POHS II: Final Exam
Objectives:
Pedo/Ado → 5
Effective Communication → 9
Home Care → 6
Dentifrice/Mouth-rinse → 6
Fixed/Removable Appliances → 5
Instrument Sharpening → 6
Advanced Periodontal Instrumentation → 4
Power Scaling → 5
Air-polishing → 6
Professionalism → 8
Instrument Sharpening
Dull Vs Sharp Periodontal Instruments
Dull | Sharp | |
Stroke Control |
|
|
Number of Strokes |
|
|
Calculus Removal |
|
|
Fatigue |
|
|
Patient Comfort |
|
|
Reflection of Light |
|
|
Bites into Test Stick |
|
|
List visual and tactile ways to test instruments for sharpness/dullness:
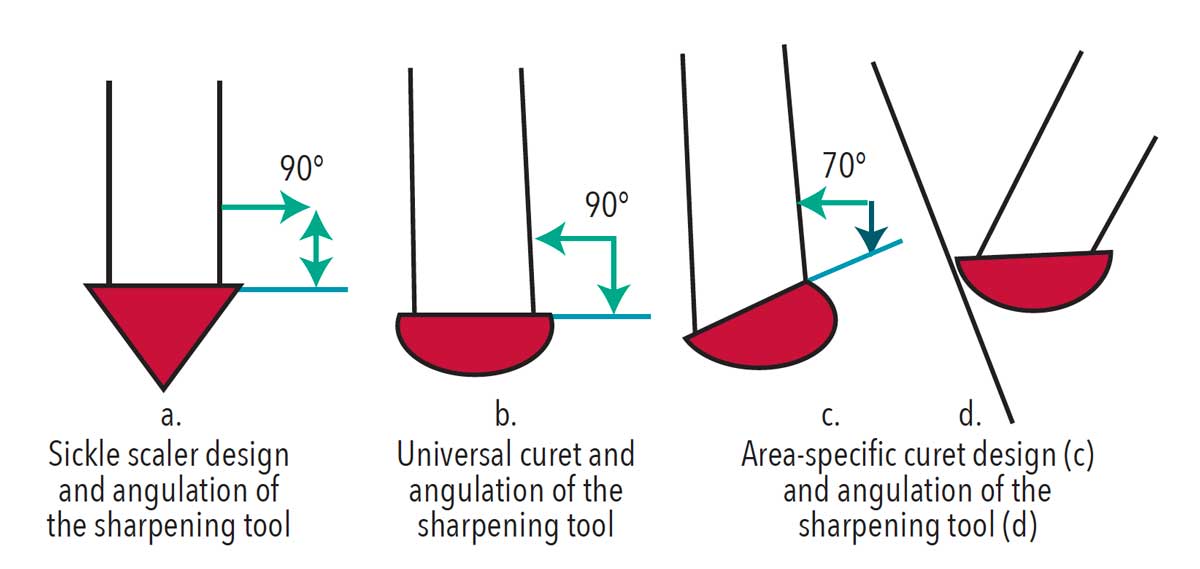
Position the terminal shank:
Area-specific: slightly tilted away
Universal/scaler: perpendicular to the floor
Motion:
up-and-down motion (end on a downward stroke)
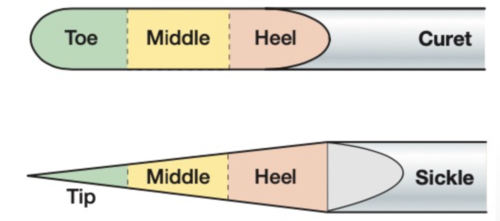
Focus on the heel, middle, and toe (tip third)
Pressure:
light to moderate
Listen for a “squeak”
3–5 strokes

Check Your Work
Test all thirds for a “bite”
List characteristics of each:
Ceramic: Fine grit; maintains cutting edge

Arkansas Stone: Moderately coarse; oil recommended; restores partially dull blades

Carborundum Stone: irregular particles that restore dull blades

Diamond-Coated (Card/Steel): Most aggressive; for completely dull instruments
automated sharpeners
Advanced Periodontal Instrumentation
Extended Gracey Curets:
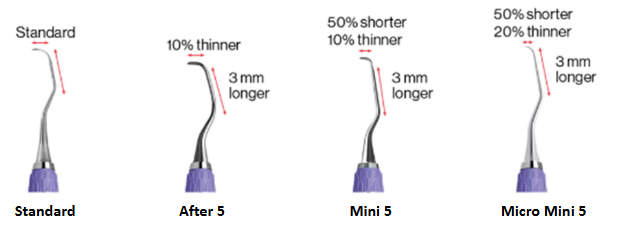
After Five:
Terminal shank 3 mm longer
Blade 10% thinner
Designed for pockets ≥ 5 mm

Mini Five Curettes
Terminal shank 3 mm longer
Blade 10% thinner
Blade length 50% shorter
Best for:
Deep pockets (≥ 5 mm)
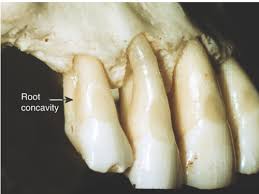
Concavities
Longitudinal depressions
Furcations
Micro Mini 5
50% shorter
20% thinner
3mm longer and thicker
APPLICATION SAME AS STANDARD GRACEY

Advanced Instrumentation:
Instrument | Primary Uses | Key Design Features | Stroke Style |
|---|---|---|---|
Chisel Scaler  |
 |
|
 |
Hoe  |
|
| Vertical pull stroke ONLY  |
Debridement Curette  |
|
|
 |
Periodontal Files  |
|
| Moderate lateral pressure; pull stroke only  |
Finishing files  |
|
|
|
Vision Curvette  |
|
| same as Standard Gracey |
Laser Therapy  |
|
|
|
Power Scaling
Power Vs. Traditional Instruments
Powered Instruments | Traditional Instruments |
0.3-0.55mm tip | 0.76-1.0mm tip/toe |
Trauma ↓ | Trauma ↑ |
Remove from above | Remove from below |
Pocket distention ↓ | Pocket distention ↑ |
Aerosols ↑ | Splatter ↓ |
Faster | Slower |
Contraindications ↑ | Contraindications ↓ |
Terms to Know:
Dysphagia
difficulty swallowing

acoustic turbulence
agitation in the fluid surrounding the vibrating tip
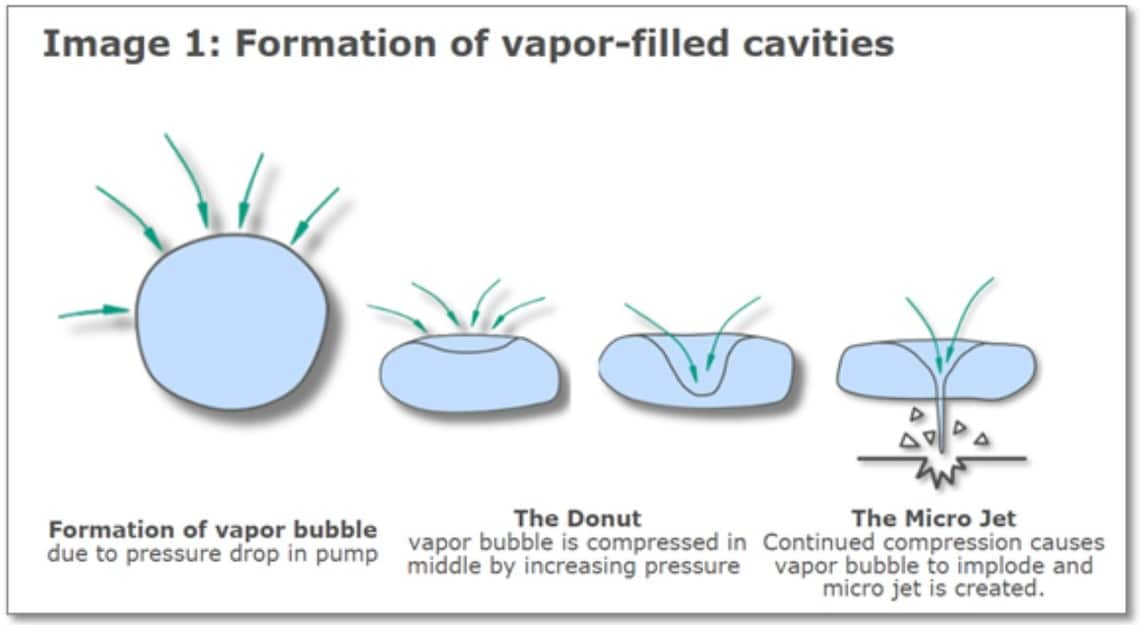
cavitation
creation and collapse of vapor-filled bubbles due to pressure variations
oscillation
going back and forth between two positions

lavage
washing of the pocket surface to remove endotoxins and loose debris

transducer
device that converts energy from one form to another
sonic scaler
Driven by compressed air with a handpiece attached to the dental unit tubing

ultrasonic scaler
converts high-frequency electrical currents to mechanical vibrations

magnetostrictive
generates a magnetic field and produces tip vibration by stack or rods
stack
acts as an antenna to pick up the magnetic field and cause vibrations

rod
ferromagnetic material with high magnetic permeability

piezoelectric
activated by a change in the crystals in the handpiece

Sonic vs. Magnetostrictive vs Pizeoelectric
Sonics | Magnetostrictive | Pizeoelectric | |
Frequency | 3,000-8,000 CPS | 18,000-45,000 CPS | 25,000-50,000 CPS |
Transductor | Compressed Air | Stacks or Rod | Ceramic Rod |
Stroke Pattern | Elliptical | Elliptical | Linear |
Active Area of Insert Tip | All surfaces | All surfaces | Lateral surfaces |
Oral Contraindication:
Demineralized enamel
Exposed dentin
Restorations
Titanium implants
Primary teeth (large pulp chambers → increased sensitivity)

Systemic Contraindications:
Communicable diseases: TB, COVID-19
Immunocompromised patients: uncontrolled diabetes
Respiratory conditions: COPD, Asthma, Emphysema, Cystic fibrosis
Dysphagia/gag reflex conditions: ALS, Parkinson’s, MS, stroke, and Pacemaker

Clinician/Patient PPE:
Clinician:
level 3 mask
face shield
Patient:
preprocedural rinse → 0.12% chlorhexidine
Apply Vaseline to the lips
Risk to Clinicians And/or Patients:
hearing changes
Vibration-related nerve sensitivity
Overheating tip → thermal damage to pulp/gingiva
Children are more sensitive to vibration
Waterline contamination risk
Insert Types
Summary:
Condition / Deposit | Recommended Insert Tip(s) |
|---|---|
Biofilm  | Perio Thinsert and contra-angled |
Heavy supra and sub Calculus / Heavy Stain  | Universal, Triple Bend & Beavertail |
Light/Moderate Calculus  | Perio Thinset, Universal (supra) or contra angle (sub) |
Furications and concavities  | contra-angled and Furcation |
Implants / Veneers  | Implant |
Developmental concavities  | contra-angle and furcation |
Air Polishing
Purpose & Key Features:
Efficient removal of stains and biofilm
Delivers slurry: air + water + powder
Propels abrasive particles to tooth surface
Pressures:
Air pressure: 40–100 PSI
Water pressure: 20–60 PSI
Advantages:
NO heat generation
ergonomic
Powders are less abrasive than polishing paste
Uses:
Preferred for orthodontic appliances
Acceptable before sealant placement

Powders
Sodium Bicarbonate (SB)
Original powder: salty taste and may sting
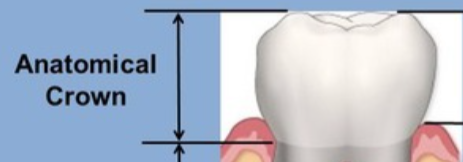
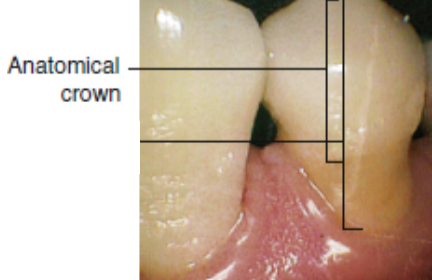
Use: anatomical crown only
Compatible: amalgam, gold, porcelain; NOT for some restorations or root surfaces
Mohs hardness: 3.0 size: 74 µm
Aluminum Trihydroxide
Alternative to SB
Use: anatomical crown only; not for restorations
Mohs: 4.0 size: 80 µm

Calcium Carbonate
Main ingredient in antacid
Use: anatomical crown only; effect on restorations unknown
Mohs: 3.0 size: 45 µm
Calcium Phosphosilicate
Bioactive glass — researchers warn against use (destructive to enamel/root)
Mohs: 6.0 size: 120 µm

Glycine
Amino acid powder
Reduces abrasiveness to the root by ~80%
Use: supra- and subgingival; safe on all restorations
Also detoxifies the root surface
Mohs: 2.0 size: 20 µm

Erythritol
Water-soluble polyol (sweetener)
Use: supra- and subgingival; safe on all restorations
Detoxifies the root surface
Mohs: <2.0 size: 14 µm

Oral Contraindications:
ALL:
open wounds
≤3 mm supporting alveolar bone → risk of subcutaneous emphysema
Caused by angulation into sulcus
Symptoms: swelling, tenderness, crackling sensation, and extreme pain
Management: emergency treatment, observation, antibiotics, and analgesia

Prophy-jet Polishing:
Root surfaces, Soft, spongy, or inflamed gingiva

Systemic Contraindications:
ALL:
Communicable airborne diseases: cold, flu, and COVID.
Respiratory disease or breathing disorders: asthma, COPD, cystic fibrosis, and pulmonary hypertension
Very immunocompromised patients: AIDS, cancer treatment, uncontrolled diabetes, immunosuppressive meds, hemophilia, neutropenia, agranulocytosis

Prophy-Jet ONLY:
End-stage renal disease, Addison’s disease, Cushing’s disease, metabolic alkalosis
Patients on potassium, antidiuretics, or steroid therapy
Sodium Bicarbonate ONLY:
sodium-restricted diet, high blood pressure, kidney disease, heart problems
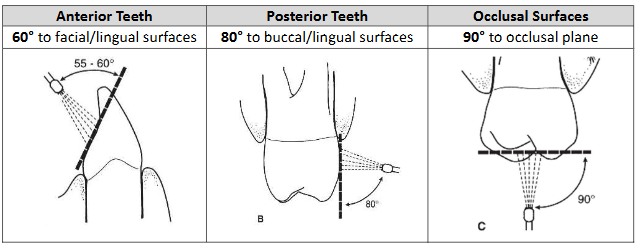
Supragingival Use with Prophy-Jet
Preparations:
cup lips or cheek to control aerosols
Procedure:
Nozzle 4–5 mm from the tooth
Anterior teeth: 60° to the facial/surfaces
Posterior teeth: 80° to buccal surfaces
Occlusal surfaces: 90° to occlusal surfaces
Method:
constant circular motion
1-2 seconds per tooth
rise and floss
Supragingival with Airflow
Procedure:
Nozzle 2–5 mm from tooth
heavier → closer
far → aerosol
Angulation: use between 15°–80° (avoid 90°)
method:
constant circular motion
1-2 seconds per tooth
rinse and floss

Subgingival with Air-Flow
Procedure:
Insert inactive tip until contact with JE, withdraw 1 mm coronally (away from base)
Activate for 5 seconds with overlapping vertical strokes
Note:
FDA: approved for pockets ≤5 mm (Canada: ≤10 mm)
tip directs to root surface, NOT base of pocket

Professionalism:
Function of Mid-level Providers:
Purpose:
bridge the gap to care
expand functions:
caries removal
place composites and amalgam
place space maintainers
Fabricate a stainless steel and a temporary crown
pulpotomies and pulp vitality testing
Extract erupted primary teeth

Core values
autonomy
respect for persons ability to make a choice

confidentiality
protect privileged communication
societal trust
bond between DH, patients, professionals, and the public

non-maleficience
avoidance of harm to others

beneficence
act of doing good

justice/fairness
fair treatment

veracity
tell the truth when information is disclosed to patients

Process of Care:
assess:
collect subjective/objective data

diagnose:
critical thinking to interpret data

plan:
strategies that meet patient needs
implement:
activation of care plan

evaluation:
determines patient needs to be retreated, referred, or placed on a continuing care schedule

documentation:
details of assessment data, diagnosis, care plan, treatments, patient education, and evaluation

Services
primary prevention: → reverse progression of disease BEFORE it begins
oral evaluation
prophylaxis
sealants
fluoride as a preventative agent
health education/promotion

secondary treatment → treat early disease
restoration
endodontics
fluoride and sealants on incipient caries

tertiary treatment: → replace lost structure
prosthodontics
implant
oromaxillofacial surgery

educational: → promotes change in individuals
link oral to systemic health
creates partnership
therapeutic: → arrest and control disease AFTER it exists
periodontal debridement (scaling)

Roles
Clinician: This role involves providing direct patient care through clinical services. Examples include working in private practice, dental specialties (like orthodontics or pedodontics), and hospitals.
Public Health: These professionals focus on enhancing access to care within the community, often in programs funded by governments or non-profits. Work settings include community clinics, schools, and the armed forces.
Corporate: This role centers on the promotion of product development and services. Examples include product sales or acting as a corporate educator.
Researcher: Researchers conduct studies to test new products, procedures, and theories. They typically work for universities, corporations, or government agencies.
Educator: Educators use educational theory and methodologies to train oral healthcare professionals. They may work in traditional clinical education, continuing education, or corporate education.
Administrator: This role involves applying organizational skills to manage resources and evaluate programs. An example is a program director in a clinical, educational, or corporate setting.
Entrepreneur: Entrepreneurs initiate new oral health-related enterprises. Their work can include practice management, consulting, developing new products, or being a professional speaker.
Level of Supervision
Direct Supervision: dentist is required to be physically present while procedures are performed

Personal Supervision: dentist authorizes procedure, present, and check the work before patient is dismissed

General Supervision: dentist authorize procedure for patient, but they do not need to be present when hygienist carries out work
Direct Access Supervision: hygienist provides services without specific authorization
limited to preventative services provided in public health or alternative practice settings, such as schools, nursing home facilities, or free clinics

Collaborative Supervision: Services are provided without supervision, but works in collaboration with dentist

Remote Supervision: dentist supervises work through use of technologies, such as tele-dentistry

Independent Practice: practice without any authorization from a dentist

Effective Communication, Interviewing and Counseling:
Terms:
Health Literacy: Ability of a patient to understand and respond to health info and make decisions
Personal: ability to make health-related decisions

Organizational: ability of organizations in finding and using health information

Feedback: receiver’s direct response to a message

Affirmation: to validate a patient’s effort toward change
Ambivalence: conflict feelings towards making a change
Elicit: to draw forth or bring out

Evocation: Drawing out thoughts through open-ended questions

Active listening: being fully engaged and demonstrating that you are listening
Reflective listening: responding with a summary or statement that shows understanding (not just repeating words)
Preventative counseling: guidance to help patients improve oral health using motivational interviewing

Sustain talk: patients argument for not changing

Change talk: Patients self-expressed arguments for change

Social Determinants of Health: conditions in which people are born, grow, live, work, play and age
Encode Vs Decode
Encode – communicators’ translation of thought into words, gestures, or signs
Decode – receiver’s ability to take in words to recreate encoded thought
Foundations of Communication
Types of Communication
Verbal: based on language and words
Verbal/vocal – spoken language

Verbal/non-vocals – signs or signals: writing, braille, sign language

Nonverbal: based on characteristics of language
Nonverbal/vocal
qualifiers: volume, pitch, tempo, cadence
characteristics: crying, laughing

Nonverbal/non-vocal
body language, movement of body and eyes, facial expressions
Barriers to Communication:
Dysarthria – a motor disorder that paralyzes muscles of the face, mouth, larynx, and vocal cords
resulting in slurred, difficult-to-understand speech

Aphasia – loss of power of expression and comprehension of language

Physical barrier – noise levels, not positioned face-to-face

Physiological barrier – inability to see, hear, touch, or vocalize to communicate

Psychosociological barrier – emotional factors, pain, or fear

Motivational Interviewing
Purpose: A tool used to elicit and strengthen patient motivation for positive behavior change
Core Processes
Engaging
connection and working relationship
Focusing
direction about change
Evoking
eliciting movitation for change
Planning
commitment to a plan of action
Spirit of MI – PACE
Partnership
Create a positive, non-intimidating environment
Listen more → talk less
Acceptance
Absolute Worth: respect the patient as a human being
Accurate Empathy: understand the patient’s perspective
Autonomy Support: respect patient choice
Affirmation: encourage hope and belief in change
Compassion
Prioritize patient needs over clinician's agenda
Builds trust
Evocation
Draw out patient strengths, thoughts, and ideas
Build on what the patient shares

Guiding Principles – RULE
Resist the Righting Reflex
Avoid the urge to “fix” the patient
Understand the Patient’s Motivation
Identify their reasons for change
Listen to the Patient
Practice active listening
Empower the Patient
Support autonomy
Outcomes improve with patient involvement

Core Skills – OARS
Open ended questions
Affirmations
validate efforts
Reflective listening
Summary


Assess Commitment to Change
Low-Level:
I’ll think about it
I’ll consider it
I plan to
I hope to
I’ll try to

High-Level:
I will
I am ready
I promise
I intend to

Dentifrice and Mouth-washing
Active Ingredients:
Cavity Protection and Remineralization:
prevents caries and ↑ remineralization
Fluorides: sodium fluoride, stannous fluoride, sodium monofluorophosphate
Others: xylitol, ACP, CPP-ACP
Biofilm and Gingivitis Reduction:
↓ inflammation and bleeding
Ingredients: Stannous fluoride and zinc citrate
Sensitivity Protection:
occludes dentin tubules and block nerves
Potassium: 5% Potassium nitrate, potassium citrate, potassium chloride
Others: stannous fluoride, strontium chloride, strontium acetate, arginine calcium carbonate, novamin
tartar control:
↓ supragingival calculus
Pyrophosphate: pyrophosphate, sodium hexametaphosphate, tetrapotassium pyrophosphate
Others: zinc chloride, zinc citrate, tetrasodium
malodor control:
↓ VSCs
Ingredients: essential oils, chlorine dioxide, cetylpyridinium chloride, sodium hexametaphosphate, stannous fluoride
Stain Reduction/Whitening:
↑ whitening effect, ↓ stain embedded in acquired pellicle
Phosphate: tetrasodium pyrophosphate, sodium tripolyphosphate, sodium hexametaphosphate
Peroxide: hydrogen peroxide, carbamide peroxide
Inactive Ingredient:
Detergent (surfactant): foam and cleanse
sodium lauryl sulfate
sodium N-lauryl sarcosinate
Abrasive: clean and polish
silica and silicate
calcium carbonate
calcium pyrophosphate
aluminum oxide
bicarbonate
Binder: thickener/stabilizer
mineral/seaweed colloid
xanthan gum
carrageenan
synthetic cellulose
Humectant: moisture stabilizer
glycerol
sorbitol
synthetic cellulous
vegetable oils
Preservation: prevent bacterial growth
alcohol
benzoates
dichlorinated phenols
Flavoring: sweeteners
essential oils (peppermint, cinnamon, wintergreen, clove)
artificial non-cariogenic (xylitol, glycerol, sorbitol)
Mouth-rinse Active Ingredients:
sodium fluoride:
↓ demin
↑ hypersensitivity
stannous fluoride: taste alternation, may stain
↓ demin, hypersensitivity
↑ remin, staining
chlorehexidine
↓ biofilm, gingivitis
8-12 hr substantibity
↑ supragingival calculus
DO NOT USE AFTER BRUSHING WITH SLS
cetylpyridinium
0.05-0.07% OTC rinse
burning sensation
tissue sloughing
sanguinarine
risk of oral leukoplakia
potential carcinogen
phenolic related essential oils
contradicted for recovering alcoholics
burning sensation
oxygenating agents
reduce NUG/NUP
oxidizing agents
reduction of malodor
short term
Case Studies
Case Study 1:
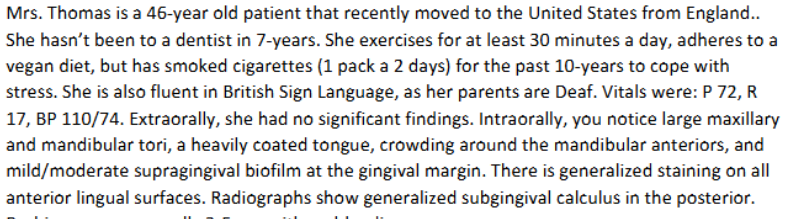
Mrs. Thomas ASA Classification is…
a. I
b. II
c. III
d. IV
ANSWER: gen. healthy but smoker → mild systemic disease
Sign language is a form of __ communication
a. nonverbal, non-vocal
b. nonverbal, vocal
c. verbal, non-vocal
d. verbal, vocal
ANSWER: verbal → communication; non-vocal → no noise
What explains absence upon bleeding?
a. mid biofilm induced gingivitis, does NOT bleed
b. healthy with no signs of disease in oral cavity
c. blood vessels have been constricted by smoking cigarettes
d. early stages of periodontal disease does not bleed, only moderate and severe forms bleed
ANSWER: nicotine causes vasoconstriction in gum tissues, supressing blood flow
Which clinical service includes providing education on importance of routine dental care and smoking cessation?
a. educational
b. therapeutic
c. preventative (primary)
d. preventative (secondary)
ANSWER: education is to make positive changes in patients (via dental care and smoking cession to improve health; preventative is to arrest diseases BEFORE it occurs.
Which instrument would remove subgingival calculus?
a. air-polish with sodium bicarbonate
b. cavitron with universal and slime line insert
c. chisel slacer around mand. anterior teeth
d. detect with 11/12 exploerer
e. scale with gracey 11/12 and 13/14
__ from cavitron will scatter calculus from surface of the tooth
a. acoustic turbulence
b. cavitation
c. irrigation
d. mechanical vibration
ANSWER: cavitrons functions to convert electrical frequency to mechanical vibrations
Which statement is FALSE regarding use of cavitron?
a. start at base of pocket
b. use slow to medium stroke
c. light tapping motion on larger deposit
d. explore and follow up with hand-instruments after use
ANSWER:
What is the BEST choice for polishing the stains Mrs. Thomas teeth?
a. air polisher with calcium sodium phosphosilicate
b. air polisher with sodium bicarbonate powder
c. cleaning paste with the RDH handpiece
d. coarse polishing paste with the RDH handpiece
ANSWER: by process of elimination, calcium phosphosilicate is destructive to enamel; handpiecings arent desidgned to remove stains, polishing paste can be abrasive compared to air polishing (function to remove biofilm and staining)
What is the BEST dentrifice to help her control supragingival calculus formation?
a. potassium nitrate
b. sodium hexametaphosphate
c. sodium fluoride
d. stannous fluoride
ANSWER: tartar control functions to reduce supragingival calculus; sodium hexametaphospahte is an ingredient under such
A humectant in the dentifrice you choose:
a. moisture stabilizer
b. polishing agent
c. thickener
d. lowers surface tension