L1 - Overview of Regulation of Blood Pressure
Mark Yoeman
Overview - Independent Study is Examined
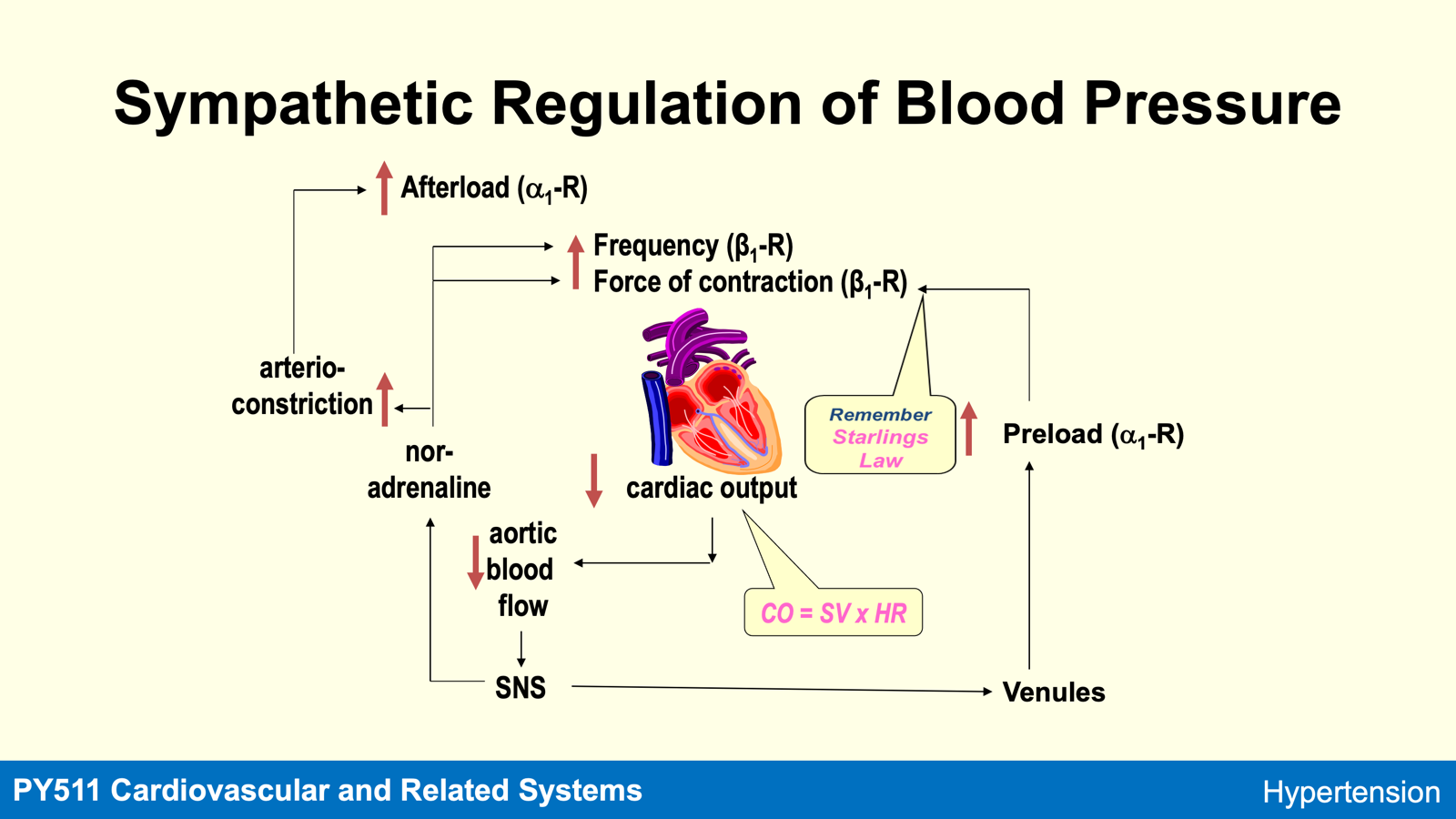
Role played by the sympathetic and renin angiotensin systems in regulating blood pressure.
Role of calcium in regulating cardiac frequency and force of contraction.
Role of calcium in regulating preload and afterload.
Look at “Aspire Reading List” for alternative explanations
Treatment - Appropriate pharmacological treatment requires a knowledge of physiological regulation of BP and how drugs work.
BP = CO x TPR
Blood pressure = Cardiac Output x Peripheral Resistance
Cardiac Output = Stroke Volume x Heart Rate
Cardiac Output = Amount of blood pumped per beat every time the ventricles contract
Stroke volume is regulated by ventricles
Heart rate is regulated by SA node
Total peripheral resistance is a measure of the degree of constriction in arterioles
Afterload generated by ventricle to pump blood into systemic circulation
Preload is a measure of how much the blood stretches the right ventricle
ADH and vasopressin are synonymous
ARB’s block AT1 receptor
ACEi inhibit ACE enzyme
Aldosterone receptor antagonist; Spironalactone
Renin-antagonist
BP and TPR
Increasing Ang II will increase IP3 and therefore increase intracellular calcium. Calcium acts in smooth muscles to constrict arteriols and increase total peripheral resistance. Now BP is increased.
IP3 will always increase calcium in every cell.
BP and Preload
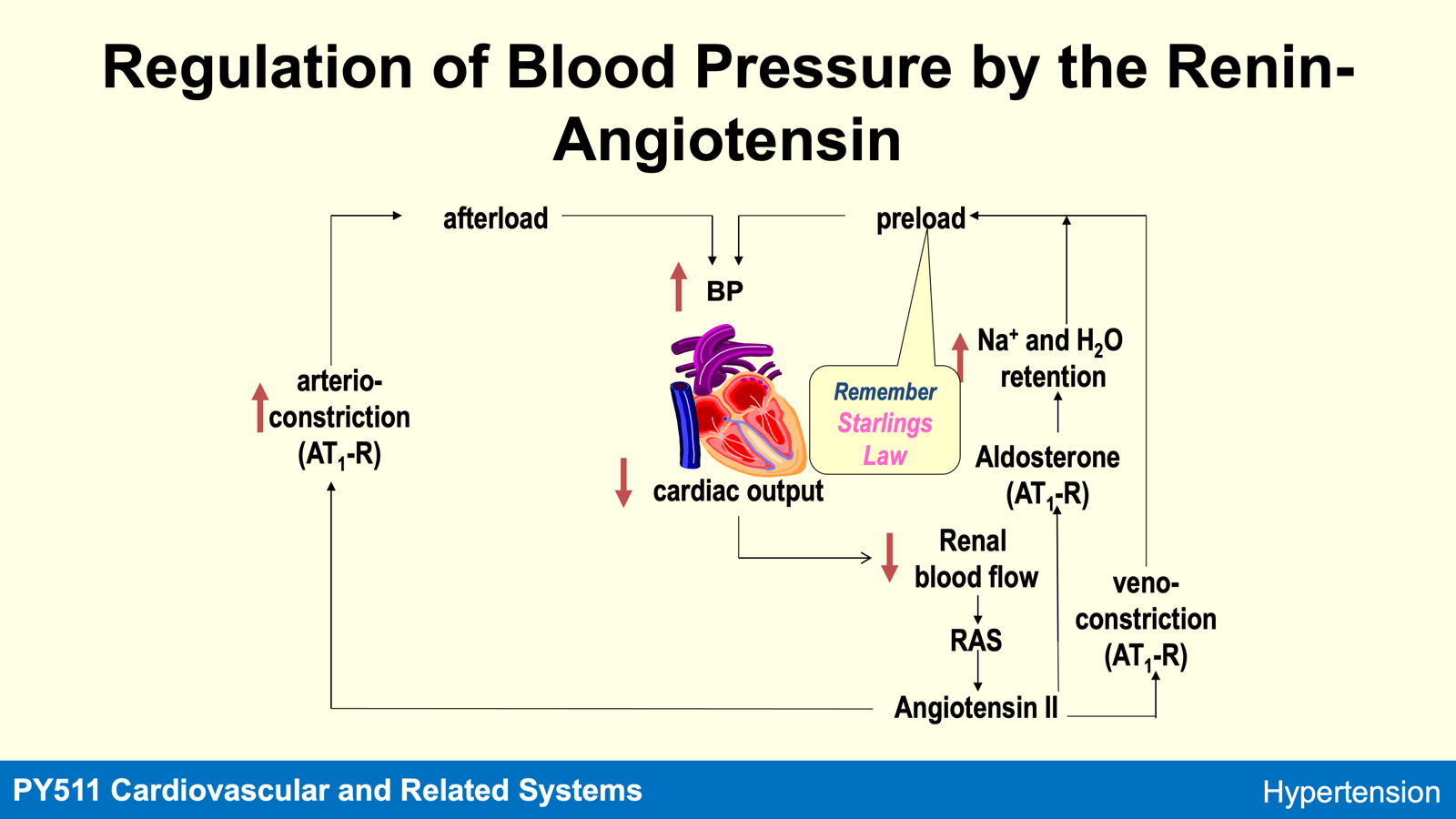
AT1-R will constrict venules.
BP and Aldosterone (RAAS)
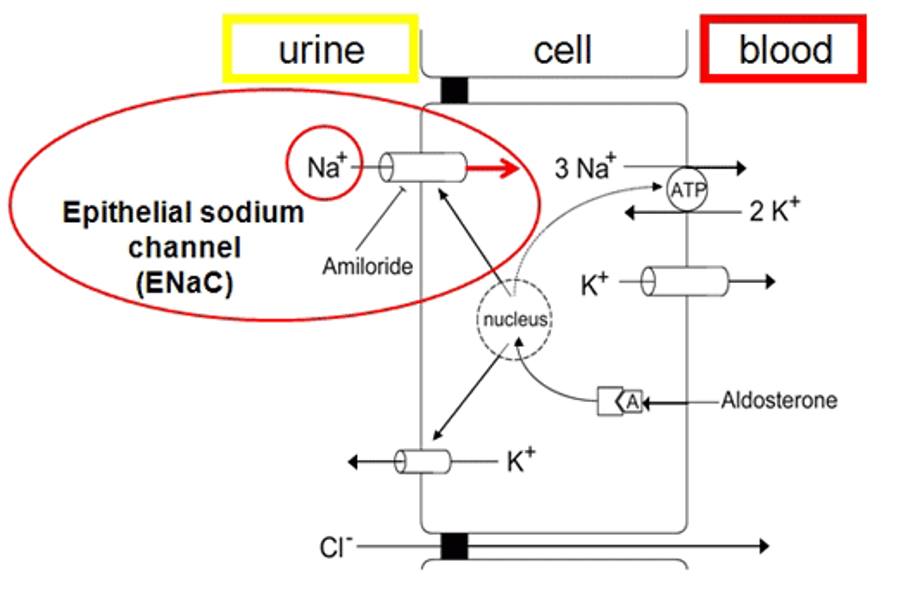
Receptor for aldosterone is not situated in membrane but inside the cell instead.
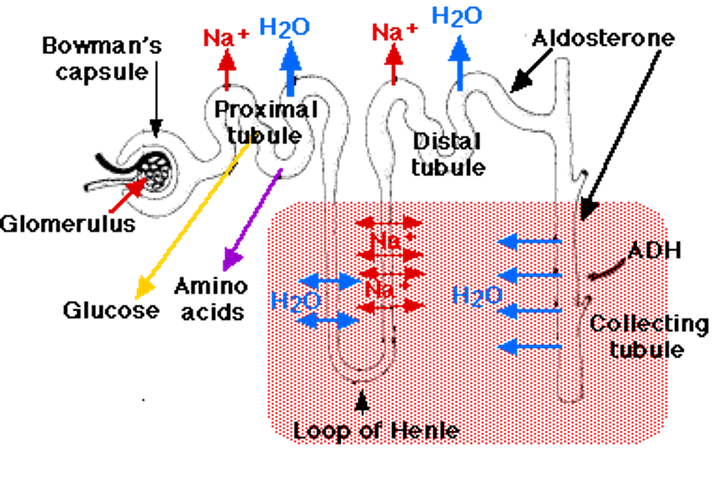
How aldosterone works - Aldosterone is lipophilic, it activates ENaC, the cytoplasmic receptor that binds to the nucleus and increase sodium ion channel expression in the membrane allowing for sodium reaborsorption by diffusion. Water follows sodium.
As sodium concentration builds up in the cell, diffusion rate slows down. Aldosterone therefore makes the nucleus generate a sodium potassium ATPase pump. This means the sodium ions inside the cells move out so the concentration rate can stay the same.
Spironalactone inhibits aldosterone’s ability to bind the mineralcorticoid receptor in the diagram below.
Drug Treatment and Factors to Consider
a) Age
—> if +55 give ACEi or ARB
—> if >55 give CCB
b) Ethnicity
—> Black African’s or Black Americans find ACEi and Beta Blockers less efficacious
c) Co-existing Diseases
Alpha-1 contricts and contracts smooth muscle in blood vessels, urinary tract and iris
Alpha-2 exists in presynaptic terminals and CNS to turn of SNS
Beta-1 increases heart rate, force of contraction (inotropy) and stimulates renin release in kidneys (RAAS)
Beta-2 relaxes smooth muscle, dilates blood vessels in uterus and bladder and breaks down fat for energy and heat.
SAQ: Explain how the renin-angiotensin system increases preload.
Angiotensin-2 also acts on AT1A receptors to constrict venules and that increases preload
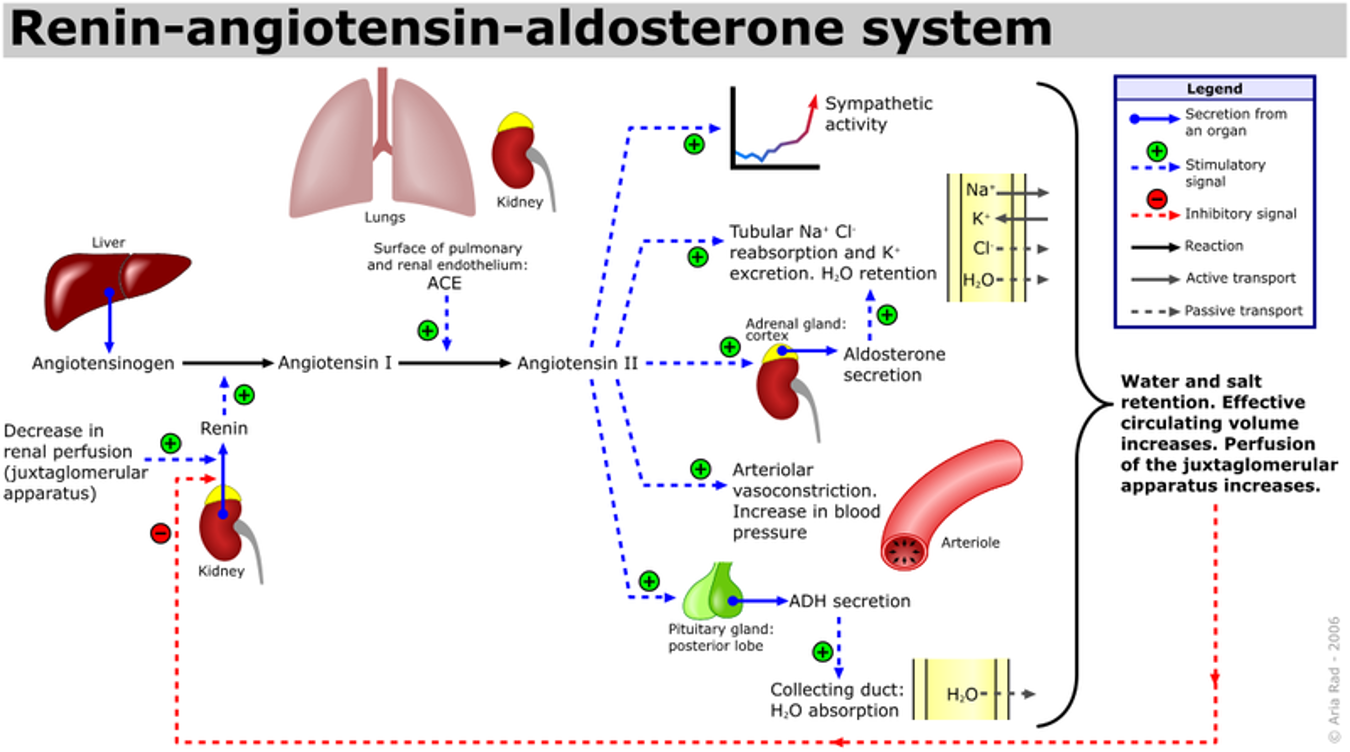
Kidney’s angiotensin AT1A receptors detect a decrease in renal perfusion (flow of blood through kidneys) and drive the release of renin.
Renin converts angiotensin into angiotensin-1 and the angiotensin converting enzyme converts angiotensin-1 into angiotensin-2.
Angiotensin-2 releases aldosterone. Aldosterone steroid will diffuse into the cell binding to mineralcorticoid receptor to bind to the nucleus and activating sodium channels in the membrane to intake sodium from urine.
Sodium will attract water with it and then diffuse out into the blood via sodium-potassium ATPase pump thus moving water out the cell too and increasing blood volume. Salt and water retention increases preload.