hemodynamics monitoring brainstorm
these are invasive ways to check a patient’s circulatory status or heart function in critically ill patients.
hemodynamic procedure and tools:
central venous pressure (CVP)
pulmonary artery pressure (PAP)
intra-arterial blood pressure (A-line)
components: invasive catheter, tubing, transducer, amplifier/recorder
Normal hemodynamics values:
CVP: 2-6 mmhg (5-12 cmH2o)
—reflects right atrial pressure and right ventricular preload
—elevated CVP (>6 mmHg or >12 cmH2O) IMPLICATION:
Fluid Overload: too much fluid in the circulatory system
Heart Failure: inability of the heart to effectively pump blood forward
Pulmonary Hypertension: increased resistance in the pulmonary circulation
Tricuspid Valve stenosis/regurgitation: impaired blood flow through the tricuspid valve
Constrictive Pericarditis/Cardiac Tamponade: conditions that restrict the heart’s ability to fill
—decreased CVP (<2 mmHg or <5 cmH2O) IMPLICATIONS:
hypovolemia: insufficient circulating blood volume due to dehydration, hemorrhage, or third spacing of fluids
vasodilation: reduced vascular tone leading to dec venous return
Pulmonary Artery Pressure (PAP)
NV: systolic: 20-30 mmHg, diastolic: 5-10 mmHg, Mean PAP: 10-20 mmHg, reflects pressure in the pulmonary artery
ELEVATED PAP IMPLICATIONS
Pulmonary Hypertension: high blood pressure in the pulmonary arteries
Left Heart Failure: back pressure from the left side of the heart
Pulmonary Embolism: blockage in the pulmonary arteries
COPD: chronic lung disease causing incr pulmonary vascular resistance
DECREASE PAP IMPLICATIONS
Hypovolemia
Pulmonary Vasodilation: decreased resistance in the pulmonary circulation
Pulmonary Capillary Wedge Pressurre (PCWP)
NORMAL: 5-12 mmHg, indicates left atrial pressure and left ventricular preload
ELEVATED PCWP (>12mmHg) IMPLICATIONS
left heart failure: inability of the left ventricle to effectively pump blood forward
mitral valve stenosis/regurgitation: impaired blood flow thru the mitral valve
fluid overload: excessive fluid in the circulatory system
DECREASED PCWP (<5mmHg):
Hypovolemia: insufficient circulating blood flow
Excessive Diuresis: over-removal of fluid from the body
Cardiac Output (CO): 4-6 L/min
—amount of blood ejected by the ventricle per minute, normal CO signifies effective cardiac pumping and tissue perfusion
ELEVATED CO (>8 L/min) IMPLICATIONS
Early Sepsis: inc metabolic demand and compensatory mechanisms
Hyperthyroidism: inc metabolic rate
Anemia: compensatory inc in CO to deliver adequate oxygen
DECREASED CO (<4 L/min) IMPLICATIONS
Heart Failure: reduced pumping ability of the heart
Hypovolemia: insufficient blood volume
Cardiogenic shock: severe reduction in cardiac output due to heart dysfunction
Cardiac Index (CI): NV 2.2-4.0 L/min/m2
—cardiac ourput normalized for body surface area, normal CI reflects adequate cardiac function relative to body size, low CI indicates inadequate cardiac performance
ELEVATED CI (>4.0 L/…) IMPLICATIONS
Early Sepsis: inc metabolic demand
Hyperthyroidism: inc metabolic rate
DECREASED CI (<2.2) IMPLICATIONS
Heart Failure: reduced cardiac function
Cardiogenic Shock: Severe heart dysfunction
Hypovolemic Shock: insufficient blood volume
Mixed Venous Oxygen Saturation (SvO2): NV 60-80%
—reflects balance between oxygen delivery and consumption
ELEVATED SvO2(>80%) COMPLICATIONS
Sepsis: inability of tissue to extract oxygen
Cyanide Poisoning: impaired oxygen utilisation at the cellular level
Hypothermia: reduced metabolic demand
DECREASED SvO2(>60%) COMPLICATIONS
Low Cardiac Output: reduced oxygen delivery
Anemia: insufficient oxygen-carrying capacity
Hypoxemia: inadequate oxygenation of blood
Increased Oxygen Consumption: inc metabolic demand (fever, shivering)
Hemodynamic Monitoring Overview
Purpose: assess cardiac function and circulatory status in critically ill patients
Key tools: CVP, PAP, arterial line
Components include invasive catheters, tubing, transducers, amplifiers, recorders
CVP
measures right atrial pressure; reflecs right ventricular preload
normal range: 2-6 mmHg, water manometer 5-12 cmH2O
inc CVP: RV failure, volume overload, tricuspid valve issues, pumonary hypertension
dec CVP: hypovol
uses: fluid status, pressure assessment, long term IV access
insertion: requires aseptic technique, patient positioning (flat/trendelenburg), monitoring for dysrhythmias
complications: pneumothorax, hemorrhage, infection, dysrhythmias, air embolism
troubleshooting: kinks, clot, improper position and leaks
Pulmonary Artery Catheter (Swan-Ganz Catheter)
measures PAP, PCWP, CO, SvO2
indications: diagnosis, therapy evaluation in heart disease, hemodynamic monitoring
lumen types: proximal (IV, CVP), distal (PA pressure), balloon inflation, thermistor (CO measurements)
insertion sites: subclavian, jugular, brachial femoral veins
nsg care: ECG monitoring during insertion, vigilance for pneumothorax, infection and arrhythmias
common issues: waveform damping, balloon rupture, catheter migration
complications: pulmonary artery perforation, infarction, embolism, infection, arrhythmias, knotting
removal: requires careful sreos including balloon deflation, vital signs, pressure application
Cardiac Output Measurements
Cardiac output = Stroke Volume x heart rate
methods:
fick method (gold standard)
dye dilution
thermodilution (most common)
thermodilution: rapid injection of cold saline, measuring temperature changes; three measurements averaged
cardiac index = cardiac output/body surface area (normal 2.2-4.0 L/min/m2)
body surface area: determined by height and weight nomogram
Mixed Venous Oxygen Saturation (SVO2)
indicates balance between oxygen supply and demand
normal 60-80%
low SVO2: low Hb, hypoxemia, low CO, increased O2 consumption
high SVO2: increased supply or decreased demand
Arterial Line (Intra-arterial BP monitoring)
continuous BP monitoring and blood sampling
indications: complicated surgery, vascular disease, mechanical ventilation, vasoactive drugs, burns, trauma, obesity
insertion sites: radial, femoral, brachial, dorsalis pedis
nsg care: aseptic technique, monitoring, troubleshooting
problems: damped waveform (under or overdamping), hemorrhage, clots, air embolism, infection
prevention: use heparinized solutions, secure connections, change solutioons regularly, sterile dressing changes
Nursing Role & Responsibilities
prepare equipment, explain procedures, obtain consent, maintain asepsis
monitor pts vital signs and ECG during procedures
recognize complications early and troubleshoot technical problems
ensure accurate readings by proper positioning and equipment care
manage catheters, tubing dressings; prevent infection and thrombosis
Prevent Complications!
Central Venous Pressure (CVP) Monitoring
Use strict aseptic technique during catheter insertion to prevent infection.
Ensure proper patient positioning (flat or slight Trendelenburg) for accurate readings.
Monitor carefully for signs of pneumothorax or hemothorax during and after insertion.
Secure all catheters and tubing to prevent disconnections and air embolism.
Regularly change intravenous fluids (IVF) every 24 hours, tubing every 72 hours, and dressings aseptically daily or as needed.
Observe for dysrhythmias caused by catheter irritation.
Relieve kinks and check stopcocks to maintain line patency.
Avoid pushing against clots; withdraw clots carefully if line occlusion occurs.
Pulmonary Artery Catheterization (Swan-Ganz)
Ensure proper balloon inflation and never overinflate beyond recommended limits to avoid pulmonary artery perforation.
Monitor ECG throughout catheter insertion to detect dysrhythmias early.
Maintain strict sterile technique to reduce infection risk.
Watch for pulmonary embolism by avoiding frequent or prolonged balloon wedging.
Document all pressure readings, patient position, and signs of impaired circulation.
Handle the catheter carefully to prevent knotting or catheter migration.
Administer oxygen therapy and medications as prescribed.
Prepare emergency equipment such as lidocaine bolus and defibrillator during catheter removal.
Apply firm pressure with sterile dressing after removal to prevent bleeding.
Arterial Line Monitoring
Use luer-lock connectors and secure catheter with sutures or adhesive to prevent hemorrhage.
Flush continuously with heparinized solution to prevent clot formation.
Purge air bubbles from catheter, IV bags, and drip chamber to prevent air embolism.
Change IV solution every 4 hours and disposable transducer sets every 72 hours to prevent infection.
Perform daily dressing changes and site inspection using strict infection control protocols.
Regularly monitor arterial blood pressure and waveform quality; troubleshoot damped waveforms by flushing tubing and checking for kinks or air bubbles.
General Measures Across Procedures
Explain the procedure to the patient and obtain informed consent.
Monitor vital signs and ECG continuously during insertion and maintenance.
Keep equipment ready for emergency response.
Proper documentation of procedures, readings, and interventions.
Education and training of healthcare providers on proper techniques and troubleshooting.
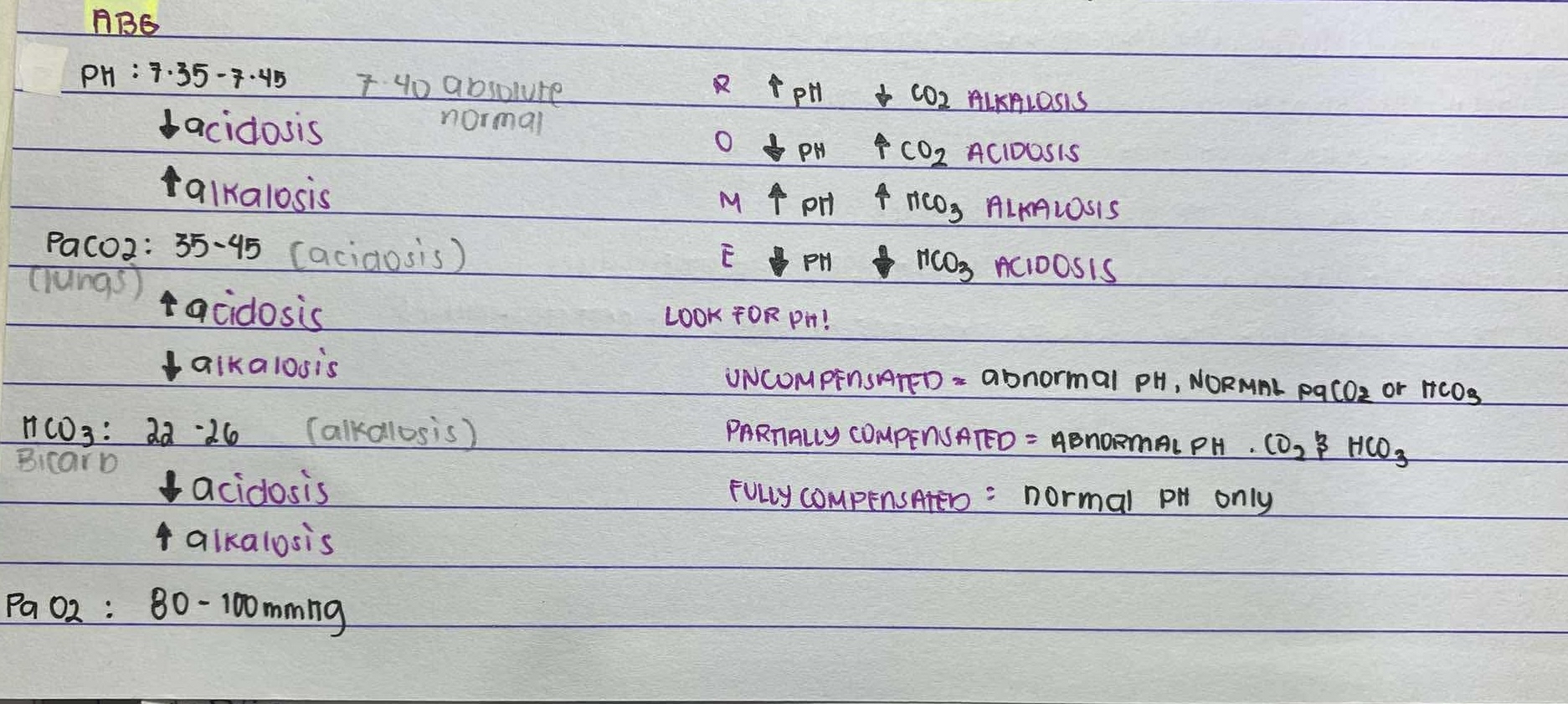
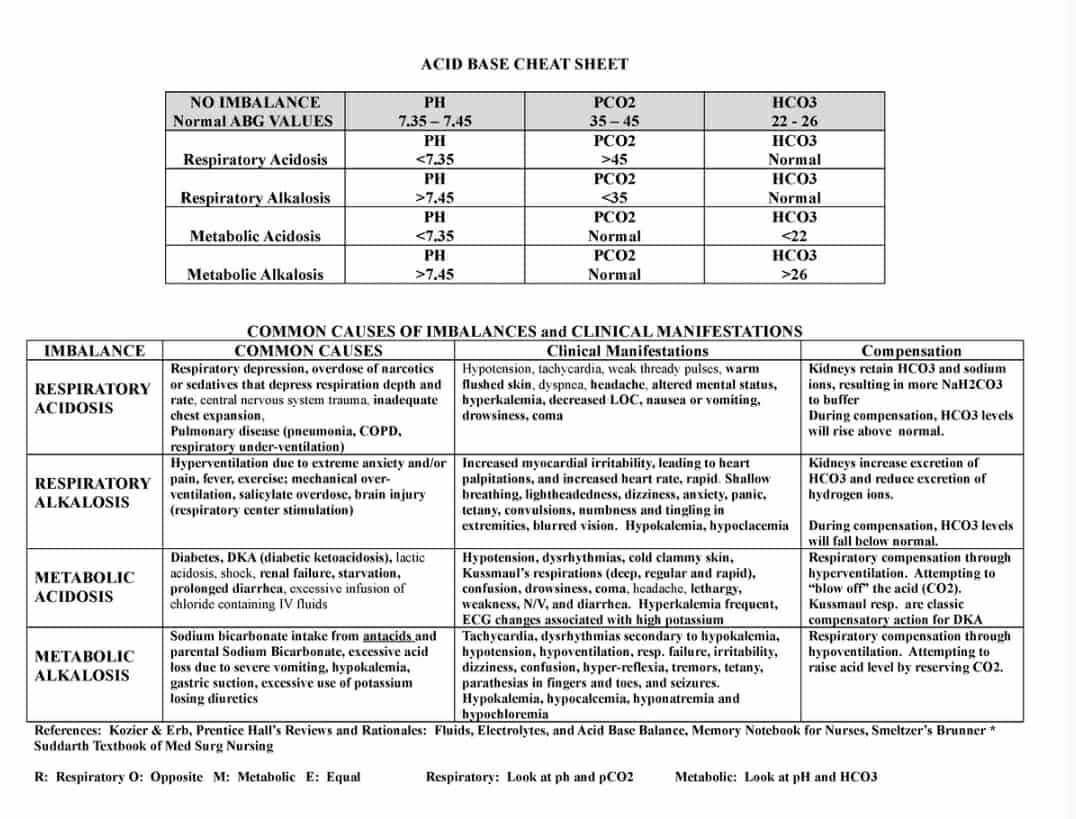
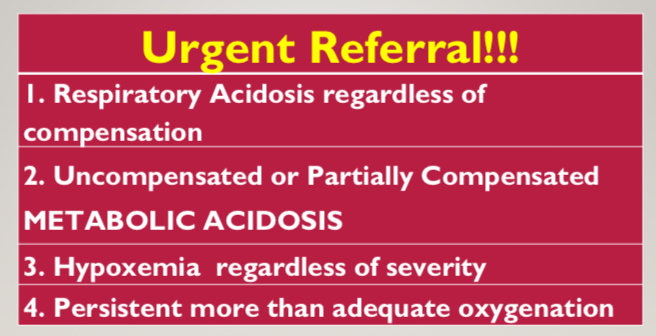
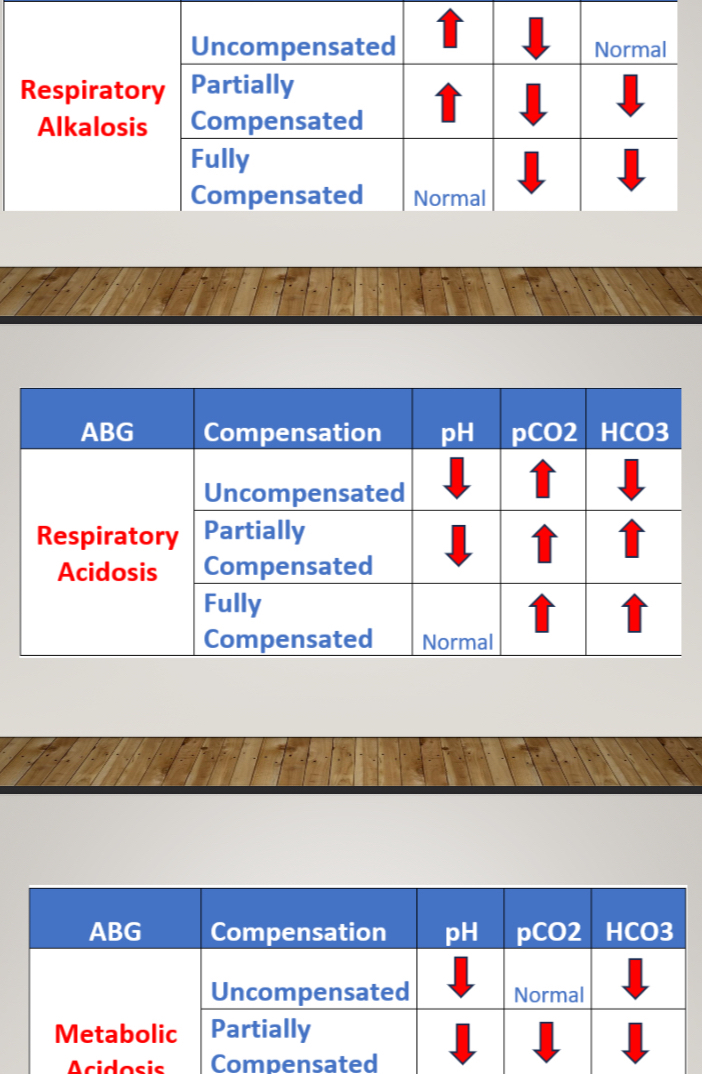
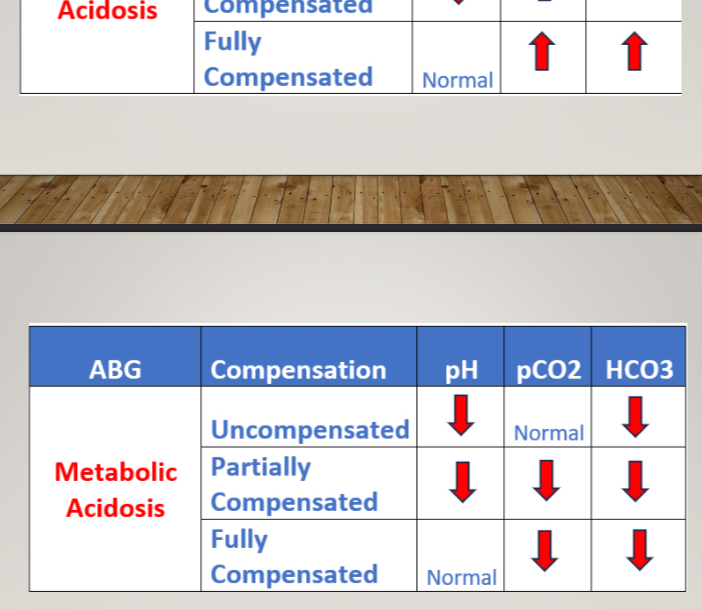
ABGs
pH: 7.35-7.45
PaCO2: 35-45 mmHg
HCO3: 22-26 mmHg
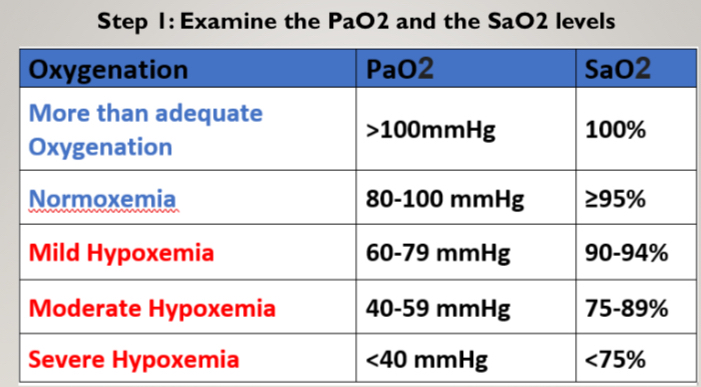
SaO2: 95-100%
PaO2: 80-100 mmHg
PURPOSE
Aids in establishing diagnosis.
Guides treatment plan.
Aids in ventilator management.
Improvement in acid/base management; allows for optimal function of medications.
Acid/base status may alter electrolyte levels critical to a patient’s status.
PROCEDURE of extracting blood specimen for ABG Test
1. Gather needed equipment
Gloves; Skin disinfectant; Gauze; Local anesthetic agent;
Pre-heparinized syringe; Needle G26
2. Palpate the radial artery using 2-3 fingers
Note: Perform Modified Allen’s Test
3. Extend the wrist slightly
4. Clean the site with alcohol swab or disinfectant
5. Infiltrate local anesthesia (not used in hospital settings)
6. Introduce pre-heparinized syringe (45degrees), extract the arterial blood
SaO2 - percentage of hemoglobin saturated with oxygen in arterial blood (O2Sat)
PaO2 - partial pressure of oxygen dissolved in arterial blood
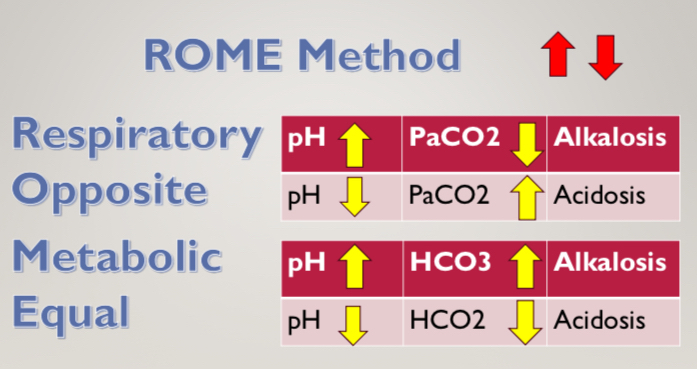
pH - arterial blood acidity or alkalinity
PaCO2 - partial pressure of carbon dioxide dissolved in arterial blood
HCO3 - concentration of bicarbonate ions in arterial blood
POTENTIAL PREANALYTICAL ERRORS
During preparation prior to sampling
Missing or wrong patient/sample identification;
Use of the incorrect type or amount of anticoagulant
>dilution due to use of liquid heparin;
> insufficient amount of heparin;
> binding of electrolytes to heparin;
Inadequate stabilization of the respiratory condition of the patient; and
Inadequate removal of flush solution in arterial lines prior to blood collection.
During sampling/handling
Mixture of venous and arterial blood during puncturing
Air bubbles in the sample.
Insufficient mixing with heparin.
General Storage Recommendation
Do not cool the sample
Analyze within 30 min
During preparation prior to sample transfer
Visually inspect the sample for clots.
Inadequate mixing of sample before analysis