The Gastrointestinal System (Chapter 27)
The organs of the gastrointestinal (GI) system are the mouth, pharynx, esophagus, stomach, small intestine, large intestine, rectum, and anus.
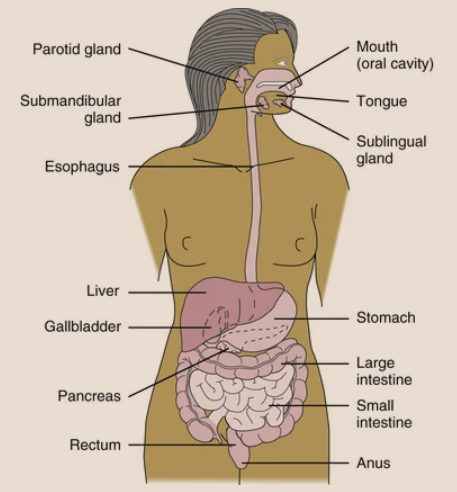
The accessory organs are the liver, gallbladder, and pancreas.
Key Digestive Sphincters
🔹 Gastroesophageal Sphincter (Cardiac Sphincter):
Controls the opening from the esophagus to the stomach.
Prevents reflux, which means it keeps stomach contents (like acid) from going back up into the esophagus.
A one-way door into the stomach.
📍 Location of the Stomach:
Found in the upper left part of the abdominal cavity.
🔹 Pyloric Sphincter:
Controls the exit from the stomach to the small intestine.
Releases food slowly into the small intestine for further digestion.
Acts like a valve to time food movement properly.
Digestive System: Small & Large Intestine + Layers
🔹 Small Intestine (about 6 meters long)
Divided into 3 parts:
Duodenum
Jejunum
Ileum
The Ileocecal valve controls movement from the small intestine into the large intestine.
🔹 Large Intestine (about 1.5 meters long)
Divided into:
Cecum (first part, where the appendix is attached)
Colon
Rectum
Anal canal
The Colon has 4 parts:
Ascending colon
Transverse colon
Descending colon
Sigmoid colon
The Appendix is a small, tube-like structure attached to the cecum—it has no known role in digestion.
Wall of the Digestive Tract (has 4 layers):
Mucosa – the innermost layer; where absorption and secretion happen.
Submucosa – supports the mucosa; contains blood vessels and nerves.
Muscular layer – helps move food along.
Serosa (Serous layer) – outermost covering of the digestive organs.
🔹Peritoneum
A serous sac that:
Lines the abdominal cavity
Covers and protects organs like the intestines, stomach, liver, spleen
Also partially surrounds the uterus and uterine tubes
Functions of the GI System
🔸 Mouth
Teeth and tongue help with chewing (mastication).
Chewing breaks food into smaller pieces for enzymes to work better
🔸 Swallowing & Movement
Food moves:
From mouth → pharynx → esophagus
Moved by peristalsis (wavelike motion of involuntary muscles).
🔸 Stomach
Mixes food with secretions:
Mucus
Hydrochloric acid (HCl)
Intrinsic factor
Pepsinogen
Gastrin
Food turns into chyme (a partially digested, semiliquid mix).
🔸 Small Intestine
Chyme enters and mixes with:
Digestive enzymes
Bile (from liver)
Pancreatic enzymes
Further digestion occurs.
Peristalsis moves the food along.
Nutrients absorbed into the blood through villi on the walls.
🔸 Large Intestine
Reabsorbs water and electrolytes.
Helps make vitamin K.
Eliminates waste.
Contains good bacteria that help break down leftover waste.
🔸 Rectum & Anus
Rectum stores feces until elimination.
Internal anal sphincter – involuntary control.
External anal sphincter – voluntary control.
🔸 Gastrocolic Reflex
Triggered when you eat food.
Stimulates bowel movement.
You can stop this reflex by tightening the voluntary anal sphincter.
Control of the Gastrointestinal (GI) System
The lining of the intestines has receptors that:
Communicate with the nervous system.
Work with the endocrine system.
These systems help:
Release digestive hormones.
Release enzymes for digestion.
Start peristalsis (muscle movements that push food through the GI tract).
Effects of Aging on the GI System
Swallowing muscles weaken → food may get stuck in the cheeks or throat.
Esophageal sphincter works less efficiently → higher risk of aspiration (food going into lungs).
Taste buds shrink → harder to taste flavors, especially salty and sweet.
After age 70:
Less hydrochloric acid, enzymes, and intrinsic factor in the stomach.
Low intrinsic factor can lead to pernicious anemia.
Small intestine absorbs nutrients less effectively.
Large intestine may slow down → less movement of waste.
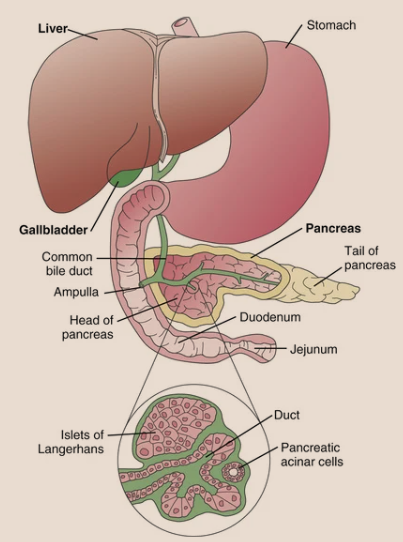
Accessory Organs – Structure & Location
Gallbladder: Small sac under the liver, stores bile.
Liver: Large reddish-brown organ in the upper right abdomen, under the diaphragm, protected by ribs.
Portal vein: Carries blood with nutrients from the small intestine to the liver.
Pancreas: Flat organ behind the stomach, shaped like a long leaf (has a “head” and a “tail”).
Gallbladder connects to the common bile duct, which leads bile from the liver to the duodenum.
Pancreatic duct runs through the pancreas and joins the common bile duct → empties into the duodenum.
Functions of the Gallbladder, Liver, and Pancreas
Gallbladder
Stores bile made by the liver (up to 50 mL).
Releases bile to the small intestine to help digest fats.
Liver
Makes bile and bile salts (needed to digest fat and fat-soluble vitamins A, D, E, K).
Makes blood proteins: albumin, fibrinogen, globulins, and clotting factors like prothrombin.
Stores:
Glucose as glycogen
Vitamins A, D, E, K, B12
Iron
Processes blood from the digestive system through the hepatic portal vein (filters drugs and nutrients).
Metabolizes drugs and detoxifies harmful substances.
Changes ammonia (from protein breakdown) into a safer form.
Breaks down and removes hormones, cholesterol, drugs, and old red blood cells.
Regulates glucose: stores excess glucose, releases when needed.
Helps with fat metabolism and makes cholesterol and phospholipids.
Changes amino acids to support protein metabolism.
Has Kupffer cells to remove toxins and damaged cells from blood.
Can store 200–400 mL of blood as a backup.
Pancreas
Endocrine part (Islets of Langerhans):
Releases insulin and glucagon → controls blood sugar and helps balance electrolytes.
Exocrine part (Acinar cells):
Produces digestive enzymes:
Amylase – for carbohydrates
Protease/Trypsin – for proteins
Lipase – for fats
These enzymes go to the small intestine through the pancreatic duct.
Enzyme release is controlled by secretin and cholecystokinin from the intestinal lining.
Effects of Aging on the Accessory Organs of Digestion
Gallstones are more common in older adults
→ May be due to higher cholesterol in bile and dehydration.Pancreas makes less lipase (a fat-digesting enzyme)
→ Makes fat digestion harder and may lead to poor nutrition.
🌟 The Gastrointestinal System Functions:
Absorption = Nutrients from the intestine move into the blood.
Peristalsis = Muscle movement that pushes food along the GI tract.
Metabolism = All the body’s chemical processes:
Anabolism = Builds/repairs tissues.
Catabolism = Breaks down substances to release energy.
GI Disorders – Causes:
Infections, inflammation, trauma, blockages, or structural problems.
Obstructions can happen from:
Adhesions (scar tissue after surgery),
Tumors, or
Blocked bile/pancreatic ducts.
Irritation of the GI lining can lead to:
Bleeding
Poor nutrient absorption
Increased peristalsis
Emotional Stress & the GI Tract:
Stress affects appetite and movement of food.
It changes how much digestive juice is made.
Too much stress can cause:
Too much acid
Less blood flow to the GI organs
Patient Teaching: Foods That May Contribute to Colon Cancer
The patient should be informed that certain foods may increase the risk of developing colon cancer. These foods include:
Foods Containing Nitrates and Nitrites:
Hot dogs
Bologna and other luncheon meats
Bacon
Ham
Smoked fish
Some imported cheeses (always check the labels)
Nitrates and nitrites are commonly used as preservatives in processed meats. It’s important to read labels carefully when purchasing deli products.
Charred Grilled Foods:
Cooking meat at high temperatures (especially grilling or charring) can produce substances that may increase the risk of cancer.
Health Promotion: Maintaining GI Health
Processed foods with nitrates and nitrites: Research on their link to cancer shows mixed results. However, if other risk factors like high-fat diets, obesity, smoking, or excessive alcohol are present, it's better to limit or avoid these foods.
Autoimmune diseases: Conditions like Crohn’s or ulcerative colitis can cause GI inflammation, and medications (especially radiation and chemotherapy) may worsen GI function, leading to issues like malabsorption.
Lactose intolerance: Common in older adults, lactose intolerance can cause diarrhea and malabsorption.
It’s important for the patient to have regular check-ups and to manage lifestyle factors such as diet, smoking, and alcohol consumption to support GI health.
Prevention of Gastrointestinal System Disorders
Maintaining optimal gastrointestinal (GI) health is essential for preventing various digestive disorders. Here are key strategies for prevention:
1. Diet and Hydration:
Eat a well-balanced, normal-portioned diet: A diet rich in fiber helps maintain a healthy colon and aids in digestion.
Fiber: Insufficient fiber in the diet can lead to conditions like diverticulosis, where pockets form in the colon, trapping waste. Ensure adequate bulk to facilitate smooth passage of waste.
Stay hydrated: Drinking enough water prevents constipation by keeping the stool moist and easy to pass.
2. Healthy Bathroom Habits:
Respond promptly to the urge to defecate: This helps keep the gastrocolic reflex functioning properly and prevents constipation and hemorrhoids.
Avoid straining: Straining at stool increases intra-abdominal pressure, contributing to hemorrhoids and discomfort.
3. Physical Activity:
Encourage mobility: Decreased mobility, especially in older adults, can contribute to digestive issues, so it's important to stay active and mobile.
4. Stress Management:
Manage stress: Chronic stress can lead to ulcers and irritable bowel syndrome (IBS). Developing healthy coping mechanisms can help keep stress in check and maintain gut health.
5. Elimination Diets:
Identify irritants: Use an elimination diet to determine which foods might irritate the GI system. Once identified, the patient can avoid these foods while ensuring proper nutrition.
6. Hygiene and Sanitation:
Good hygiene: Always wash your hands before cooking and eating to avoid foodborne illness.
Sanitize cooking utensils: Ensure that cooking and eating utensils are thoroughly cleaned.
Prevent food poisoning:
Keep meats, mayonnaise-based dishes, and dairy products refrigerated.
Properly store food in the fridge and cover it when not in use.
Follow safe canning, freezing, and food-handling practices.
Causes of Gallbladder Disorders
Gallbladder disorders, particularly the formation of gallstones, can be caused by several factors:
1. Gallstone Formation:
Stones can develop within the gallbladder, causing irritation and increasing susceptibility to inflammation and infection.
When gallstones move into the common bile duct, they can block the flow of bile, leading to obstruction.
2. Rapid Weight Loss:
Severe calorie and fat restriction, especially with gastric bypass surgery or rapid weight loss, can lead to the development of gallstones.
3. Gender and Age:
Women are more likely to develop gallstones than men, with the risk increasing with age.
Obesity and multiple pregnancies also increase the risk because pregnancy causes bile stasis, which contributes to gallstone formation.
4. Medical Conditions:
Diabetes mellitus and Crohn disease are associated with a higher risk of developing gallbladder disorders.
5. Family History:
Genetic predisposition plays a role. Gallbladder disease tends to run in families, suggesting a possible genetic link to the condition.
Cultural Considerations
Genetic Gallstone Risk:
Native Americans: Native American populations, particularly the Pima Indians in Arizona, have a higher risk of gallstones. Many Native American men have gallstones by age 60, and 70% of Pima Indian women have gallstones by age 30.
Mexican Americans: This group also has higher rates of gallstones across both sexes and all age groups due to genetic factors influencing cholesterol secretion in bile.
Prevention of Gallbladder Disorders
To lower the risk of gallstones:
Maintain a normal body weight
Eat a low-fat, low-cholesterol, high-fiber, and high-calcium diet
Avoid rapid weight loss diets
Consume alcohol moderately
Stay active and keep an active lifestyle
Causes of Liver Disorders
Viruses, especially Hepatitis B & C, cause liver inflammation and account for 70% of liver cancer cases
→ Goal: Reduce hepatitis infections (Healthy People 2030)Alcohol and toxic substances lead to cirrhosis
Medications (hepatotoxic drugs):
Acetaminophen (Tylenol): Pain reliever and fever reducer (not for inflammation).
Ibuprofen: Pain reliever and anti-inflammatory (like for headaches, fever, or arthritis).
Erythromycin: Antibiotic used to treat infections.
Phenytoin: Medicine that helps prevent seizures.
Statins (e.g., Atorvastatin): Lower cholesterol to help prevent heart problems.
Methyldopa: Lowers blood pressure (used for high blood pressure, especially in pregnancy).
Sulfonamides: Antibiotics used to treat bacterial infections.
Many others – always check liver function before giving meds
Chemical toxins:
Acetaldehyde: Chemical from alcohol breakdown; can be toxic.
Aerosolized paint: Tiny paint particles in air; can harm lungs.
Cadmium: Toxic metal found in batteries and smoke; damages kidneys and lungs.
Ethyl alcohol: Found in drinks; affects the brain and liver.
Ethylene oxide: Gas used to sterilize; can be harmful and cause cancer.
Mercury: Toxic metal; affects brain and kidneys.
Nitrosamines: Chemicals found in smoked foods and tobacco; can cause cancer.
Paint thinner: Strong-smelling liquid; harmful if inhaled.
Polychlorinated biphenyls (PCBs): Industrial chemicals; can damage immune and nervous systems.
Many cleaning solvents and pesticides: Can be toxic; may irritate skin, lungs, and harm health with long exposure.
Parasites (from contaminated water or food in tropical regions)
Cancer (can start in liver or spread from another site)
Trauma to the liver may cause severe internal bleeding
Prevention of Liver Disorders
Vaccinate against Hepatitis A and B
Test adults for Hepatitis C (vaccine still in trial)
Use Standard Precautions to avoid contact with infected body fluids
Avoid excess alcohol
Avoid toxic drugs and chemicals
Practice good hygiene
Avoid raw oysters/shellfish from contaminated waters
Avoid unprotected sex with high-risk individuals
Causes of Pancreatic Disorders
Pancreatitis (inflammation of the pancreas) is associated with:
Alcoholism: Long-term drinking that damages organs like the liver and brain.
Obstructive gallstones (cholelithiasis): Stones block bile flow, causing pain and digestion problems.
Peptic ulcers: Sores in the stomach or small intestine lining, often from acid or bacteria.
High triglycerides (hyperlipidemia): Too much fat in the blood; increases risk of heart disease. (High Cholesterol)
Trauma
Pancreatic cancer risk increases with:
Age
Smoking
Obesity
Chronic pancreatitis
Diabetes mellitus
Prevention of Pancreatic Disorders
Avoid large amounts of alcohol to prevent pancreatitis
Remove gallbladder if gallstones are present to prevent duct blockage
Keep triglyceride levels below 200 mg/dL
Quit smoking to lower risk of both pancreatitis and pancreatic cancer
Diagnostic Tests for Gastrointestinal (GI) Disorders
Test | Purpose | Description | Nursing Implications |
|---|---|---|---|
Upper GI Series (UGI) | Locate obstruction, ulceration, or growths in esophagus, stomach, duodenum | Patient drinks contrast medium; x-rays taken in various positions | NPO 8–12 hrs; explain procedure; give fluids and laxatives after; stool may be white up to 3 days |
Barium Enema (BE) | Locate tumors, obstruction, ulceration in colon | Radiopaque enema followed by air for contrast | NPO 8 hrs; bowel prep with laxatives/enemas; post-care same as UGI |
CT – Abdomen | Detect tumors, cysts, abscesses, inflammation, bleeding | Combines x-rays and computer to make sectional images | NPO 4 hrs if oral contrast used; consent needed; check for iodine/shellfish allergy; explain test |
Virtual Colonoscopy (CT Colonography) | Detect polyps or abnormalities in colon | Helical CT scan with oral contrast | May take oral contrast 1 day prior; lie still; remove metal; encourage fluids after if barium used |
MRI with or without Contrast | Detect abnormalities in liver or other structures | Uses magnetic field and radiofrequency signals | No food/fluid restrictions; remove metal; may need anti-anxiety meds; explain thumping noise |
Ultrasonography | Detect gallstones, tumors, cysts | Uses sound waves to create images | NPO after midnight; explain procedure; patient supine and still; test ~30 mins |
HIDA Scan (Hepatobiliary Scintigraphy) | Evaluate bile flow, confirm cholecystitis | IV tracer (99mTc) and imaging camera used | Lie flat; test takes 60–90 mins; minimal radiation |
GI Scintigraphy | Locate site of active GI bleeding | IV radioactive tracer attaches to RBCs for imaging | Same as HIDA; tracer lasts up to 24 hrs for follow-up scans |
EGD (Esophagogastroduodenoscopy) | View esophagus, stomach, duodenum; take biopsies | Scope through mouth; sedation given | NPO 8 hrs; consent; IV access; monitor gag reflex and signs of perforation after |
ERCP | View biliary/common ducts, remove stones or place stents | Scope and fluoroscopy with contrast medium | NPO after midnight; consent; post-care same as EGD |
Flexible Sigmoidoscopy | View rectum and sigmoid colon | Scope through anus, biopsy or remove polyps | Bowel prep; clear liquids night before; observe for bleeding afterward |
Colonoscopy | View entire colon lining | Sedation; scope through rectum; biopsy/removal of polyps | Clear liquid diet 1–3 days; NPO 8 hrs; bowel prep; monitor for bleeding or perforation |
Ambulatory pH Monitoring | Detect and measure gastric reflux | Thin pH tube inserted transnasally | (Info incomplete; if needed, I can complete this part too |
Liver Biopsy (percutaneous needle biopsy) | Remove liver tissue sample for diagnosing liver disorders | Under local or general anesthesia, a special needle is inserted through abdominal wall to aspirate liver tissue | Verify informed consent; NPO 4–8 hrs; check coagulation studies; assess allergies; baseline vitals; patient supine or left lateral; hold still; needle inserted on exhalation; lasts ~15 min; monitor for pain, bleeding, respiratory issues; post-care: lie on right side with support 1–2 hrs; vitals q15min x1 hr, q30min x4 hrs, then q4h x24 hrs; avoid coughing, straining, heavy lifting 1–2 weeks |
Laboratory Tests Overview
Test Name | Purpose | Normal Values | Specimen Type | Nursing Considerations |
|---|---|---|---|---|
Fecal Analysis | Observe shape, odor, color, consistency; analyze for mucus & fat | — | Stool | Explain test, provide collection means, deliver promptly to lab |
gFOBT / Hemoccult | Test for occult blood, screen for colon cancer | — | Stool smear | Avoid red meat 3 days before test |
iFOBT / FIT | Test for occult blood, colon cancer screening | — | Stool sample | No dietary restrictions |
Stool Culture | Detect bacteria, fungi, parasites, viruses | — | Stool | Collect in clean container; send promptly to lab |
Serum Bilirubin | Detect abnormal bilirubin metabolism | Total: 0.3–1.0 mg/dL | Blood | Protect from light, fasting may be needed |
ALT (Alanine aminotransferase) | Detect liver disease | 4–36 IU/L | Blood | No fasting required |
AST (Aspartate aminotransferase) | Detect liver damage, hepatitis, biliary obstruction | 0–35 units/L | Blood | Prevent hemolysis; IM injections can affect levels |
ALP (Alkaline phosphatase) | Detect liver tumors, biliary obstruction | 30–120 units/L | Blood | No fasting required |
Ammonia | Detect severe liver disease with encephalopathy | 10–80 mcg/dL | Blood | May need to ice sample |
GGT (Gamma-glutamyl transferase) | Detect liver dysfunction, biliary disease | 8–38 units/L | Blood | Avoid alcohol and certain drugs |
Total Protein | Detect altered protein metabolism | 6.4–8.3 g/dL | Blood | No fasting required |
Albumin | Detect altered protein metabolism | 3.5–5.5 g/dL | Blood | No fasting required |
Prothrombin Time (PT) | Monitor clotting ability | 11.0–12.5 sec | Blood | INR used more often; apply pressure after draw |
INR (International Normalized Ratio) | Monitor anticoagulant therapy | 0.8–1.1 | Blood | Used to manage medication levels |
PTT (Partial thromboplastin time) | Detect clotting deficiencies (stage II) | 60–70 sec | Blood | Used to manage heparin therapy |
aPTT (Activated PTT) | Detect liver failure effects on clotting | 20–35 sec | Blood | Draw 30–60 min before next heparin dose |
H. pylori Antibody | Detect H. pylori infection (ulcers, gastritis) | None present | Blood | No fasting needed |
Special Considerations for GI Diagnostic Tests
Allergy Check:
Always verify if the patient has allergies to contrast media or injectable markers before any diagnostic test.
For women of childbearing age, a pregnancy test might be ordered before testing with radiation or contrast.
Correct Test Order (to avoid contrast interference):
1⃣ Gallbladder sonogram
2⃣ Barium enema
3⃣ Upper GI series
CT Colonography (Virtual Colonoscopy):
A non-invasive test for colon cancer screening.
Combines spiral CT scan images to create a 3D picture of the colon.
No sedation needed and less expensive than a standard colonoscopy.
If something abnormal is found, the patient will still need a regular colonoscopy to take tissue samples.
Colon Cancer Screening Guidelines:
Begin screening at age 45.
Yearly:
High-sensitivity fecal occult blood test (FOBT)
Or fecal immunochemical test (FIT)
Every 3 years:
Stool DNA test
Preparation for Diagnostic Tests:
Patients need clear instructions before any GI test.
Many tests require GI tract cleansing (often with laxatives).
Poor bowel prep may cause delays or require retesting.
Tip: Liquid laxatives are easier to take when chilled or served over ice.
Clinical Cues for Comfort During Preparation
For patients with nausea:
Sucking an ice cube before drinking the prep solution can help.
Using a straw reduces taste sensation.
NPO Considerations:Most GI tests require the patient to be NPO the night before.
In the hospital:
Offer mouth care in the morning.
Keep the room door closed to avoid food smells increasing hunger.
After the test:
Get a food tray quickly once NPO is lifted.
Offer juice, water, tea, or coffee while waiting for the tray.
Watch for Signs of Dehydration:Especially in patients with vomiting, nausea, or diarrhea.
Lack of intake plus illness can cause quick dehydration.
Nursing Management: Assessment (Data Collection)
History Questions:
Family history
Diet and food intolerances
Pain
Bowel movement patterns
Toxin/chemical exposure
Blood clotting issues
Immunization status
Liver Disease Consideration:
Assess all systems due to the liver’s many functions.
Physical Assessment
1. Oral and Skin Inspection
Check teeth, gums, and oral mucosa for issues.
Observe the skin for:
Color changes
Lesions
Discolorations on the abdomen
Look for edema and ascites (fluid in the abdomen):
Signs: Marked abdominal distention, taut and glistening skin
2. Abdominal Inspection
Check abdomen contour
Look for outpouchings (may indicate a hernia)
Auscultation of Bowel Sounds
Use the diaphragm of the stethoscope.
Important: Always auscultate before palpation or percussion to avoid stimulating movement that’s not naturally present.
Normal sounds: Soft gurgles and clicks every 5 to 15 seconds
Normal frequency: 5 to 30 sounds per minute
Loud, frequent sounds = Excessive bowel motility
Clinical Cue:
To call bowel sounds absent, listen to all 4 quadrants for 5 minutes each.
Hypoactive sounds = No sounds in each quadrant for 30 seconds
Hyperactive, high-pitched sounds in one quadrant and decreased sounds in another = possible intestinal obstruction
Check for nausea and vomiting
Palpation
Use light palpation over each quadrant
Look for:
Tenderness
Masses
Watch the patient’s facial expressions for discomfort
Do not palpate if a pulsating mass is found—may indicate an abdominal aneurysm
Percussion
Tap with finger technique to assess sound:
Resonant sound = over air-filled areas
Dull, thudding sound = over solid organs
Helps detect excessive air (often from inflammation or irritation)
Assessing for Ascites
Position patient:
Supine, arms at sides, knees flexed
Check for bulging flanks (fluid buildup)
Measure abdominal girth:
Measure at the umbilicus
Mark measurement sites with ink for consistency
Shifting dullness test:
Percuss from umbilicus to flanks
Dullness in lower sides = fluid has shifted
Lab and Stool Assessments
Check urine:
Dark/tea-colored urine = bilirubin present
Check stool:
Fat in stool = stool floats
Clay-colored or white stool = bile not reaching intestines
Check for urobilinogen (substance formed when the liver breaks down bilirubin. It is found in urine and stool)
Focused Assessment of the Gastrointestinal System and Accessory Organs
Mouth: Check the condition of teeth, gums, and mucous membranes.
Swallowing: Assess the patient's ability to swallow.
Skin: Inspect for color changes, discoloration, visible vessels, and bruising.
Sclera & Mucous Membranes: Check for icterus (yellowing).
Abdomen: Observe the contour.
Bowel Sounds: Auscultate all four quadrants.
Palpation: Lightly palpate each quadrant of the abdomen.
Percussion: Percuss if intestinal irritation or inflammation is suspected.
Ascites: Measure abdominal girth if ascites is present.
Stool: Inspect for characteristics and test for occult blood if needed.
Urine: Inspect for color.
Anus: Check for external hemorrhoids.
Vomitus: If vomiting occurred, inspect the vomitus and test for blood if indicated.
Common Problem Statements, Expected Outcomes, and Nursing Interventions for Patients with Gastrointestinal Disorders:
Problem | Goals/Outcomes | Nursing Interventions |
|---|---|---|
Fluid Volume Deficit (nausea, vomiting, diarrhea) | - Vomiting and diarrhea controlled in 24 hours. | - Monitor urine output and hydration. |
Altered Nutrition (anorexia, nausea, vomiting) | - Patient will ingest at least 1200 calories/day. | - Provide mouth care. |
Diarrhea (intestinal infection/inflammation) | - Infection resolves within 72 hours. | - Administer medications (antibiotics, anti-inflammatory). |
Constipation (medications, diet, inactivity) | - Regular bowel movements within 2 weeks. | - Increase fluids, fiber, and exercise. |
Incontinence (rectal sphincter issues) | - Continence achieved within 1 month. | - Start bowel training program. |
Limited Coping (stress) | - Patient will learn coping methods within 2 months. | - Teach relaxation and stress management techniques. |
Implementation
Nursing interventions for gastrointestinal (GI) issues include:
Pain management: Implement strategies to control and eliminate pain.
Fluid and electrolyte balance: Monitor and correct imbalances.
Nutrition support: Promote adequate nutrition through proper diet and supplements.
Rest and healing: Encourage rest to support recovery.
Complication prevention: Monitor and address potential complications like constipation, impaction, or infection.
Note: Nurses should ask every patient about bowel movements daily, especially in the hospital setting, to prevent constipation and possible impaction.
Evaluation
Lab values: Regularly analyze laboratory results to assess progress and response to treatment.
Eating and bowel patterns: Evaluate if the patient's eating habits and bowel functions are normalizing.
Side effects and complications: Continuously monitor for adverse effects from medications or the disease itself.
Documentation: All evaluation findings and actions must be documented for continuity of care and legal purposes.
Common Problem: Anorexia
Definition:
Anorexia is the absence of appetite, often caused by physical, mental, or environmental factors.
Physical Causes:
Poorly fitting dentures
Stomatitis (mouth inflammation)
Decaying teeth or bad taste in the mouth
Pain, nausea, or GI infections
Diseases of the GI tract
Psychological Causes:
Emotional states like anxiety, anger, fear, or depression can decrease appetite.
Unattractive or unfamiliar food, unpleasant surroundings, or negative mental associations can also reduce appetite.
Nursing Management:
Monitor nutrition: Persistent anorexia requires attention to prevent inadequate nutrition.
Understand causes: Talk with the patient, family, and review the medical record to identify underlying causes.
Mouth care: Provide mouth care before meals to minimize oral issues affecting appetite.
Monitor labs: Keep track of albumin and electrolyte levels.
Document intake: Note and document the percentage of each meal eaten.
Older Adult Considerations:
Age-related changes: Reduced taste and smell, poor dental health, or polypharmacy (multiple medications) can affect appetite.
Dental issues: Dentures or missing teeth may make eating painful, and polypharmacy may decrease appetite.
Interventions for Older Adults:
Offer preferred foods if health allows.
Make meals more appealing with a variety of colors, textures, and tastes.
Nausea and Vomiting
Impact:
Persistent nausea and vomiting can significantly interfere with eating and nutrition. It can be caused by various factors, including illness, medications, anesthesia, pain, cancer treatments, or stress. While transient nausea may not require treatment, ongoing issues are managed with antiemetics and IV fluids.
Nursing Management:
Smells can worsen nausea: Ensure that health care personnel avoid using strong-scented self-care products (e.g., laundry detergent, lotions, hair products, soaps, deodorants) that could exacerbate nausea in sensitive patients.
Complementary and Alternative Therapies:
Ginger for nausea:
Ginger has long been used to alleviate nausea, motion sickness, and indigestion.
Available in various forms, including candied, capsules, fluid extracts, and tea made from fresh gingerroot.
It has antiplatelet properties and should be used cautiously in patients on anticoagulant medications.
Accumulation of Flatus (Gas)
Cause:
Obstructions, surgeries, or injuries to the intestinal tract can impede gas and fecal material flow, leading to distention and bloating.
Nursing Management:
Encourage ambulation: Moving around can help with peristalsis and reduce bloating.
Trendelenburg position (if permitted):
Raise the patient's buttocks and legs above their head to allow gas to rise toward the rectum, easing its expulsion.
Gentle abdominal massage:
Start on the right side, move across the abdomen, and finish on the left to help move gas along the colon.
Avoid abdominal incisions when massaging.
Avoid extreme temperatures: Advise against chilled or hot drinks, as they may worsen bloating.
Use of antiflatulent medications: Medications like simethicone (e.g., Phazyme) can be helpful if the patient is not NPO.
Patient Teaching (Exercise for Reducing Gas and Bloating):
Leg exercise:
Lie on your back, legs extended with a pillow under your knees.
Raise and bend your right leg towards the abdomen for 10 seconds, then lower it back.
Repeat with the left leg.
Breathing: Take slow deep breaths between repetitions.
Frequency: Repeat the exercise three or four times with each leg, several times a day, with rest periods between sessions.
Expel gas when needed: Advise patients not to hold back gas.
These interventions can help manage bloating, improve comfort, and encourage the expulsion of gas.
Constipation
Constipation occurs when the stool becomes hard, dry, and difficult to pass.
Symptoms include bloating, painful defecation, and infrequent stool passage.
Causes of Constipation
Dietary Factors:
Low fiber diet and inadequate fluid intake can contribute to constipation.
Physical Activity:
Lack of exercise and physical inactivity can slow down bowel movements.
Neurological Issues:
Certain neurological disorders affecting the nerves in the intestinal tract can cause constipation.
Medications:
Opioid medications slow down peristalsis (intestinal movement) and contribute to constipation.
Other Contributing Factors:
Ignoring the gastrocolic reflex (the urge to have a bowel movement after eating).
Stress can exacerbate constipation.
Treatment for Opioid-Induced Constipation
FDA-Approved Medications for Opioid-Induced Constipation:
Methylnaltrexone bromide (Relistor)
Naloxegol (Movantik)
Lubiprostone (Amitiza)
Naldemedine (Symproic)
These medications are used for opioid-induced constipation in patients with noncancer pain on chronic opioid therapy.
Signs and Symptoms of Constipation
Physical Symptoms:
Hard, dry stool that is difficult to pass.
Hypoactive bowel sounds.
Abdominal distention (swelling).
Firm abdomen.
Abdominal discomfort or pain.
Older Adult Considerations
Increased Risk for Constipation in Older Adults:
Decreased GI motility (slower digestion).
Lack of exercise.
Limited fluid intake.
Constipating medications (e.g., pain medications, iron supplements).
Difficulty reaching the bathroom or suppressing the defecation urge.
Laxative Use:
Older adults often rely on laxatives; this should be discouraged unless necessary.
Instead, increase dietary fiber and fluid intake (about 2500 mL/day of fluids, if not contraindicated by cardiac or renal conditions).
Nursing Management of Constipation
Identify the Cause:
Understand the underlying cause of constipation (dietary, lifestyle, medication, etc.).
Initial Treatment:
Use of rectal suppositories or laxatives to help induce evacuation.
Stool softeners may be prescribed.
Increase fiber and liquid intake.
Ongoing Treatment:
Bulk-forming laxatives (e.g., Metamucil) may be used daily.
If impacted stool occurs, digital extraction may be necessary.
Administer a mild analgesic 30-60 minutes before impaction removal for pain relief.
Oil retention enema followed by lubricants (e.g., K-Y Jelly or lidocaine jelly) for comfort during procedure.
Nutrition Considerations for Constipation
Hydration:
Maintain adequate hydration to keep stool moist and easier to pass.
Daily fluid intake recommendations:
3.7 liters/day for males.
2.7 liters/day for females.
Fluid needs increase with activity or heat exposure.
Foods like fruits and vegetables have high water content.
Dietary Changes:
Add raw fruits and vegetables to the diet.
Incorporate whole-grain cereals and breads.
Add bran to the diet for increased fiber.
Drink plenty of fluids, especially fruit juices (which contain fructose, a natural laxative).
Key Takeaways
Constipation can be caused by dietary, lifestyle, medication, and health factors.
Older adults are at higher risk due to decreased motility and other age-related factors.
Nursing management focuses on identifying the cause, using laxatives and stool softeners, and ensuring proper hydration and dietary intake.
Long-term reliance on laxatives should be avoided, especially in older adults.
Six foods high in fiber that a patient might add to the diet to combat constipation.
Whole grains (e.g., whole wheat bread, brown rice, quinoa, oats)
Legumes (e.g., lentils, black beans, chickpeas)
Fruits (e.g., apples, pears, berries, bananas with the skin on)
Vegetables (e.g., broccoli, spinach, carrots, Brussels sprouts)
Nuts and seeds (e.g., almonds, chia seeds, flaxseeds)
Bran (e.g., wheat bran or oat bran)
These fiber-rich foods help promote regular bowel movements and maintain overall digestive health.
Diarrhea
Diarrhea is the frequent passage of liquid or semiliquid stools.
It occurs due to various causes, such as illnesses, food poisoning, excessive stress, and bowel inflammation.
Causes of Diarrhea
Infections (e.g., bacterial, viral, or parasitic).
Food poisoning (from contaminated food or water).
Excessive stress can also trigger episodes of diarrhea.
Bowel inflammation (such as in conditions like Crohn's disease or ulcerative colitis).
Medications (e.g., antibiotics, which can disrupt the normal gut flora).
Signs and Symptoms
Multiple liquid or semiliquid bowel movements.
Hyperactive bowel sounds (increased activity in the intestines).
Abdominal cramping.
Treatment for Diarrhea
Mild Diarrhea:
Typically not treated unless it persists for more than 24 to 48 hours or causes significant fluid loss.
Antidiarrheal Medications:
Diphenoxylate hydrochloride (Lomotil).
Loperamide hydrochloride (Imodium).
Tincture of opium (paregoric).
Kaopectate (a combination product).
Severe Diarrhea:
Nothing by mouth until symptoms subside to prevent worsening peristalsis (intestinal movement).
Clear liquids only if the diarrhea is moderate.
In cases of severe, long-term diarrhea, Total Parenteral Nutrition (TPN) may be needed.
Infection-related Diarrhea:
Stool cultures and antibiotics may be required if the diarrhea is caused by an infection.
Complementary and Alternative Therapies
Probiotics:
Probiotics can help reduce the risk and duration of diarrhea, especially when used alongside rehydration therapy. These are beneficial bacteria that help restore normal intestinal flora.
Nutrition Considerations for Diarrhea
Foods That Help Thicken Stool:
Once solid foods are reintroduced, gradually offer foods that can help thicken stool:
Applesauce.
Bananas.
Rice.
Bread (white).
Beets.
Potatoes (without skin).
Oatmeal.
Creamy peanut butter.
Pasta.
Tapioca.
Yogurt.
Nursing Management
Monitoring Intake and Output:
Assess and measure the amount of fluid lost in stool.
Monitor the patient for signs of dehydration (e.g., decreased skin turgor, thick oral secretions, decreased urine output).
Fluid and Electrolyte Management:
Replace lost fluids and electrolytes using solutions like electrolyte replacement solutions or Gatorade.
Avoid coffee or tea, as caffeine can stimulate peristalsis and worsen diarrhea.
Hand Hygiene:
Proper hand hygiene is crucial, especially when caring for patients with infectious diarrhea.
Follow Standard Precautions and Contact Precautions if an infection is the cause (e.g., Clostridium difficile infection).
Relief for Discomfort:
Warm sitz baths can help reduce soreness and cleanse the area.
Keep the patient clean and dry to prevent skin irritation.
Managing Odor:
Deodorizing sprays can help reduce unpleasant odors in the room.
Promptly empty and clean bedpans or commodes to maintain cleanliness.
Key Takeaways
Diarrhea is typically self-limiting, but treatment is necessary if it persists or causes significant fluid loss.
Rehydration is a priority, and probiotics can aid in recovery.
Medications like Imodium or Lomotil help reduce symptoms, but severe diarrhea may require fasting and fluids.
Good nursing care involves monitoring fluids, preventing dehydration, and maintaining proper hygiene.
Bowel Incontinence
Bowel incontinence refers to the inability to control bowel movements, leading to the involuntary passage of stool.
This can occur due to severe illness, trauma, neurologic damage, or prolonged bed rest.
Psychological Impact
Bowel incontinence can be embarrassing for alert patients, and it is important to address this issue with sensitivity and care.
Maintaining the patient’s dignity is essential by ensuring they stay clean and dry.
Initial Steps for Managing Incontinence
Track Incontinent Movements:
Keep a log of the times the patient has accidents.
Offer toileting opportunities after each meal to create a routine.
Private Environment:
Ensure that the patient has access to a private space for bowel movements to maintain privacy and dignity.
Bowel Training Program
When incontinence is persistent, a bowel training program may be necessary to retrain the bowel. Key elements include:
Timing:
20 to 40 minutes after a meal: This is the optimal time for bowel movements due to the body’s natural digestive processes.
Positioning:
Encourage a normal sitting position for defecation if the patient can sit up.
If the patient is bedridden, position them in a side-lying position to mimic a normal bowel posture.
Digital Stimulation:
Digital stimulation involves gently inserting a gloved, lubricated finger into the rectal sphincter and rotating it. This mimics the body’s normal defecation reflex.
It should be done regularly to help the patient re-establish a bowel routine.
Additional Stimuli:
Offering a warm drink with lemon or prune juice can help stimulate the bowels and aid in regular bowel movements.
Use of Suppositories:
Suppositories may also be used as part of the bowel training program to help the patient achieve bowel movements.
Consistency and Patience
Consistency and patience are critical to the success of bowel training. It may take time for the patient to regain control over bowel movements, and gradual progress should be encouraged.
Safety Considerations
Always encourage safety during the bowel training process.
Assist the patient in getting to and from the toilet to prevent falls or injury.
Reassure the patient that calling for help is important for both their safety and to monitor the progress of the training program.
Key Takeaways
Bowel incontinence can be distressing for patients, but proper management through a structured bowel training program can help restore control.
Timing, positioning, and digital stimulation are key elements in the program.
Patience and consistency are necessary for success, and maintaining safety and dignity is crucial throughout the process.