Quiz Report
HA/ MAHAS
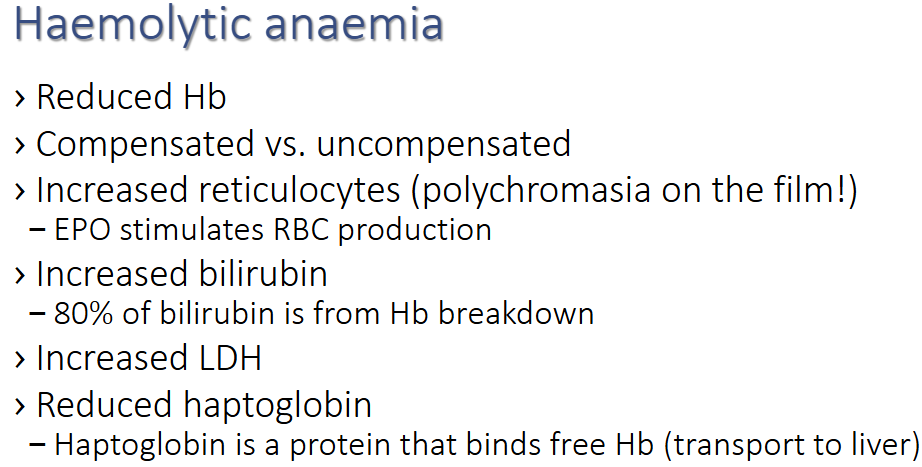
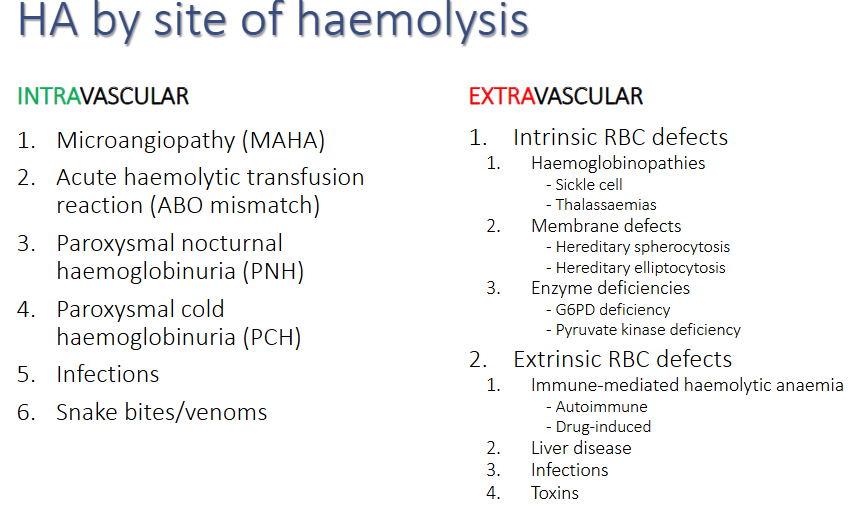
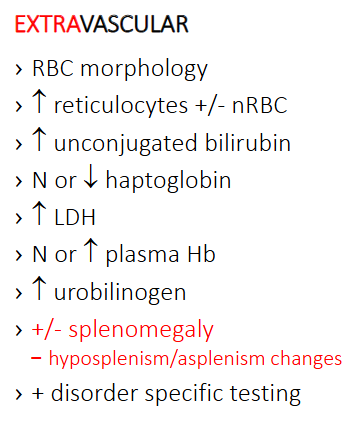
Haemolytic anaemia (EXTRAVASCULAR)
Haemolysis Screen always the same:
**Hereditary Ovalocytosis:
A genetic condition characterized by the presence of oval-shaped red blood cells, leading to mild to moderate hemolytic anemia.
Caused by genetic mutations affecting the membrane proteins of the red blood cells, which makes the cells more rigid.
Cells look like bread loaves or nutri grain (ovale stomacytes).
Requires further genetic testing.
Hereditary Elliptocytosis (HE)
What are some symptoms of Hereditary Elliptocytosis?
Fatigue or weakness due to anemia
Jaundice from increased bilirubin levels
Splenomegaly (enlarged spleen)
Increased susceptibility to infections
Gallstones due to hemolysis can occur as a result of increased bilirubin production.
What would you see on the FBC and blood film?
In a full blood count (FBC), one would typically observe normocytic anemia, with a possible decrease in hemoglobin and hematocrit levels. The blood film may reveal the presence of elliptical-shaped erythrocytes, known as elliptocytes, along with the potential presence of reticulocytes indicating increased erythropoiesis in response to hemolysis. Additionally, the FBC may show a compensated reticulocytosis as the body attempts to produce more red blood cells to counteract the anemia, while the blood film might also indicate the presence of other abnormal cell shapes.
Explain the pathophysiology of Hereditary Elliptocytosis and how does this affect the cells? Hereditary Elliptocytosis is characterized by a defect in the spectrin or protein 4.1, which leads to a distortion in the red blood cell membrane, causing the typical elliptical shaped red blood cells. This altered shape affects the cell's flexibility, making it more susceptible to splenic sequestration and destruction, ultimately resulting in anemia and increased jaundice due to elevated bilirubin levels.
What is the differential diagnosis?
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
**Autoimmune Haemolytic Anaemia (AIHA)
What are some symptoms of AIHA?
SOB
Lower back pain
What would you see on the FBC and blood film?
Low RCC
High MCV
nRBC (from compensation due to crisis)
Marked spherocytes
Polychromasia (retics)
Explain the pathophysiology of AIHA and how does this affect the cells?
Extravascular & Extrinsic haemolysis: Due to the production of antibodies against red blood cells, often triggered by autoimmune disorders, infections, or certain medications, leading to premature destruction of RBCs in the spleen and liver.
What is the differential diagnosis?
Hereditary spherocytosis
Other autoimmune disease
Drugs
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
Haemolysis screen:
DAT:
(Note: if DAT neg, its HS)
**Cold Auto Immune Haemolytic Anaemia
What are some symptoms of cold auto immune haemolytic anaemia?
Dizziness
Lower back and leg pain
Fatigue
Cold sensation in fingers and toes
What would you see on the FBC and blood film?
On the full blood count (FBC), you would typically observe a low HB, low HCT, low RCC
The blood film may show signs of hemolysis, such as spherocytes or polychromasia.
Explain the pathophysiology of cold auto immune haemolytic anaemia and how does this affect the cells?
The pathophysiology involves the binding of IgM antibodies to red blood cells at colder temperatures, leading to agglutination and eventual destruction in the liver and spleen.
This immune response disrupts normal cellular function and lifespan of red blood cells, resulting in anemia.
What is the differential diagnosis?
Differential diagnosis includes warm autoimmune hemolytic anemia,
hereditary spherocytosis
IM (mono)
drug-induced hemolysis.
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
Haemolysis screen
C3D:
Viral screen:
Mycoplasma screen:
(Note: Can be caused by IM)
Hereditary Sperocytosis (HS)
What are some symptoms of Hereditary spherocytosis.
Anemia: Due to the destruction of spherocytes by the spleen, patients often present with fatigue and pallor.
Jaundice: A result of elevated bilirubin levels from increased hemolysis, leading to yellowing of the skin and eyes.
Splenomegaly: Enlargement of the spleen due to its increased workload in filtering abnormal red blood cells.
Gallstones: Higher risk of developing pigment gallstones due to increased bilirubin levels.
Lower back pain
What would you see on the FBC and blood film?
Increased WBC count indicative of splenic activity
Decreased RBC count reflecting anemia and
Elevated RETIC count demonstrating the bone marrow's compensatory response.
Marked spherocytes
Explain the pathophysiology of Hereditary spherocytosis and how does this affect the cells?
A genetic disorder cthat produces abnormal red blood cells in a spherical shape, which leads to increased fragility and hemolysis. Results from defects in the proteins that make up the red blood cell membrane, such as spectrin or ankyrin, disrupting the cell's cytoskeleton and leading to a loss of the typical biconcave shape. Altered red blood cells are more prone to rupture, especially as they pass through the spleen, causing anemia and compensatory reticulocytosis due to the bone marrow's attempt to produce more red blood cells. Spherocytes also exhibit a reduced surface area-to-volume ratio, which compromises delivery of oxygen efficiently to tissues and causes sequestration and destruction by the spleen. Accumulation of spherocytes in the bloodstream contributes to splenomegaly, as the spleen becomes enlarged due to the increased workload of filtering spherocytes.
What is the differential diagnosis?
Auto immune haemolytic anaemia
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
Supravital stain to see RETICS
Haemolysis screen
DAT:
E5M
**Oxidative Haemolytic anaemia (drug induced)
What are some symptoms of Oxidative haemolytic anaemia?
Drug use is key
Haematuria
Back pain
What would you see on the FBC and blood film?
Bite Cells = oxidative
Mild polychromasia
Sometimes spherocytes
Anaemia
High MCV (macrocytic)
Explain the pathophysiology of oxidative haemolytic anaemia and how does this affect the cells?
Intravascular and extravascular haemolysis
Oxidative stress leads to damage of red blood cells (RBCs), resulting in the formation of bite cells due to the removal of denatured hemoglobin (heinz bodies) by splenic macrophages.
This disrupts the integrity of the cell membrane causing mild polychromasia as bone marrow compensates by producing more retics. Possible spherocytes indicates increased destruction of RBCs, as they are less flexible and more likely to be engulfed by macrophages during circulation.
What is the differential diagnosis?
G6PD
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
Haemolysis screen
Heins body test: Dye that shows oxidative damage
**Oxidative Haemolytic anaemia- G6PD deficiency (X-linked, in males)
Genetic deficiency. is X-linked, making males higher risk
What are some symptoms of G6PD stress?
Symptoms during crisis include jaundice, dark urine, and fatigue.
Common triggers for hemolysis include infections, certain medications (e.g., sulfa drugs), and foods like fava beans.
What would you see on the FBC and blood film?
Blisters + bite cells = oxidative
Explain the pathophysiology of G6PD stress and how does this affect the cells?
Decreased production of NADPH from the pentose phosphate pathway limits the reducing agents maintaining glutathione in its reduced form, exacerbating oxidative damage and promoting hemolysis. Oxidative stress leads to a decreased ability of red blood cells to regenerate reduced glutathione, which normally protects them from damage; this results in hemoglobin denaturation and the formation of Heinz bodies, ultimately leading to cell rupture and hemolysis. This compromises the structural integrity of the red blood cells, making them more susceptible to destruction in the spleen.
What is the differential diagnosis?
Drug induced haemolytic anaemia
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
Haemolysis screen
Heins body test: Dye that shows oxidative damage supravital stain
G6PD screening test: Cannot test for G6PD during crisis
NOTE: PDX always Ox haem anaemia. DDX drug induced or G6PD.
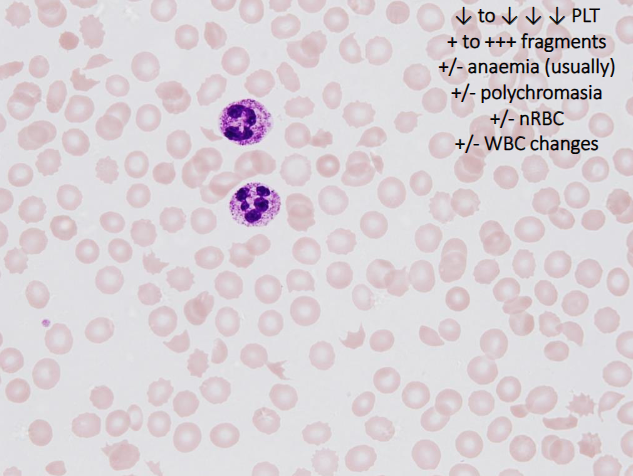
Micro angiopathic haemolytic anaemia (Schistocytes)
Similarities: Serious and can be rapidly fatal – ALWAYS URGENT – must phone doctor.
Characterised by
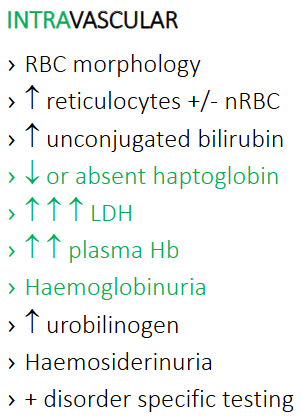
INTRAVASCULAR HAEMOLYSIS
RBC fragments (schistocytes)
Microthrombi and/or damaged endothelium
Thrombocytopenia
Usually moderate to marked/critical levels
Haemolysis is intravascular (but both occur)
Intravascular – RBC damage/shearing
Extravascular – spleen clears fragments

Haemolysis Screen always the same:
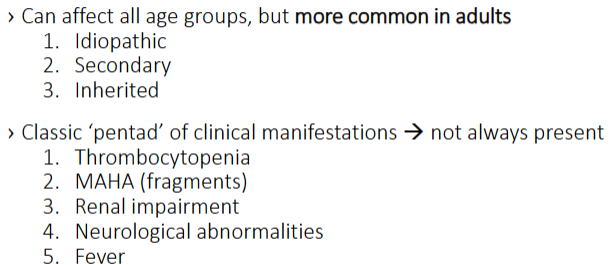
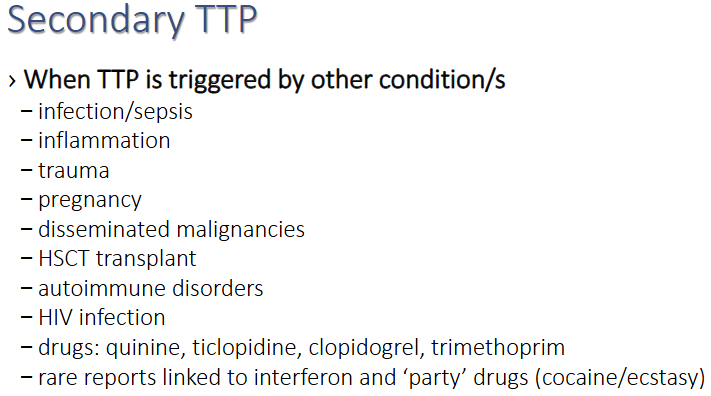
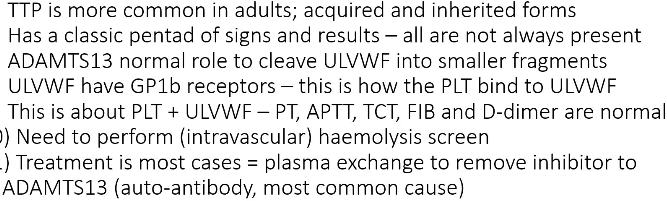
TTP Thrombotic Thrombocytopenic Purpura (IN ADULTS)
Adult-driven; deficiency of enzyme. Normal coags usually, but critical thrombocytopenia.
Symptoms
What would you see on the FBC and blood film?
Morphology: Schistocytes, nucleated reds, and extreme lack of platelets.
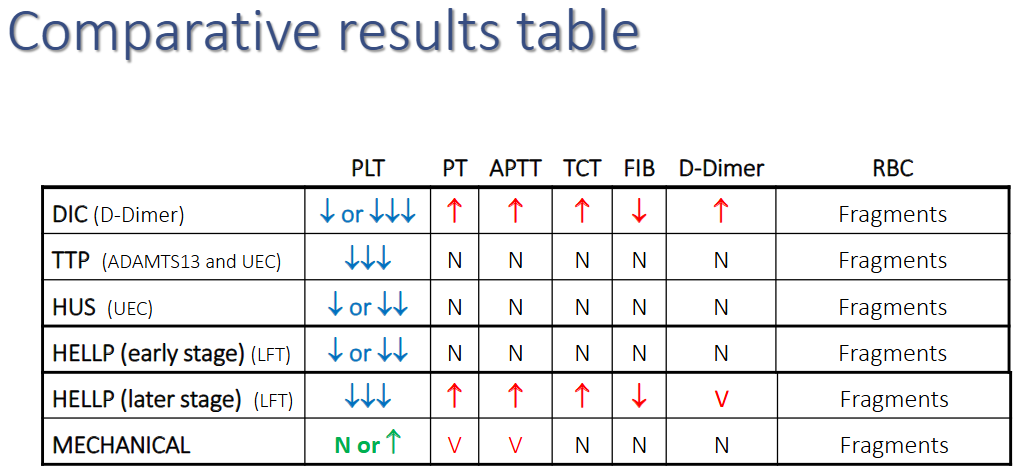
Coagulation: Coags are typically normal in TTP, which is a key diagnostic differentiator from DIC.
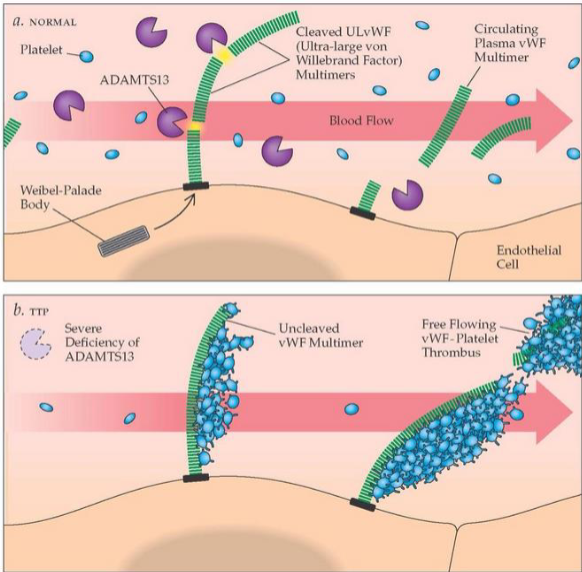
Explain the pathophysiology of Thrombotic Thrombocytopenic Purpura and how does this affect the cells?
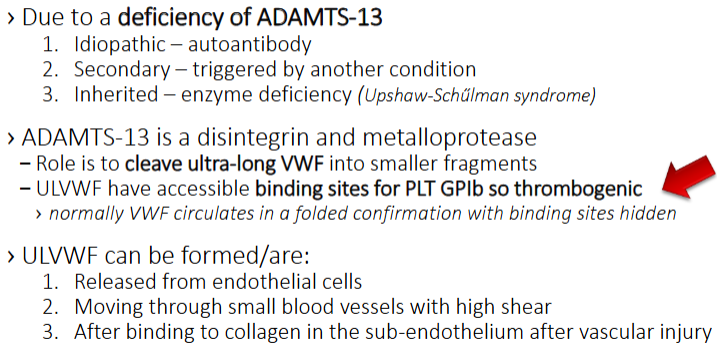
Deficiency or inhibition of the enzyme. This prevents the cleavage of ultra-long Von Willebrand factor () molecules, which then catch and consume platelets into microthrombi, especially in the brain/neurological system.
What is the differential diagnosis?
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
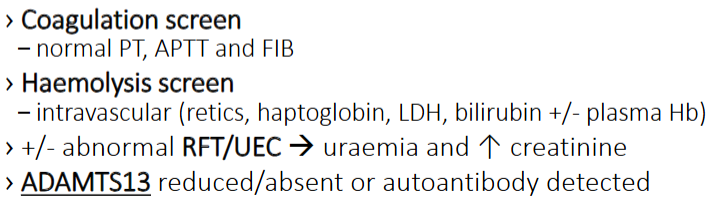
Coagulation screen
PT:
APTT:
FIB:
Haemolysis screen
RFT/UEC:
ADAMTS13 screen:
Important points:
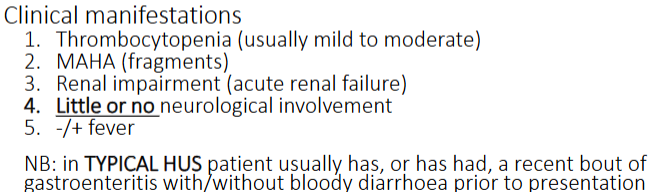
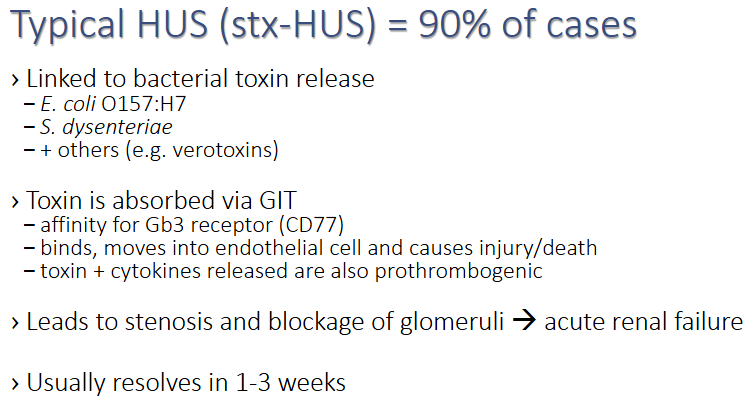
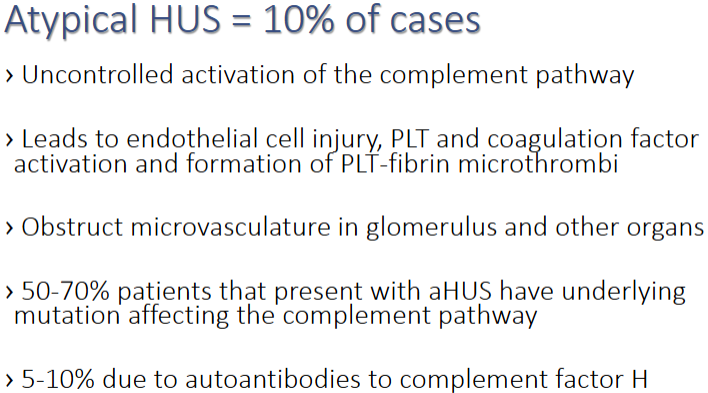
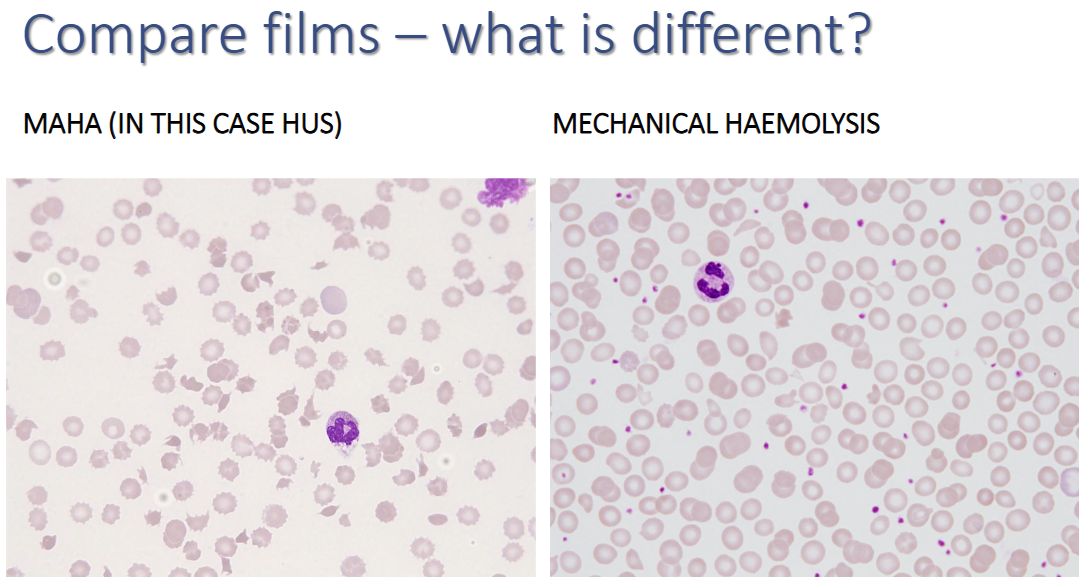
**HUS Hemolytic Uremic Syndrome (IN CHILDREN)
Pediatric-driven; triggered by toxins ( ). Normal coags, renal failure symptoms.
What are some symptoms of Hemolytic Uremic Syndrome?
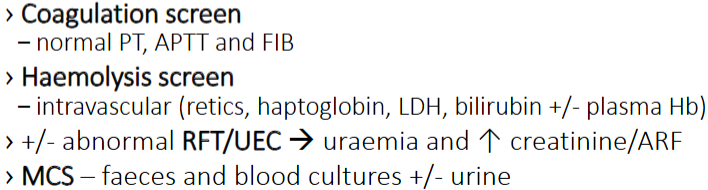
Coagulation: In HUS, coags () are typically normal, as the primary pathology is localized endothelial damage in the kidneys rather than systemic factor consumption.
What would you see on the FBC and blood film?
Morphology: Schistocytes (fragments), Polychromasia (regeneration), Nucleated Red Blood Cells (), and pseudospherocytes (damaged/remodeled cells).
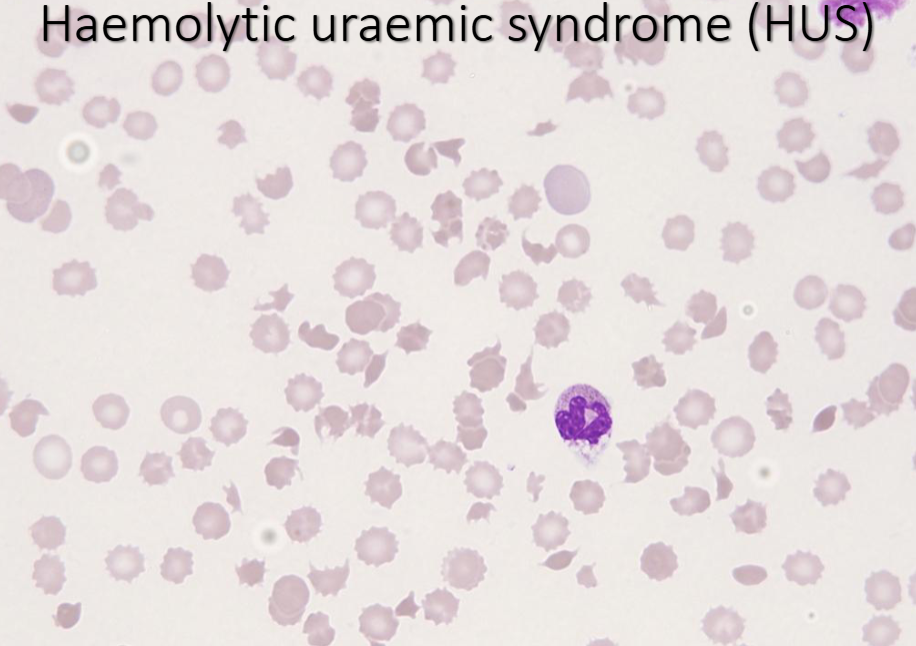
Explain the pathophysiology of Hemolytic Uremic Syndrome and how does this affect the cells?
In Hemolytic Uremic Syndrome (HUS), the endothelial damage leads to microangiopathic hemolytic anemia due to the stress placed on red blood cells as they pass through narrowed or damaged microvasculature. This results in the formation of schistocytes as the cells are fragmented. Due to the increased demand for red blood cell production in response to hemolysis, polychromasia and nucleated red blood cells may be observed in the blood film, indicating regeneration. Presence of pseudospherocytes suggests the red blood cells are undergoing significant remodeling due to membrane damage, which can further affect functionality and lifespan. This can contribute to the overall hemolytic process, exacerbating anemia and leading to complications related to insufficient red blood cell counts.
What is the differential diagnosis?
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
Coagulation screen
PT:
APTT:
FIB:
Haemolysis screen
RFT/UEC
Urine and faeces MCS:
Blood culture:
Important points:
HELLP Hemolysis, Elevated Liver enzymes, Low Platelets (ONLY IN PREGNANT WOMEN)
Early stage normal coags, Late stage elevated coags
What are some symptoms of HELLP?

What would you see on the FBC and blood film?
Explain the pathophysiology of HELLP and how does this affect the cells?
HELLP syndrome is characterized by hemolysis, elevated liver enzymes, and low platelet count, which stems from the severe activation of the coagulation cascade and endothelial dysfunction.
What is the differential diagnosis?
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
Coagulation screen
PT:
APTT:
FIB:
LFT:
Important points:
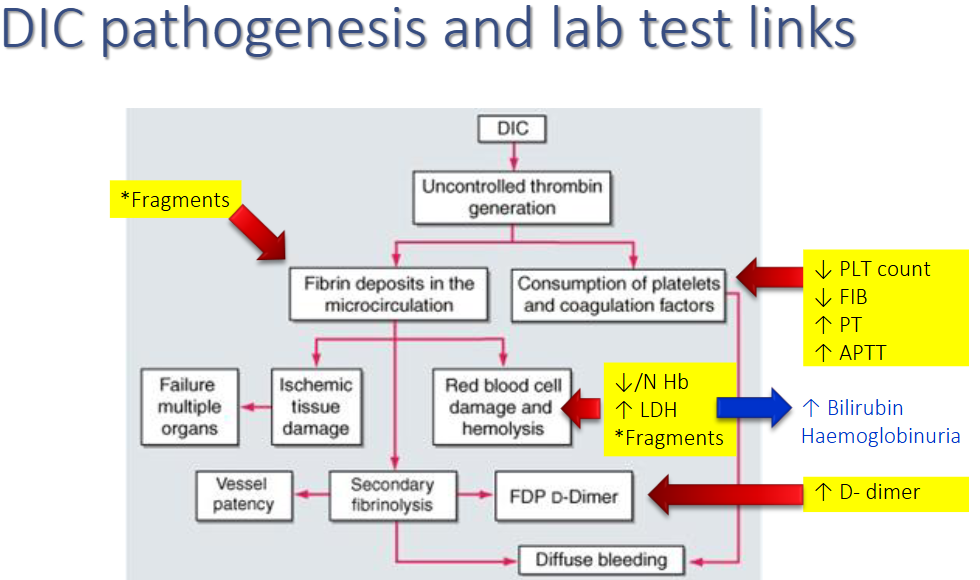
**DIC Disseminated Intravascular Coagulation (AFFECTS ALL)
Sepsis/malignancy trigger; elevates coags and platelets
Symptoms
Patients may present with bleeding, organ dysfunction, and signs of ischemia, leading to critical complications such as acute kidney injury or respiratory failure.
What would you see on the FBC and blood film?
Haemolysis, such as schistocytes, as well as thrombocytopenia
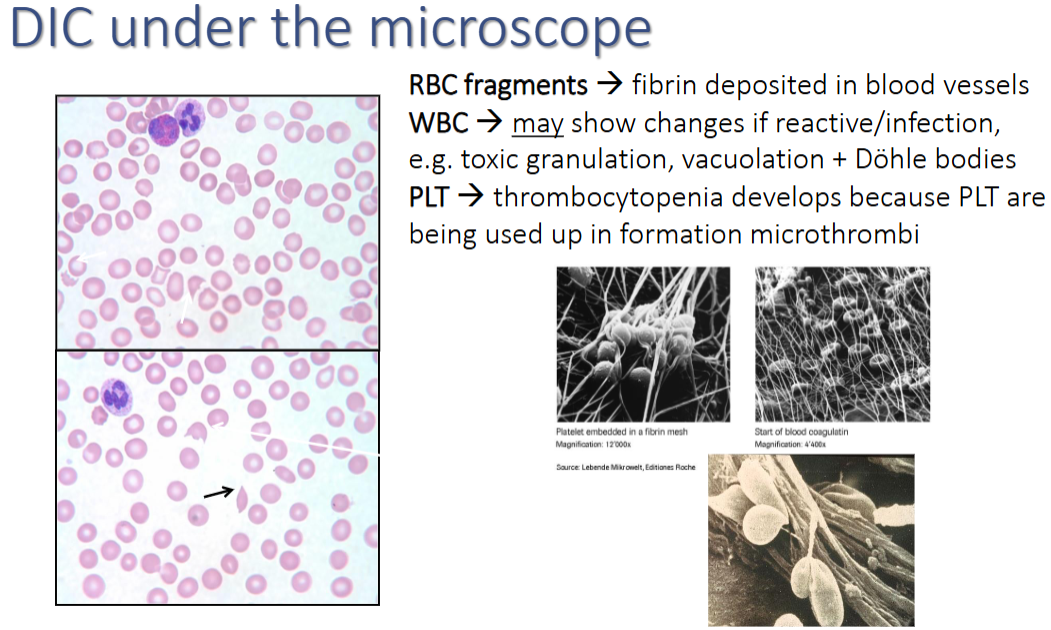
Explain the pathophysiology of DIC and how does this affect the cells?
In DIC, widespread activation of the coagulation cascade leads to the formation of microthrombi throughout the small blood vessels, which results in multi-organ dysfunction due to impaired blood flow. This process causes the consumption of clotting factors and platelets, leading to a paradoxical increased risk of bleeding despite elevated coagulation parameters. Elevated levels of D-dimer, reflecting the breakdown of fibrin, and the blood film may show a reduced number of red blood cells due to hemolysis.
What is the differential diagnosis?
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?

Coagulation screen
PT:
Purpose: To assess the extrinsic and common pathways of coagulation.
Expected Result: Prolonged PT indicates possible deficiencies in clotting factors such as VII, X, V, prothrombin, or fibrinogen.
APTT:
FIB:
D-Dimer:
Haemolysis screen
What is the differential diagnosis?
Important points:
MECHANICAL HAEMOLYSIS
HIGHER PLTS (Often heart valve related)
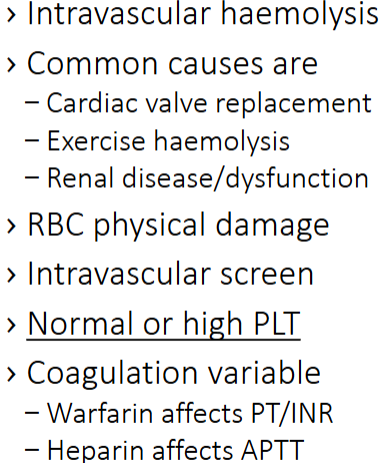
What would you see on the FBC and blood film?
Schistocytes as evidence of fragmented red blood cells indicating mechanical damage.
Normal or high platelets can be observed, reflecting the compensatory response to ongoing damage and hemolysis.
Reticulocytes may also be elevated as the bone marrow responds to the increased demand for red blood cell production due to hemolysis.
Will likely have raised PT/INR as patients are on warfarin Rx
If they are an inpatient the APTT would be elevated if they are on heparin Rx
Explain the pathophysiology of mechanical haemolysis and how does this affect the cells? Mechanical hemolysis occurs when red blood cells are physically damaged due to turbulence in blood flow or contact with artificial surfaces, such as prosthetic heart valves. This causes fragmentation of red blood cells resulting in the release of hemoglobin into circulation and depletion of red cell mass. In response to this loss, the bone marrow attempts to compensate by increasing red blood cell production, leading to the presence of reticulocytes in the blood. Damaged red blood cells may release cytoplasmic contents, contributing to further inflammatory responses and potential organ dysfunction. This can stimulate the production of additional cytokines and promote further activation of the immune system.
What is the differential diagnosis?
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?
Haemostasis and Coagulation
PAEDS
ABO Haemolytic disease of the Newborn (HDN)
What are some symptoms of ABO Haemolytic disease of the Newborn?
What would you see on the FBC and blood film?
Explain the pathophysiology of ABO Haemolytic disease of the Newborn and how does this affect the cells?
What is the differential diagnosis?
What are the tests that can be requested? Why are you requesting them and what are the expected results for each test mention?