Cardiac Physiology & Pathologies
Cardiac anatomy
Blood Flow through the Heart
heart is a double pump, R side pumps blood into pulmonary circuit, L side pumps blood into the systemic circuit
Right side Left Side
Vena Cava Pulmonary veins
Atrium Atrium
Tricuspid valve Mitral valve
Ventricle Ventricle
Pulmonary valve Aortic valve
Pulmonary artery Aorta
Cardiac Cycle
diastole: chamber at rest & filling with blood
both atria and ventricles can be in diastole at the same time
systole: chamber contracting & ejecting blood
atria and ventricle CANNOT be in systole at the same time
Term Association/ Cycle
mechanical event
contraction generated by calcium influx in cell (DEpolarization)
Cardiac cycle event
systole
Electrical event
depolarization: change in cell membrane electrical charge (- → +) that allows calcium influx
if contraction is in atria it is the P wave
if contraction is in ventricles its QRS complex
Mechanical event
relaxation as calcium is reduced
Cardiac cycle event
diastole
Electrical event
repolarization ( + → -) that allows calcium influx
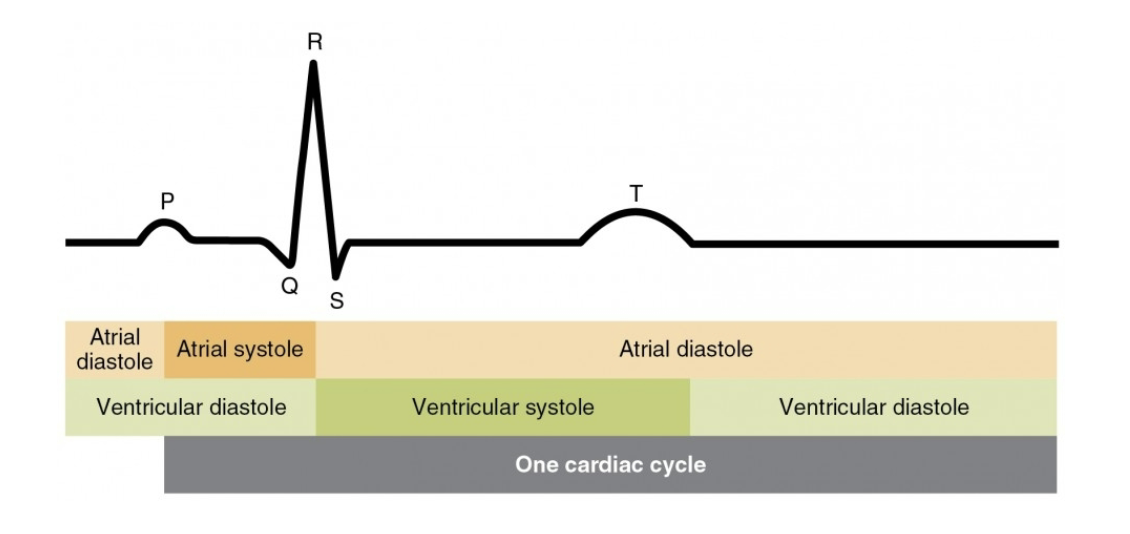
EKG
EKG meaasures electric activity in heart
P wave is electric change in atria initiating contraction (SA node to AV node
T wave represents electric change in ventricles initiating relaxation
QRS represents atrial repolarization and ventricular depolarization (atria relax, ventricles contract)
Atrial & Ventricular Systole
SA node in the R. atrium wraps around the atria and triggers contraction on the way to the AV node
AV node in R. atrium wraps around ventricles & triggers their contraction
Cardiac Pathologies
Cardiac Hypertrophy
concentric hypertrophy: results from pressure overload, MAP is too high
eccentric hypertrophy: too much blood volume getting into ventricle and stretching out tissue
both can be adaptations to exercise, thats when they are good
BOTH can result in heart failure when pathologic, w/ either preserved ejection fraction (HFpEF) or reduced ejection fraction (HFrEF)
Mechanical Event Pathology
there’s a disturbance in the chain
electric normal,
mechanic eccentric hypertrophy from volume overload
causes stretching and weakening of ventricles,
insufficient ventricular pressure
blood flow: reduced ejection fraction (HFrEF)
normal ejection fraction = 70% of LVEDV (left ventricular end diastolic volume (most blood L. ventricle will ever have))
heart failure = <40% of LVEDV
Pressure Event Pathology
electric normal
mechanical normal
pressure: elevated ventricular pressure to overcome arterial pressure (Pventricle>Partery)
chronic hypertension
valvular stress
diabetes, obesity
blood flow is initially maintained (concentric hypertrophy)
over time HFpEF occurs
progression to true heart failure
Blood Flow Event Pathology
electric normal
mechanical normal
pressure normal
blood flow: moves backwards instead of forward due to a valvular disease (regurgitation)
blood flows back into atrium, but theres still blood coming from pulmonary veins that all needs to be pushed back into the ventricle, causing stretching
can lead to overload of the ventricle HFrEF