ANA 877 Antiarrhythmics Lecture
Introduction to Antiarrhythmics
Focus of the lecture: antiarrhythmics.
Reference materials: Stolting Chapter 21, Nagel Hout Chapter 13 for supplementary information.
Importance of understanding cardiac conduction and EKG interpretation to grasp antiarrhythmics.
Cardiac Conduction System
Overview of key components in the cardiac conduction system:
SA Node: initiates the impulse.
Internodal tracts: pathways for impulse propagation. Three key tracts:
Anterior internodal tract (Bachmann bundle)
Middle internodal tract (Winkiebach tract)
Posterior tract (Thurall tract)
AV Node: relays the impulse to the ventricles.
Bundle of His: transmits impulses from the AV node to the bundle branches.
Bundle branches: carry impulses to the ventricles.
Purkinje fibers: distribute impulses throughout the ventricles.
Arrangement of conduction pathways: SA node → 3 internodal tracts → AV node → Bundle of His → Bundle branches → Purkinje fibers.
Conduction Velocity
Definition: speed of electrochemical propagation along the neural pathway.
Influencing factors:
Resting membrane potential
Amplitude of action potential
Rate of change during phase zero
Influencing elements:
Autonomic tone
Electrolyte imbalances (hyperkalemia, acidosis)
Ischemia
Antiarrhythmic drugs.
Comparative speed of conduction:
SA and AV nodes: m/s (relatively slow).
Myocardial muscle cells: 0.3-1m/sec (intermediate speed)
Bundle branches and Purkinje fibers: 1-4 m/sec (faster conduction.)
EKG and Cardiac Action Potential
Slide introduction to EKG components and mechanical events.
EKG: graphical representation of electrical activities of the heart.
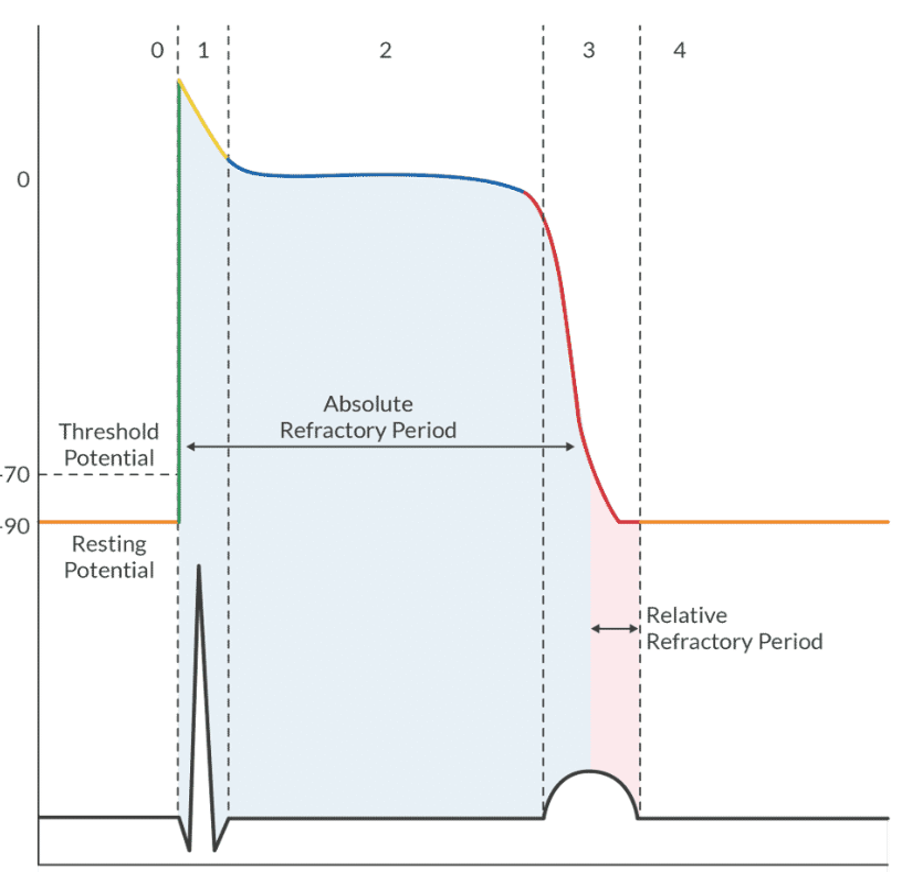
Ventricular Action Potential:
Absolute refractory period: myocytes cannot be depolarized.
Relative refractory period: requires larger stimuli for depolarization.
KNOW DIAGRAM (HD monitoring APEX)
Wiggers Diagram: illustrates phases of the cardiac cycle, including:
Atrial and ventricular pressures.
Valves open and close at distinct times.
Heart volume changes during different phases: passive filling, active filling, diastasis.
Phases of the Cardiac Action Potential
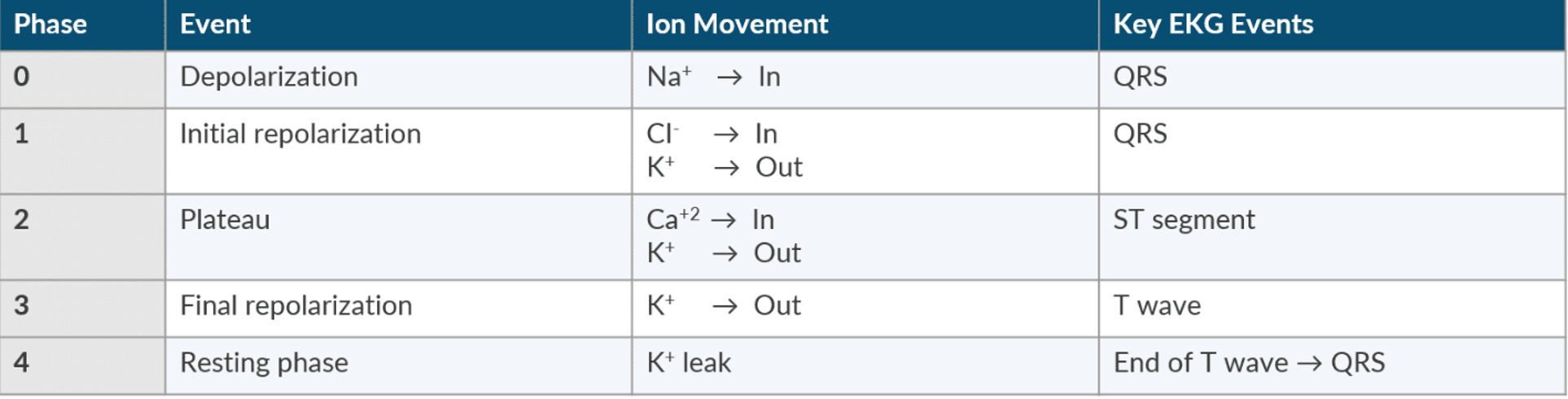
Detailed breakdown of action potential phases:
Phase 0: Rapid depolarization (sodium influx).
Phase 1: Initial repolarization (chloride influx, potassium efflux).
Phase 2: Plateau (calcium influx, continued potassium efflux).
Phase 3: Final repolarization (potassium efflux).
Phase 4: Resting phase (gradual potassium leak).
Important EKG events correlating with action potential phases are crucial for understanding arrhythmias.
Discussion of EKG Disturbances
Common EKG disturbances and rhythms:
Bradycardia: heart rate < 60 bpm.
Tachycardia: heart rate > 100 bpm.
Atrial fibrillation, atrial flutter, junctional rhythms, PVCs.
Complications: ventricular fibrillation and its implications.
Proarrhythmic Effects
Potential side effects of medications that can cause arrhythmias (proarrhythmias):
Example: Torsades de Pointes (Torsades)
Can arise from QTc prolongation.
Drugs that cause QT prolongation include class 1A antiarrhythmics, certain antibiotics (e.g., Zofran).
Incessant Ventricular Tachycardia (V tach):
Caused by slowed conduction, particularly with class 1A and 1C drugs.
Reentrant tachycardia circuit requires medication or external shock to interrupt.
Heart Block Review
Normal PR interval: seconds.
First-degree heart block: Prolonged PR interval (stable, common in elderly).
Second-degree heart block types:
Mobitz Type I (Wenckebach): progressive PR interval lengthening leading to a dropped beat.
Mobitz Type II: intermittent non-conducted beats often requiring intervention.
Third-degree heart block (complete heart block): independent atrial and ventricular rates (AV dissociation).
Antiarrhythmic Medications Overview
Classification of antiarrhythmics based on ion channel blockade:
Class I: Sodium channel blockers (subdivided into Ia, Ib, Ic).
Ia: Lengthens action potential duration (e.g., quinidine, procainamide).
Ib: Shortens action potential duration (e.g., lidocaine, mexiletine).
Ic: Potent sodium channel inhibitors (e.g., flecainide).
Class II: Beta blockers (e.g., propranolol, esmolol): decrease heart rate and myocardial oxygen demand.
Class III: Potassium channel blockers (e.g., amiodarone): prolong action potential duration.
Class IV: Calcium channel blockers (e.g., diltiazem, verapamil): slow conduction and decrease heart rate.
Specific Antiarrhythmic Drugs
Lidocaine: Used for ventricular arrhythmias (e.g., PVCs, V tach).
Mechanism: Delays phase 4 depolarization.
Dosage: bolus, therapeutic levels .
Advantages: Rapid onset, low side effect profile.
Beta Blockers:
Propranolol: non-selective beta blocker, hepatic metabolism, dosage varies.
Esmolol: selective beta blocker, rapid onset, short duration of action ( mins), careful with concurrent beta blocks.
Effects: Reduces heart rate, myocardial oxygen demand.
Amiodarone: Multifaceted antiarrhythmic, used for various tachyarrhythmias.
Dosage: Initial bolus; possible hypotension.
Side effects: Bradycardia, QT prolongation, pulmonary toxicity, thyroid dysfunction.
Reduces mortality rates post-MI.
Calcium Channel Blockers (e.g., Verapamil, Diltiazem): Best for rate control in rapid atrial arrhythmias.
Dosing of Diltiazem: ; initiate drip thereafter.
Side effects: Bradycardia, hypotension, myocardial depression.
Digitalis (Digoxin): Used to stabilize atrial rhythms, slowing AV conduction.
Recognizable toxicity signs: atrial arrhythmias, visual disturbances.
Adenosine: Treats paroxysmal SVT, rapid infusion required.
Dose: Initial , followed by as needed.
Short half-life (), side effects include transient heart block.