WK 1 Advanced Imaging and Contrast
Anatomical slices/sections
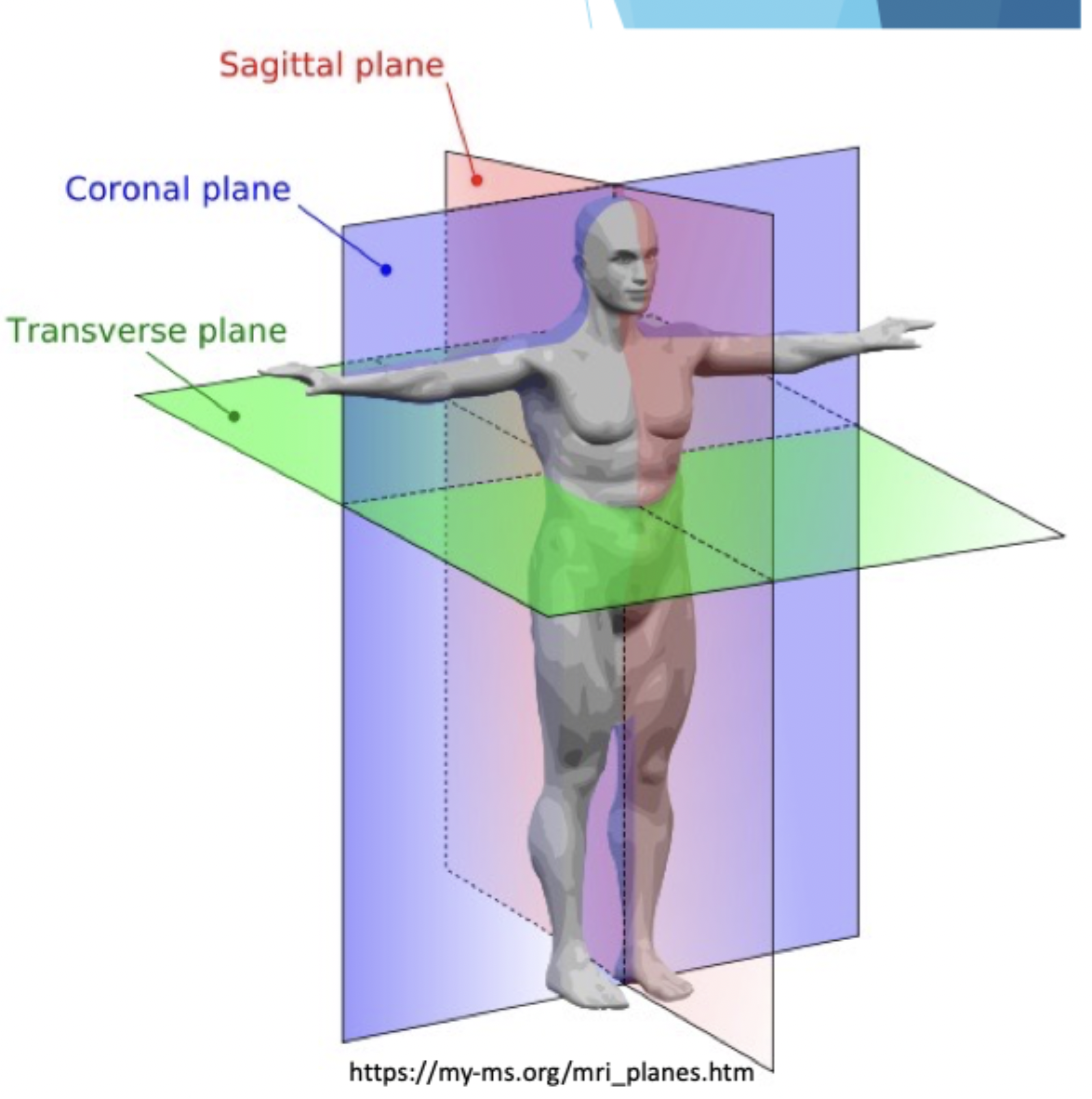
Sagittal (median/mid-sagittal, parasagittal): cuts into the right and left side
Coronal/frontal: separates front and back
Transverse/Axial/Horizontal: separates upper and lower part
Oblique/angled: between other planes
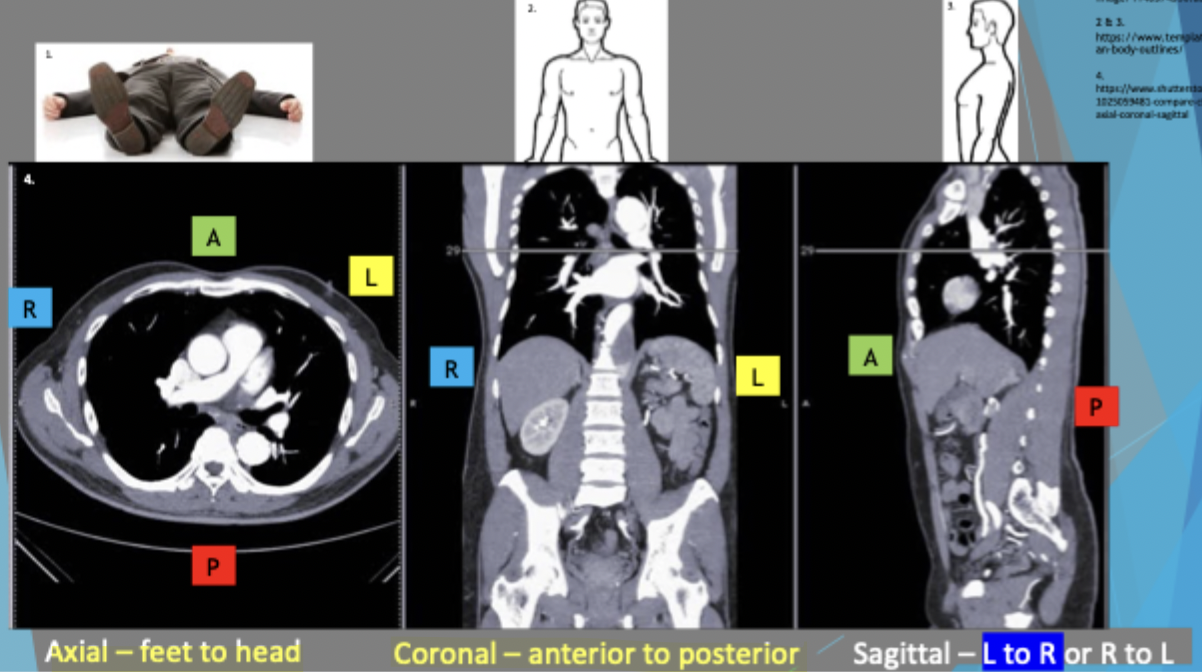
Viewing and orientation
Axial is looking from feet to head, anterior is superior in the image and posterior is inferior
Coronal: looking at patient face to face and anterior side is separated so you’re looking at posterior side
Sagittal: L to R or R to L. Left to right = seeing right side as left is cut away
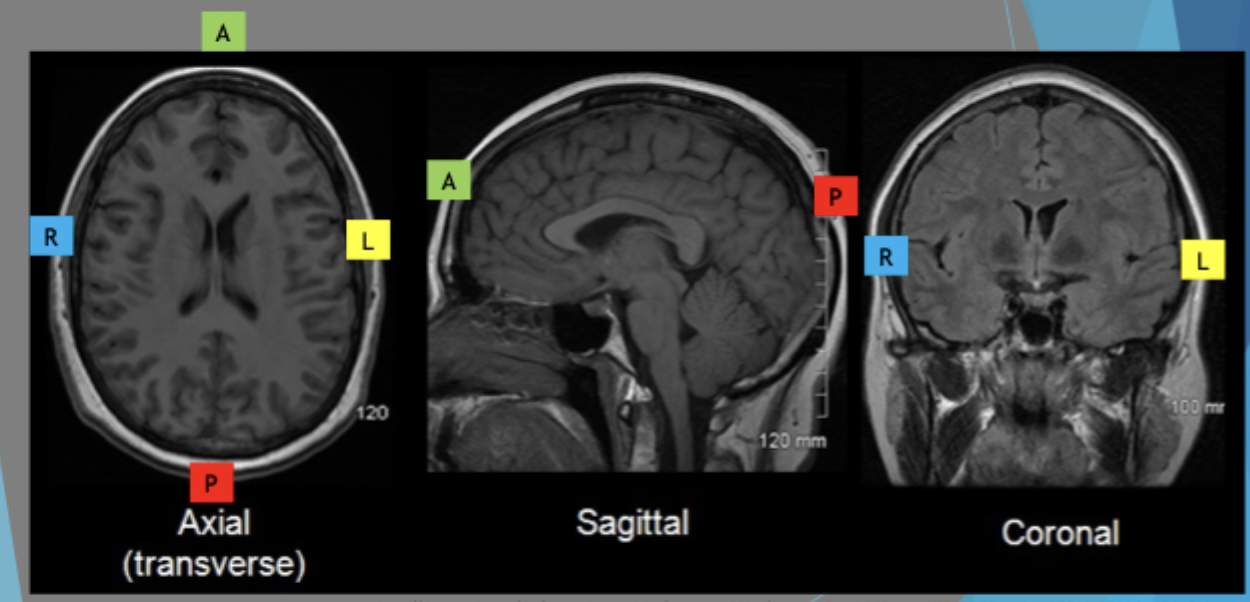
Brain and skull anatomical viewing and orientation
Axial skull: feet from the top of the head - cutting away body and looking at the head from underneath
Skull is narrower and more pointed in the front, rounded at the back
patient lying their back so L and R is opposite from you
Sagittal is left or right side cut away so you’re looking at the other side
Coronal is the patient looking at us but the face is separated and we’re looking behind
Contrast
Definition: obvious difference between two or more things - light and dark areas on an image. Difference in densities
High contrast = few shades of grey between black and white - easy to differentiate
Low contrast = more shades of grey - able to see more detail
Good contrast = can see what is needed
Resolution and visual acuity
Resolution: measured of sharpness of an image with which a device can produce or record an image based on the number of pixels - how sharp an image can be demonstrated with pixels (high end vs low end MRI)
Visual acuity: measure of the ability of the eye to distinguish shapes and the details of objects even at a given distance
Contrast types
Innate/natural:
Tissues (density/atomic mass of tissues - more compact organ = higher density)
Gases (eg. gas in stomach)
Liquids: high in density
Administered (introduced)
Contrast media - adding something to increase/decrease the density
Chemicals (heavy metals) - iodine, barium and gadolinium which all increase density
Gasses introduced - decreases density
Positive contrast adds density/colour - increases signal
Negative density reduces density and colour - decreases signal
Contrast media administered when tissues have similar densities and look similar in imaging - fat and water
Contrast media
Routes and terms
Orally to see GIT lumen
Installation - rectally placed or into ducts/cavities
Injected into blood - intravenous (IV) or intraarterial (IA)
Injected - intrathecal (spinal canal), interosseous (into bone)
Retrograde (against flow - rectal enema) vs anterograde (with flow - barium swallow)

Contrast enhanced image
Barium and gas added
Lumen can be seen well
Double contrast as barium can close up the tube so gas is added afterwards to mimic the natural shape of the large intestines
Contrast media types
Barium based: x-ray, CT, fluro, angio, venography
Into the GIT
Not water soluble - cannot be excreted through kidneys so it needs to be expelled through faeces
barium must be used in a tube only
Iodine based: into GIT or into blood stream (IV/IA)
Water soluble - cleared through kidneys and urinary tract - also faeces
Health of kidney (eGFR) needs to be determined beforehand - if not healthy or diseased it can be cleared through faeces
Barium based contrast media
used to visualise GIT
Orally ingested for barium swallow (pharynx, oesophagus and stomach) and barium follow through (duodenum, jejunum and ileum) or rectally instilled for barium enema (large intestines, rectum and anus - find tumours and distension
Commonly added with gas to inflate the bowels - called double contrast
Contraindications: suspected perforation in GIT, vomiting, swallowing issues, toxic megacolon, pregnancy, ulcerative colitis
Iodinated contrast media
Categorised as;
non ionic (molecules stay together) or ionic (molecules can break up and become ions)
Ionic has higher rates of complications and HO but used for GI and lower rectal system when barium cannot be used
Non-ionic has lower rates of complications and LO, commonly used for IV, IA, intrathecal
High osmolarity (increases concentration by drawing in water) or low osmolarity (doesn’t draw in water or increase concentration)
Reactions to iodinated contrast
Very mild: nausea
Mid-range to severe: renal impairment/failure
Severe: anaphylactoid, angioedema, bronchospasm (airway constricting) and cardiac arrest (heart attack)
most severe reactions occur 20-30min after administration and in IV injections
Hives are common and itchiness
Anaphylactoid vs anaphylaxis
Anaphylactoid reactions:
not IgE related so the immune system doesn’t activate it
can be mild, moderate or severe
occurs with first time exposure
more likely to have a second reaction upon re-exposure - this is anaphylaxis
treated with adrenaline
Anaphylactic reactions
immune system initiates response (IgE)
requires first exposure - priming
likely to have follow up reactions with increasing severity after re-exposure
treated with adrenaline
Injected idoniated contrast media causes water to enter the vessel due to increased concentration
Water moving into the lumen from the vessel wall cells causes then to become stressed and release histamine
Mast cells sitting in the tissues release large amounts of histamine
Histamine causes vasodilation in the blood vessels which causes it to not function properly and reduce its volume
This causes the patient to undergo a decrease in blood pressure and oedema
Swelling (oedema) of the bronchial tree can restrict breathing - most severe anaphylactoid reaction
when adrenaline is injected it causes the blood vessels to restrict and reverses all the processes