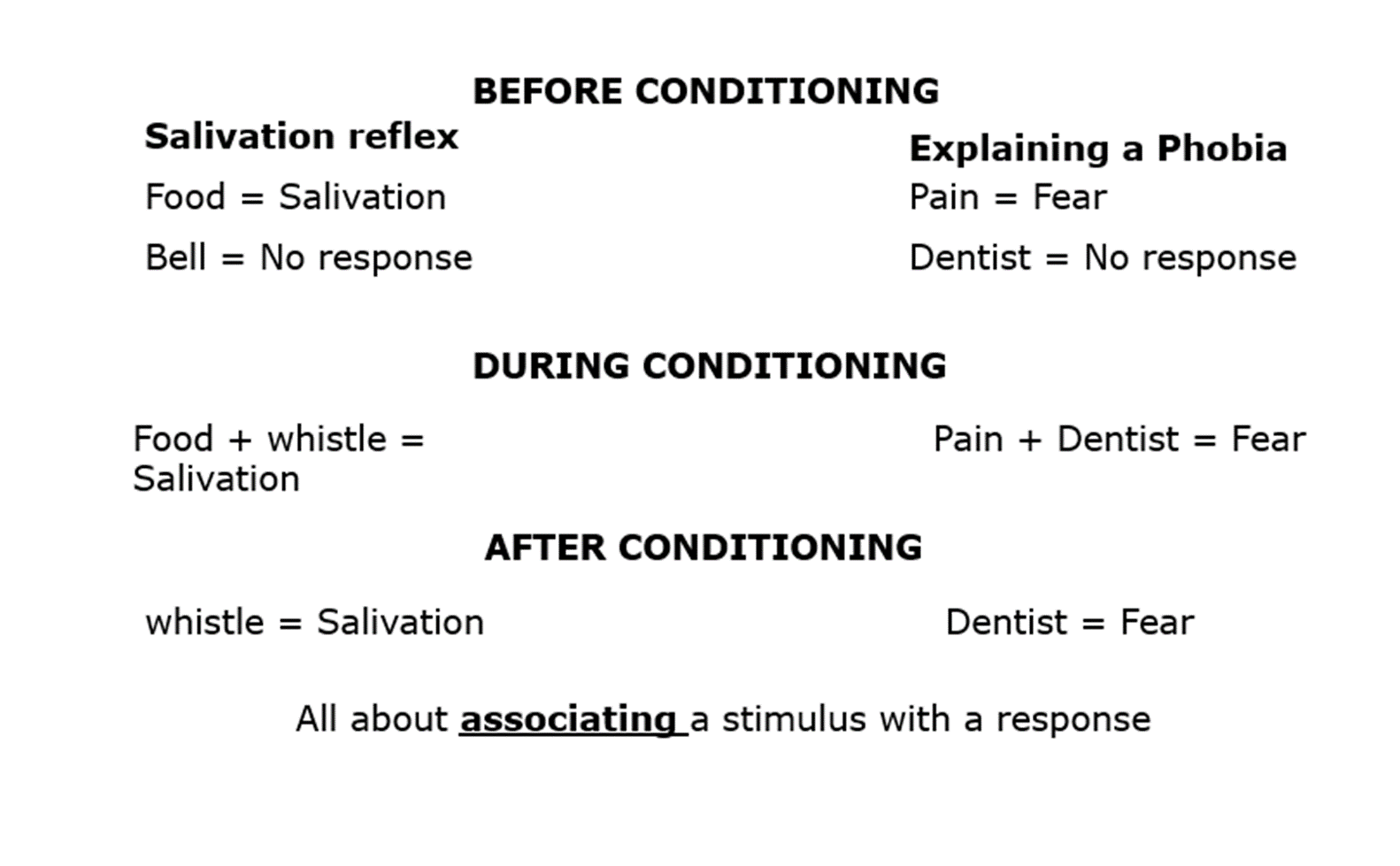
- Components of classical conditioning:
- Unconditioned Stimulus (UCS or US): innate stimuli that trigger reflex
- Unconditioned Response (UCR): fear
- Conditioned Stimulus (CS): sights, sounds, smells, taste and touching
- Conditioned Response (CR): reactions that are triggered by CS
- Example: Litte Albert → Watson & Rayner (1920) → 11 month old Albert paired pet rat (CS) with loud noise (UCS).
Behavioural Terms
Habituation → a decline in behavioural responses, particularly the physiological responses → over repeated exposures to emotionally provoking stimuli.
Extinction → the tendency of previously learned behaviour to decrease in case of non-reinforcement.
- Instead of getting something good to strengthen the behaviour, or having something added or taken away to suppress the behaviour, nothing happens.
Problems with Traditional Conditioning Account
- Patients often can’t recall any trauma (UCS) and not all people who have experienced a trauma paired with a situation develop a phobia.
- Incubation - fear increase over successive non-reinforced presentations of the CS (Eysenck, 1979) but traditional account predicts extinction. [conditioned response acts as a reinforcer]
- Not all stimuli present during associative learning = object of phobia (Lack of equipotentiality of stimuli)
- Some people appear to develop phobia via observational learning
Avoidance learning
This happens when a person engages in a behaviour in anticipation of a stimulus → this prevents the stimulus from occurring.
Slightly different to escape which is a behaviour that terminates a stimulus.
Experiment: Solomon, Kamin and Wynne (1953)
- Dogs trained to fear a light – light + shock
- Light quickly became a CS
- In extinction phase some dogs were allowed to jump over a fence away from floor that had delivered shocks. These dogs continued to show CR to CS
- Whereas, dogs that were not allowed to jump, showed reduction in CR to CS
Two-stage theory of Mowrer (1960)
- Stage 1: Classical conditioning → the previously neutral stimulus takes on the function of eliciting discomfort or anxiety itself.
- Stage 2: Operant conditioning → Fear maintained by behaviours (escape or avoidance) → the reduction of anxiety acts as a reinforcer (negative reinforcement).
How does this apply to phobia?
- A phobia is first acquired through classical conditioning
- Once a behaviour phobia has been acquired it is maintained through operant conditioning
- A behaviour that is reinforced is more likely to be repeated
- A phobic response is unpleasant, so escaping the object or situation causes a reduction in fear (negative reinforcement)
- Will is afraid of lifts, so instead he uses the stairs, which reduces anxiety = reinforces behaviour
Supporting two-stage theory
- Sue et al (1994) → Individuals with a phobia often recall a specific incident to trigger fear
- Barlow & Durand (1995) → 50% of those with driving phobia reported a traumatic experience while driving
- Supports acquisition part of phobia, but doesn’t help explain maintenance
Problems with Mowrer’s theory
- That each object can become a phobic stimulus (CS), provided that it is followed by an aversive event (UCS).
- Not always the case - not all accident survivors developed a fear of driving.
- Avoidance can exist without fear (you can remove the fear but the avoidance can remain)
- Fear of situations can be observed without avoidance (e.g. military situations feared but not avoided)
Mowrer’s theory
- This theory suggests the ‘golden role’ – don’t leave until anxiety has reduced - for successful behaviour therapy.
- Rachman (1986) showed this is not always necessary for successful treatment
- i.e. repeated brief exposure can work even if the person leaves the situation as long as they return.
The contribution of Mowrer’s two factor theory
- The insight that there are two learning processes involved in avoidance:
- Pavlovian learning of fear
- Instrumental learning of avoidance
- We now have alternative models of these two core processes
Gray’s re-working of Mowrer’s two factors
- Safety signals (stimuli that represent the absence of threat) are used to explain persistence of anxiety disorders.
- They are signals from which the expected punishment will not occur.
- Safety signals reduce fear and provide secondary reward for the avoidance response
- Fear generates escape/avoidance and search for safety
Contemporary conditioning approach
CS does not become a substitute for the UCS
Two things are learned from pairing of CS with a UCS:
- a CS-UCS association
- a representation of the UCS.
The CS elicits the CR because of its association with the UCS representation.
- If either the CS-UCS association is weak or the UCS representation is weak, the CR will be correspondingly weak
It’s the correlation between CS and UCS that matters
- If stimuli has previously been paired with other UCS (or nothing at all) then the correlation between the CS and the new UCS will be weaker
- i.e. if you have had many trauma-free experiences with a stimuli it will be much harder to subsequently associate that stimulus with a trauma
Vicarious Learning
- In modern accounts, it is accepted that you can learn the association between CS and UCS by being told what the contingency is or by observation
Social Learning Theory
- Behaviour (of a role model) is observed and then copied. Imitation or modeling.
- Unlike classical and operant conditioning, SLT takes into account cognitions.
- SLT is the bridge between learning theory and the cognitive approach.
- These mental factors mediate in the learning process to determine if a response is acquired.
UCS Revaluation Processes (Davey, 1989)
- The strength of the CR will be affected by any factor which changes knowledge about the UCS contained in the UCS representation
- Different from signal or Pavlovian learning, in which the CS acquires a predictive value, the CS in this paradigm attains the affective quality of the UCS.
- Usually explained by the formation of an association between the cognitive representation of the CS and the UCS
- Exposure to the CS after repeated pairings with a UCS will activate the representation of the UCS, which in turn activates its corresponding response (S–S learning)
- Cognitive learning involves learning a relationship between two stimuli and thus is also called S‐S learning
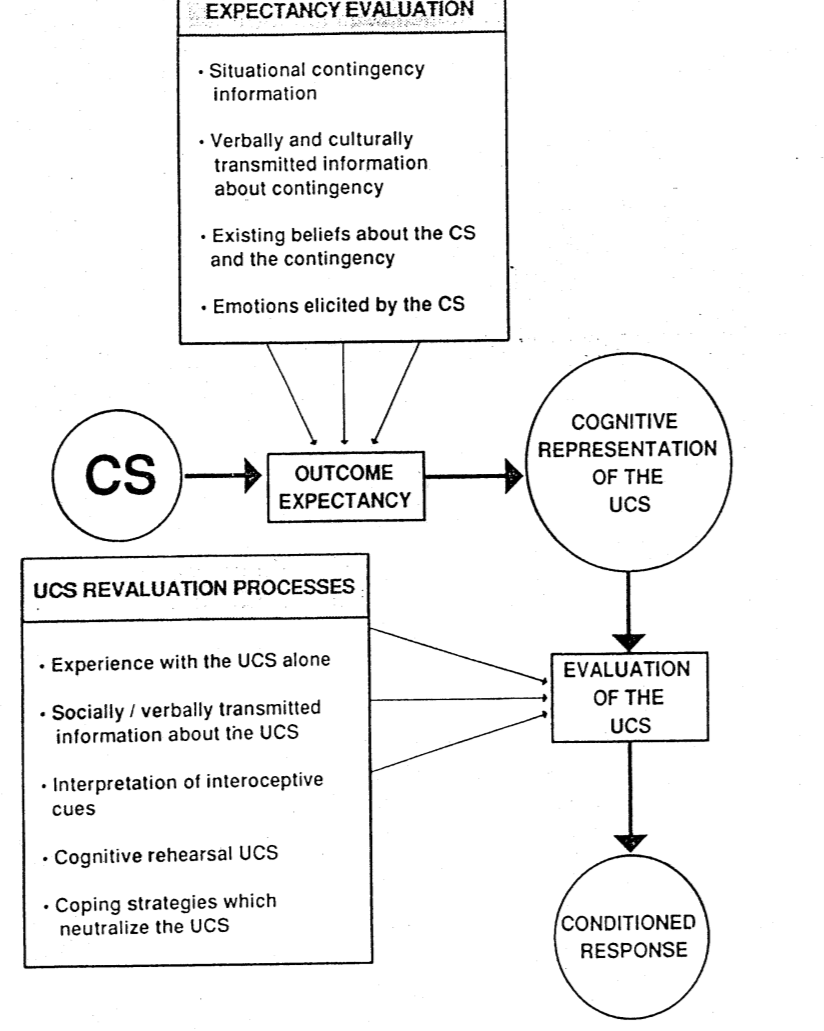
Verbal Information about the UCS
- It is much easier to use verbal information to increase the aversiveness of the UCS than to reduce the UCS
- i.e. post-conditioning verbally transmitted information about a consequential UCS can increase the aversive evaluation of the UCS
- Rehearsing the UCS after conditioning produces larger CRs to subsequent test presentations of the CS Interpretation of interoceptive cues - subjects may perceive what they believe to be a strong CR and attribute this to the fact that they must still frightened
Direct traumatic conditioning versus non associative accounts
- Some phobia do seem well explained by direct conditioning experiences
- e.g. dental phobia, dog phobia, accident phobia and choking phobia
- height phobia, snake phobia, spider phobia and water phobia do not seem to regularly involve direct conditioning experiences
Non-associative account (Poulton, 2002)
- Most people will show fear to a set of biologically relevant stimuli
- i.e. phobias result from innate fears shared by all humans
- Biological and Evolutionary preparedness/Genetic mechanisms
- The notion that the role of the environment is to abate biologically relevant fears, rather than account for their emergence, is at the heart of the non-associative position
Pathways to development of clinical anxiety
- Environmental learning pathways
- Direct conditioning
- vicarious learning / modelling, and transmission of misinformation
- Non-associative pathways
- Biological and Evolutionary preparedness
- Genetic mechanisms
Why we avoid?
- Expectation of unpleasantness
- over-prediction of fear
- Availability of safety
- safety signal e.g. partner
- Motivation
- Avoidance indicates a propensity to move away from (or maintain distance from) an undesired stimulus.
- Motivation is defined as the energization and direction of behaviour.
Behaviour Therapy Methods
- In vivo exposure: Directly facing a feared object, situation or activity in real life.
- For example, someone with a fear of snakes might be instructed to handle a snake, or someone with social anxiety might be instructed to give a speech in front of an audience.
- Imaginal exposure: Vividly imagining the feared object, situation or activity.
- For example, someone with Posttraumatic Stress Disorder might be asked to recall and describe his or her traumatic experience in order to reduce feelings of fear.
- Virtual reality exposure: In some cases, virtual reality technology can be used when in vivo exposure is not practical.
- For example, someone with a fear of flying might take a virtual flight in the psychologist's office, using equipment that provides the sights, sounds and smells of an airplane.
- Interoceptive exposure: Deliberately bringing on physical sensations that are harmless, yet feared.
- For example, someone with Panic Disorder might be instructed to run in place in order to make his or her heart speed up, and therefore learn that this sensation is not dangerous.
- Flooding expose the client to anxiety arousing stimuli for prolonged durations.
- Flooding deals with the actual stimulus or its image, while in implosion therapy anxiety is aroused by only imagining the simuli (without direct contact).
- Further, implosive therapy involves imagined scenes that are often exaggerated by a therapist
Habituation and Sensitisation
Habituation: a decline in fear responses, particularly the physiological responses, over repeated exposures to fear provoking stimuli
The emphasis is on confronting feared stimulus through exposure and reducing avoidance.
Habituation is the mechanism of change
Decreases in responsiveness produced by repeated stimulation are referred to as habituation effects
Increases in responsiveness are called sensitization effects
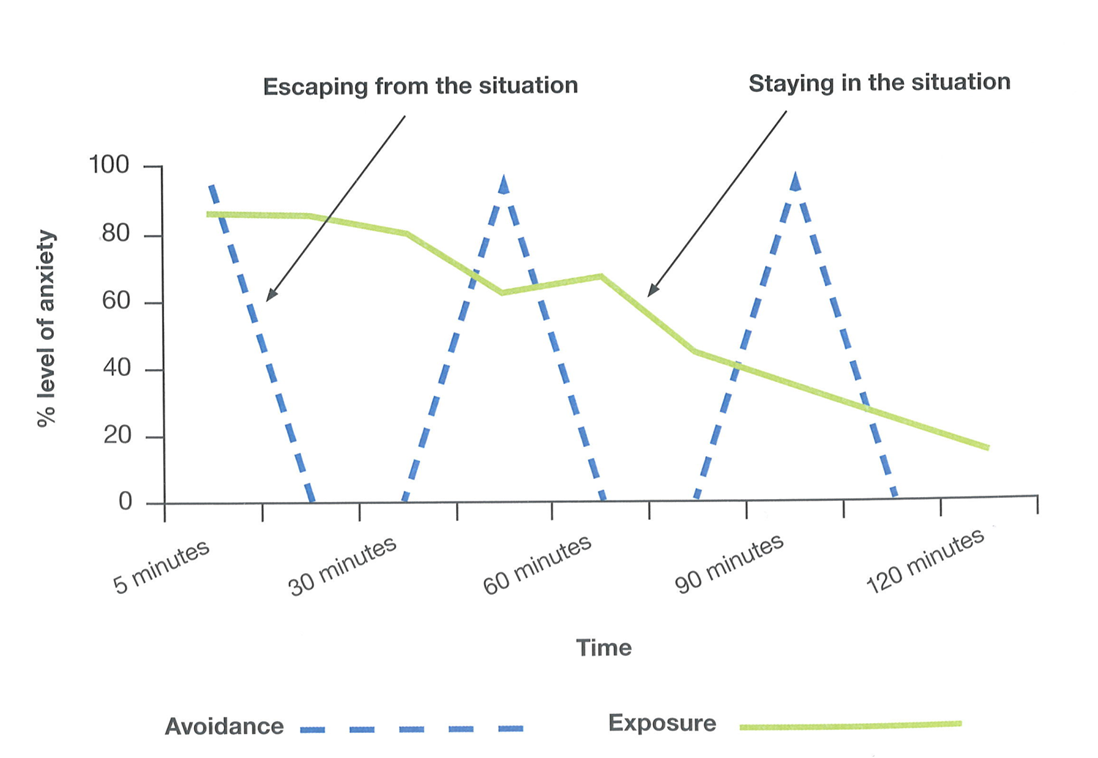
Extinction
- Extinction: anxiety reduction results from repeated encounters with anxiety provoking situations without aversive consequences (minimal anxiety response)
- Refers to decrements in responding through repetition of unreinforced responding
- i.e. non-fearful pairing is generated through repeated encounters with feared stimuli without aversive consequences
- During extinction, inhibitory meaning is learned (‘on-top’ of excitatory meaning).
- There is new learning (ie mental representations are altered) can be indirect.
- Thus the CS comes to have a dual meaning resolved only by the current context of the CS
Exposure therapy
- During exposure treatment new memories are developed that compete with intact older memories
- e.g. experiencing petting a dog without being bitten
- During treatment the storage strength of the old fear representation is unchanged
- but its retrieval strength decreases as the competing representation gains strength.
Panic Disorder
- is characterized by recurrent, sometimes unpredictable, panic attacks.
- A panic attack consists of intense apprehension, fear and discomfort of sudden onset, with no immediately determinable cause.
Some medical conditions can cause panic attacks. For example:
- hyperthyroidism
- hyperglycemia
- pheochromocytoma (a catecholamine producing tumor
- temporal lobe epilepsy
Distinctiveness of Panic Disorder
- Klein in late 1950s found benzodiazepines not effective but imipramine (anti-depressant) was.
- Infusion of lactate in patients with PD induced panic.
- According to Klein’s biological model spontaneous panics are the result of the false firing of a suffocation alarm system
- i.e. mechanism for detecting CO2 dysfunctioning
- Problems with Klein’s model
- Anti-depressants work for a range of anxiety disorders
- A number of patients with panic disorder do not respond to lactate-infusion test and a number respond to placebo infusions
- Diverse range of chemicals can induce panic
- Klein’s model does not explain why more women than men develop panic disorder
Fear as a biologically derived CNS response
- True alarms - ‘fight or flight’ when confronted with real danger or threat
- False alarms occur in the absence of real threat (e.g. panic attack)
- Learned alarms – because of false alarms inherently unpleasant they become associated with internal or external cues
Psychological cause of first panic attack
- attack is a climatic consequence of anxiety that is unusually high or prolonged
- interpersonal conflict, death or illness of a significant other and drug reactions are very often in the background to first panic attack
Role of hyperventilation in panic
- Most people hyperventilate when anxious
- For some individuals even small amounts of over-breathing elicit such symptoms as dizziness, shortness of breath and tingling of the extremities.
- Symptoms of hyperventilation precede full blown panic
Classical conditioning model - First panic attack to panic disorder
- First panic attack is an UCR to hyperventilation
- Just as an external cue (e.g. tone) can be established as CS by predicting an aversive UCS so can an internal cue (e.g. dizziness) be established as a CS by predicting panic attack
- i.e. panic is a CR to interoceptive stimuli → CS (Goldstein and Chambless, 1978)
- Viewing panic as a CR to internal sensations led to treatment where patients are desensitized to bodily sensations → interoceptive exposure
Problems with interoceptive exposure conditioning model of panic disorder
- Razran (1961) demonstrated interoceptive conditioning in laboratory using clearly distinct ‘events’ in the dog
- With panic attacks the ‘events’ are not so clear
- how do you say which bodily events are CS and which are CR - does ‘skipped heartbeat CS’ elicit ‘dizziness CR’ or vice versa.
- The events indexing the CS (e.g. heart rate) are the same as those indexing the CR (e.g. a further increase in heart rate)
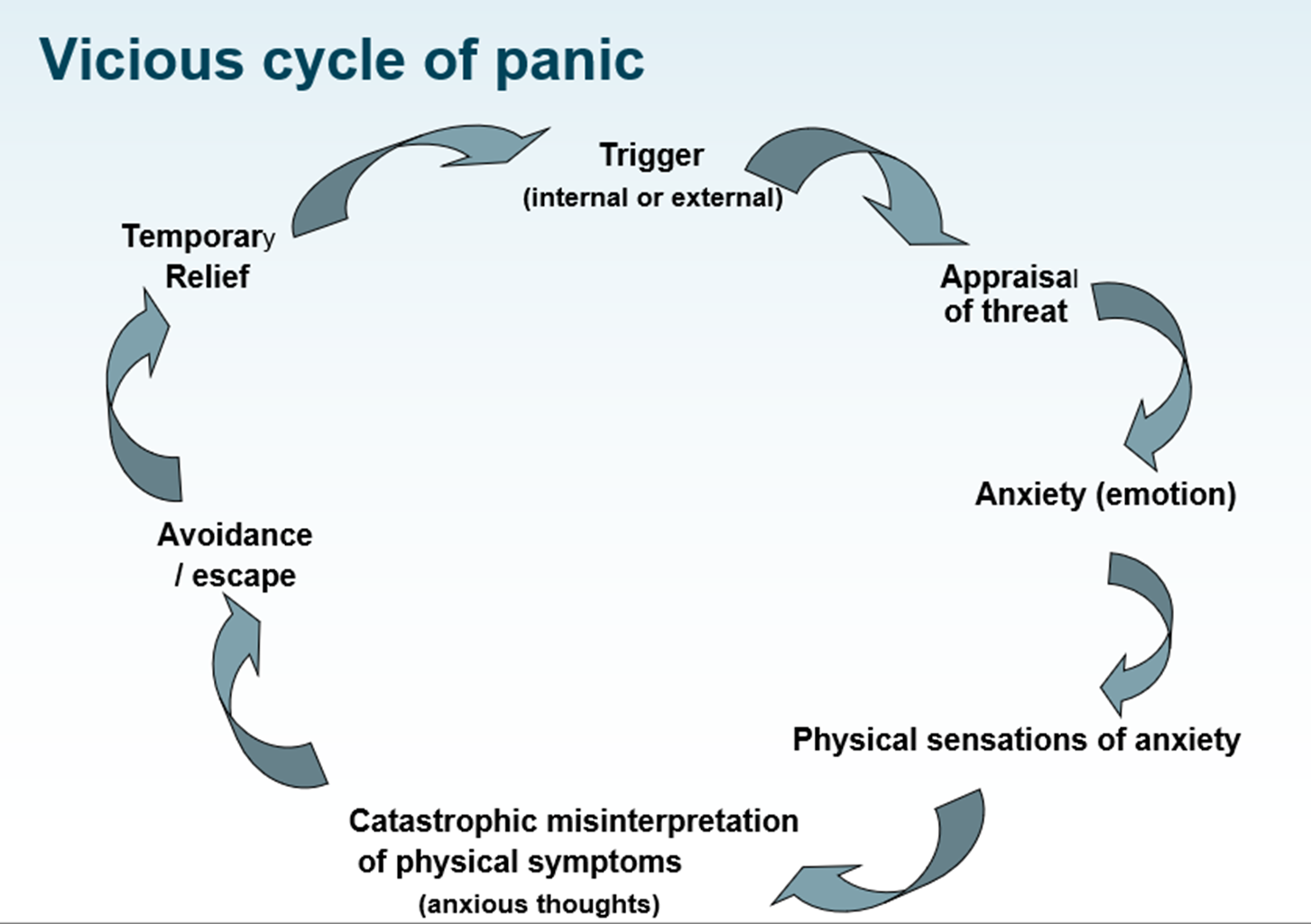
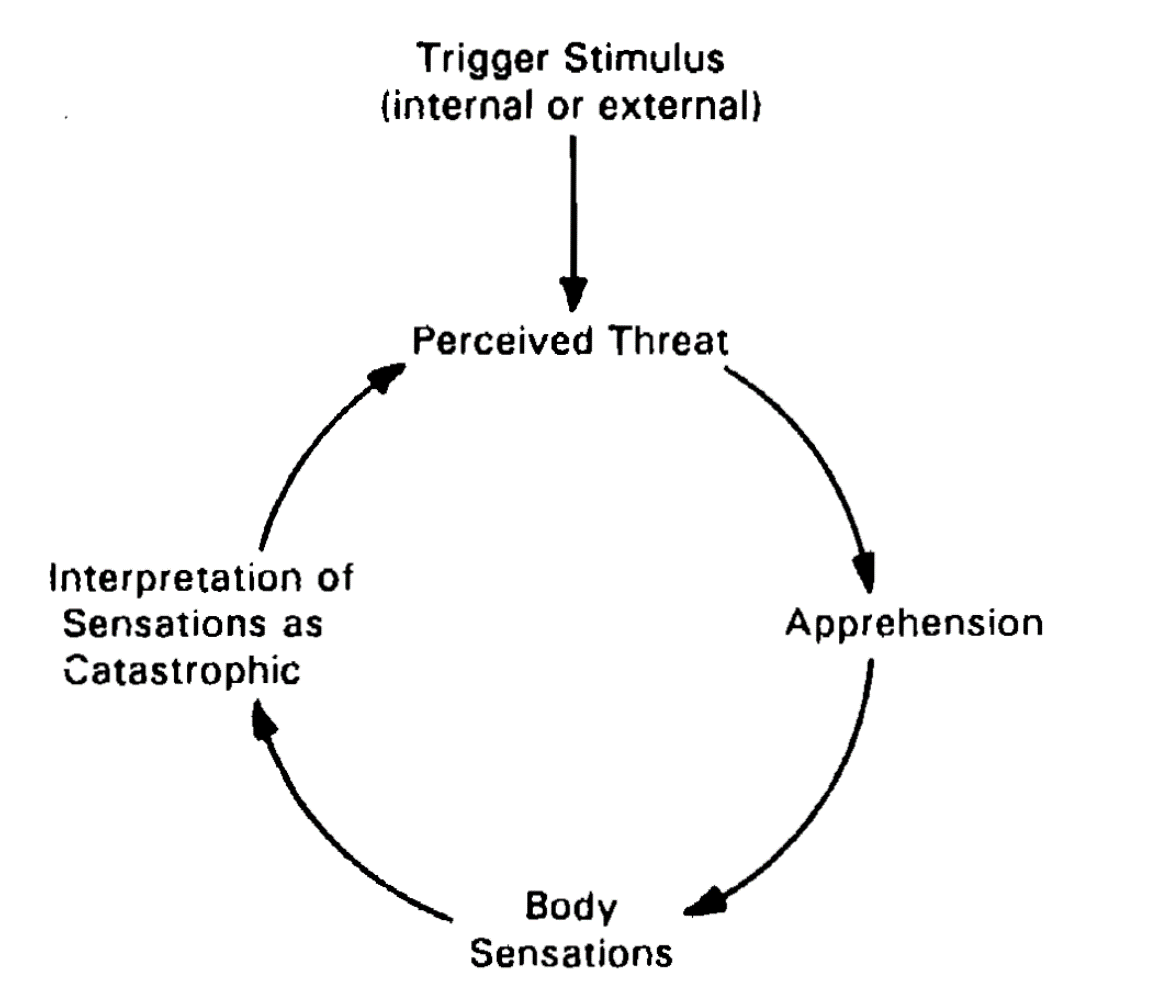
Cognitive therapy model of panic disorder
Catastrophic Misinterpretation of Bodily Sensations
Clark (1986)
Events only lead to panic if the unusual bodily sensations they produce are catastrophically misinterpreted
- e.g. substance give to non-panic patients do not lead to panic
Catastrophic misinterpretation need not be conscious
Catastrophic misinterpretations persist because of “safety behaviours”
- i.e. avoidance
Some patients require rigorous demonstrations (behavioural experiments) for them to abandon their beliefs whereas others immediately convinced that the symptoms are harmless once symptoms explained.
Behavioural Experiments are a cognitive intervention in which you are testing out predictions, graded exposure is a behavioural intervention.
Anxiety Sensitivity (Reiss & McNally, 1985)
- Anxiety sensitivity refers to preexisting beliefs about the consequences of bodily sensations and anxiety
- Anxiety sensitivity is a dispositional construct conceptually and empirically distinct from trait anxiety
- Anxiety sensitivity=fear of anxiety symptoms.
- Trait anxiety = fearful in general
Fear of Anxiety Model
- Previous explanations for the re-occurance of panic attacks in panic disorder was the ‘fear of anxiety model’(Goldstein & Chambless, 1979)
- A fear of anxiety through its association with interoceptive cues leads to a fear of panic symptoms.
- Clark model disputes this and puts at the centre the belief about the meaning of the symptoms
Beliefs
- beliefs can be acquired in many ways not solely as a result of a panic attack
- anxiety sensitivity refers to beliefs not conditioned fear responses
- level of anxiety sensitivity highest in panic disorder, lowest in phobic disorders
Effectiveness of treatment
- For Panic Disorder CBT should be first line treatment. 80-90% of patients who receive CBT are panic free at end of treatment (Clarke, 1997)
- Little evidence to support the use of pharmacological and psychological interventions in combination
Summary of cognitive account of anxiety
- All anxiety-related phenomena arise from cognitions of threat or danger.
- Acquisition of anxiety problems is learned as in behavioural account (different terms to describe what is learned). The approaches differ in terms of maintenance.
- Cognitive account of maintenance is that the focus of avoidance is feared outcomes, not feared stimuli or seeking relief from anxiety as in behavioural account
Medication commonly used in the treatment of anxiety disorder
- Anxiolytics (benzodiazepines & Azapirones e.g buspirone) especially for generalized anxiety disorder.
- High risk of dependency for benzodiazepines
- eg valium
- Benzodiazepines are indicated for the short-term relief (two to four weeks only) of anxiety that is severe, disabling, or causing the patient unacceptable distress, occurring alone or in association with insomnia or short-term psychosomatic, organic, or psychotic illness.
- Antidepressants (tricyclic antidepressants, MAOIs & SSRIs) have anxiolytic as well as antidepressant effects
- Beta blockers (Beta-adrenergic inhibitors) help control tremor and palpitation in social phobia
- Beta blockers reduce anxiety by decreasing heart rate and preventing shaking.
- do not reduce non-autonomic symptoms, such as muscle tension.
- Beta-blockers are therefore indicated for patients with predominantly somatic symptoms; this, in turn, may prevent the onset of worry and fear.