Implant Designs and Characteristics
Introduction
Patients desire teeth in good health that provide function, aesthetics and phonetics.
When indicated for missing teeth, dental implants are a means to fulfill these requirements.
This Learning Module will outline the implant design features and characteristics that are aimed at facilitating integration with the hard and soft tissues, allowing them to serve as anchorage elements for prosthetic reconstructions whilst also withstanding occlusal loading forces.
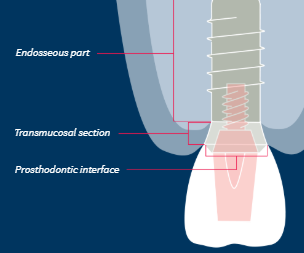
General divisions of implant body
Endosseous: lies within the bone
Transmucosal: lies in the soft tissues between the bone and oral cavity
Interface to the prosthodontic components
Within each of these three parts there are further design characteristics and variations in
shape
features
dimensions
There are also variations in implant body material and surface technology.
Variations in Implant Prosthodontic Interface
The primary implant function is to serve as anchorage for prosthodontic reconstruction whilst also withstanding occlusal loading forces
Implants need an interface with prosthodontic components
Variations in the implant prosthodontic interface are realted to:
Extent of implant contribution to prosthodontic platform
Design of connection to prosthodontic components and the implant
Relationship to the bone crest and neighbouring hard/soft tissues
Implant contribution to prosthodontic platform
Prosthodontic interface can be:
Integral part of the implant
Part implant/part abutment
An abutment is defined as a part or component that serves as support and/or retention for a dental prosthesis
Provided entirely by separate abutment
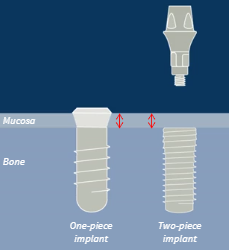
One-piece implant
Provides all or part of prosthodontic platform
Transmucosal design
Fixed neck and built-in emergence profile
Two-piece implant
Separate abutment provides prosthodontic platform
Designed to stop at bone level
More prosthetic flexibility
Useful in sites with limited dimensions and aesthetic concerns (option to select a tooth-coloured abutment)
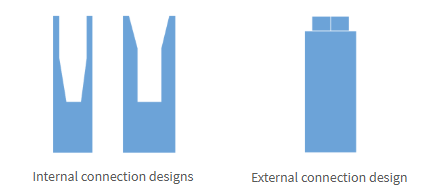
Design of implant connection to prosthodontic components
Internal connection vs external connection
Both types usually have anti-rotational indexing
Examples can be seen with flat sides in the tapered internal connection and with a hexagonal profile in the external connection.
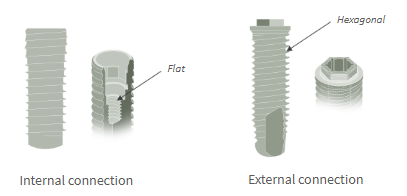
Internal Connections
Can have tapered or straight sides or a combination
Tapered designs provide greater intimacy of fit and stability under load
External Connections
Generally offer a flat shoulder butt fit
Provide less precise abutment fit and stability under load
There is a general shift towards internal connections across most implant systems.
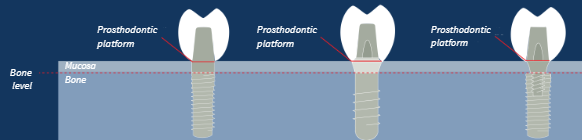
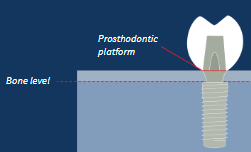
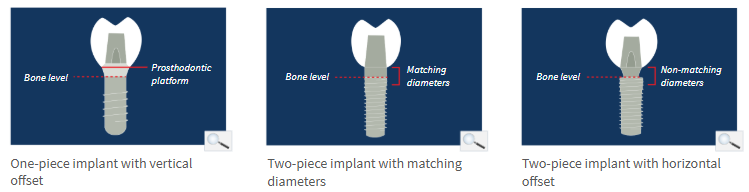
Relationship of implant prosthodontic interface to bone crest
One-piece implants: typically 2-3mm above the bone crest - distance is called vertical offset
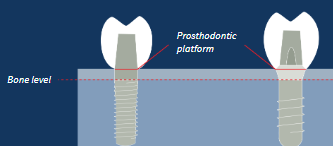
Two-piece implants: the interface is at the bone crest
Can have matching or non-matching abutment diameters
Implant and abutment with matching diameters - butt joint
Implant and abutment with non-matching diameters - horizontal offset
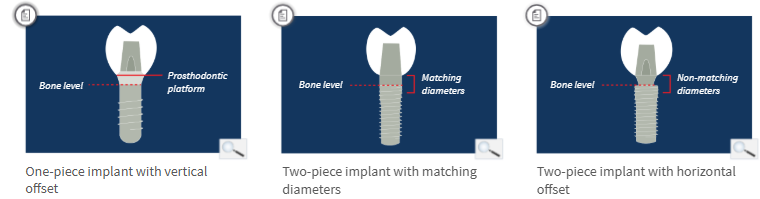
Impact of implant prosthodontic interface on bone crest stability
Vertical offset avoids inflammation at bone crest and allows stable bone levels
Matching diameter is associated with an inflammatory response and 1.5-2.0mm bone loss
Horizontal offset moves the bacterial infiltrate away from the bone crest and reduces bone loss to 0.5mm
Key Points:
One-piece implants provide all or part of the prosthodontic platform, and their transmucosal design offers a vertical offset that promotes stable bone levels.
Two-piece implants are designed to stop at bone level, and the prosthodontic platform is provided by a separate abutment, which offers more prosthodontic flexibility.
A matching diameter of the two-piece implant to abutment interface is associated with greater crestal bone loss than a horizontal offset.
An internal tapered connection to the abutment offers a more intimate fit and greater stability under load than internal straight side and external connections.
Variations in Implant Transmucosal Section
Lies within the soft tissues between bone and oral cavity
One-piece implants: built-in; 2-3mm tall
Two-piece implants: provided by abutment
the transmucosal section is part of a separate abutment that attaches into the implant abutment interface
Promotes soft tissue integration and establishing a biologic width similar to teeth

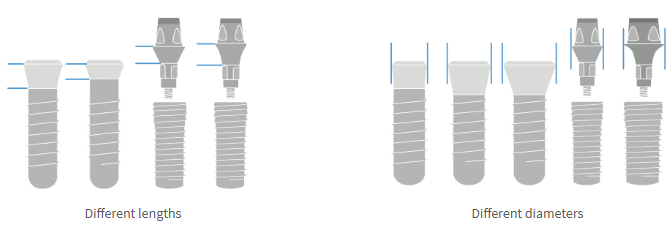
Dimensions
Length: Varies with clinical situation and thickness of mucosa
Diameter: Varies with clinical situation and dimensions of the edentulous space
Both one-piece and two-piece implants offer variations in length and diameter but the two-piece designs are likely to offer greater flexibility of choice.
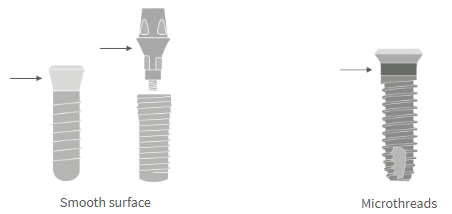
Surface design
Surface: smooth or textured
Most implants have a smooth or machines transmucosal part
Some have textured surfaces as there is some evidence that this may enhance soft tissue attachment
Microthreads: with or without
Key Points:
In a one-piece implant the transmucosal section is built into the implant, while in a two-piece design the transmucosal section is part of a separate abutment.
The length and diameter of the transmucosal section is selected to suit the specific clinical situation.
The transmucosal section may be textured to enhance soft tissue attachment.
Variations in Implant Endosseous Part
Endosseous Part: Shape
Cylindrical (parallel walls)
Conical (tapered walls)
Cylindrical/conical combined (parallel and tapered)
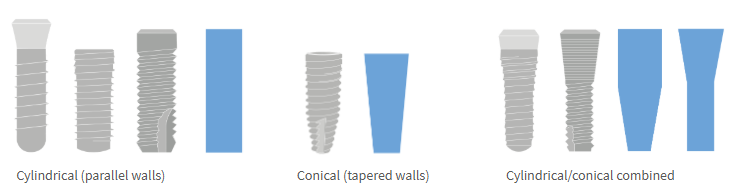
Amount, quality and morphology of available bone influences selection of implant shape
Conical implants typically achieve higher initial stability than cylindrical
Higher stability is required for immediately loaded implants (<1 week)
Implant shape determines osteotomy preparation and drilling intruments used
Endosseous Part: Threads
Helical ridges near the apex, are separated by a groove, usually in a clockwise direction
Functions of a thread
Facilitate insertion of the implant or osteotomy
Assist with initial implant stability (initial bone-to-implant contact is established at the tip of the threads)
Direct loading forces into bone
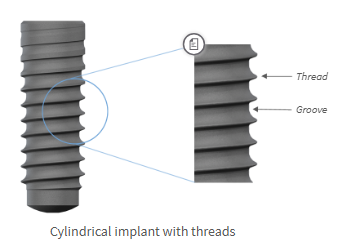
Thread pitch: distance between threads
Pitch varies to suit different bone types
Wider pitch is advantageous for low-density bone; preserves initial stability, reducing the risk of crushing the bone at the junction.
Less common: implants with no threads
Placed by pushing or tapping the implant into the osteotomy

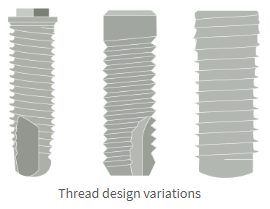
Design variations:
Single or multiple threads
Flat or deep grooves
Self-tapping or non-self-tapping threads
For non-self-tapping designs, tapping is normally required before the implant is inserted.
In situations with low-density bone, placing a threaded implant without prior tapping may help to increase primary stability.
Amount, quality and morphology of available bone influences selection of implant thread design
Apex
Shape: flat, rounded or pointed
Threads: with or without
Bone-cutting ability: with or without
Cut bone, compress bone or be passive with respect to contact with the bony bed when being inserted
Amount, quality and morphology of available bone influences selection of implant apex design
Implant apex affects osteotomy preparation steps and drilling intruments used

Implant dimensions
Length: long/short
6-14mm
Diameter: narrow/standard/wide
3-6mm
Length and diameter of implant depends on prosthodontic and surgical assessment of planned implant site
Key Points
The amount, quality, and morphology of available bone as well as the need for higher initial stability influence the selection of implant body shape.
The thread design contributes to the initial stability of the implant.
The configuration of the implant apex has an impact on the bony bed during insertion.
Prosthodontic and surgical assessment of the planned implant site determines the appropriate length and diameter of the implant.
Variations in Implant Material and Surface Technology
Implant material
Implants are made of various materials
All materials must:
be biocompatible
promote osseointegration
Commercially pure titanium is the material of choice due to its clinical results and long history
Titanium
Titanium allows (e.g. titanium-aluminium-vanadium, titanium-zirconium)
Increased tensile strength
Zirconia
Aesthetic and metal-free
Choice of material depends on clinical situation and patient desires

Surface topography
Surface properties affect osseointegration
Determined during the manufacturing process

Degrees of surface roughness
Categorisation:
Smooth
Minimally rough
Moderately rough
Rough
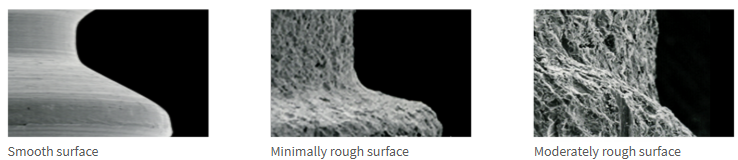
Surface roughness influences osseointegration
Neither smooth nor very rough surfaces promote optimal integration
Moderately rough surfaces promote integration better than other surfaces
Clinical Implications
Moderately rough surface → Higher rate of bone formation (earlier loading) → Greater bone-to-implant contact (shorter implant)
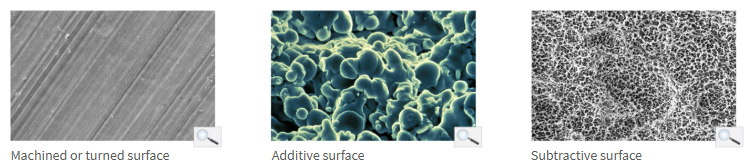
Altering implant surface roughness
Initial grinding process creates machines/turned surface
Additional manufacturing steps produce desired microstructure
Subtractive or additive surface treatments
Mechanical or chemical rocesses
Chemical processes
Altered surface roughness
Remove contaminants
Add chemical compounds to improve bone formation
Sandblasted and acid-etched (SLA and SLActive) surfaces show:
increased surface wettability
enhanced cellular attachment
faster osseointegration
At 2 and 4 weeks, the SLActive surface shows higher bone-to-implant contact than the original SLA surface.
Biological activation
Compounds added to implant surface (e.g. hydroxyapatite)
No tangible clinical benefits
Key Points:
Implants may exhibit different degrees of surface roughness as well as distinct surface features.
These features are produced by a range of mechanical, chemical, and biologic manufacturing processes that may be additive or subtractive.
Surface roughness influences the rate and amount of osseointegration; greater bone-to-implant contact has been observed for implants with moderately rough surfaces.
Chemical and biologic alterations of the implant surface have the potential to increase the process of bone formation at the implant surface.
Summary
Implant design features affect clinical outcomes; therefore, clinical aims govern the choice of implants with specific design features.
Implant design features encompass both macro- and microstructural characteristics.
Implant design features are further associated with chemical and biologic processes.
The amount, quality, and morphology of available bone influences selection of implant design features.
Primary implant stability is influenced by mechanical and biologic elements.
Secondary implant stability is also influenced by mechanical and biologic elements.