Pediatric Endodontics
Patient Management
Parent
Teammate
Decision maker…they are in your office
Emotional
Earn their trust!
Patient
#1 priority
Today’s problem
Surviving their parent
Lifelong oral health
Fear
Innate vs Acquired
objective vs subjective
DDS
Positive
Boss
Arbitrator
Grace (but win)
You have a job to do
No one is there to help you…without rules
Parent can stay if … dentist is in charge, child talks first, ask me to come in the hall for any discussion
Child needs to…open, listen, accept discomfort, know there are steps and when we’ll be done
Child rewards…parent can stay if, watch tv after, ipods during
Dentist need to…listen, be reasonable, organized/focused, have a minimal and ultimate goal
Win can mean ANY success…including a next appt!
Experience
Meet as a group
Pull parent aside
Assistant aide
Goals
Types of teeth in children
Primary teeth
immature permanent teeth (open apices)
Mature permanent teeth
Endodontic Differences
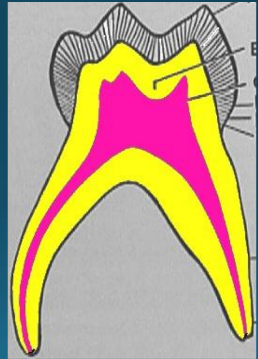
1. Anatomic Differences
Pulp Size: primary comparatively larger
Pulp horns: primary horns are higher
Pulp chamber: primary comparatively larger, accessory canals in floor lead directly into furcation
Roots: primary flare out more, comparatively narrower, thinner, and longer
Root canals: primary more ribbon-like
Resorption: physiologic resorption depending on age
Apical foramen: primary larger =>more complex anatomy
Nerve supply: primary less dense
2. Diagnostic Criteria for Primary Teeth
Swelling
History of pain
Duration
Frequency
Local vs Diffuse
Radiographic examination
Periradicular and furcation areas
Canal space
PDL space
Percussion most reliable
Cold test minimally reliable
EPT not reliable
Mobility (infection/resorption)
Radiographs
3. Treatment Options for Primary Teeth
Indirect pulp cap
key: asymptomatic
Selective caries removal…affected vs infected
Goal: don’t expose pulp
Calcium hydroxide on affected dentin
Ultrablend
“Permanently” restore (no second access to assess caries)
Direct pulp capping
6 months or less til exfoliation
Mechanical exposure only
Debate is extraction vs space maintenance
Contraindication: Swelling or symptoms
Pulpotomy
pulp exposure but vital with minimal symptoms
carious exposure imminent
process
Carious exposure, All caries removed, Coronal pulp removed with bur, Bleeding controlled with water/cotton pellet, Fill chamber floor with MTA, Cover MTA with flowable or Paracore, Stainless steel crown
Pulpectomy/RCT
irreversibly inflamed or necrotic pulp
Process
Carious exposure, All caries removed, Coronal pulp removed with bur, Bleeding controlled with water/cotton pellet, Fill chamber floor with MTA, Cover MTA with flowable or Paracore, Stainless steel crown
Focus of Treatment
Pt comfort
Space Maintenance
Lack of infection
Compromised: Keep options open
3. Treatments for Immature Permanent Teeth
Key: Err on the side of keeping the pulp alive
Apical closure
Apical closure on permanent teeth will occur approximately 3 years after eruption
For example eruption of a second molar happens at about12 years old but apical closure will not happen until patient is 15
Problem: Open Apices
Routine RCT cannot be performed
Weaker tooth
No Apical Stop
Can result in gross overfilling and/or poor apical seal, or fracture
Treatment options:
Pulpotomy (Vital Pulp Therapy)- reversible pulpitis, carious pulp exposure, vital and can control pulpal hemorrhage
Indications—Immature permanent teeth
Normal pulp to Reversible pulpitis
Traumatic exposure
Carious pulp exposure
Contraindication
Avulsed or severely luxated
Requires post/core
Non-restorable
Irreversible pulpitis or Necrotic pulps
Horizontal root fracture in cervical 1/3
Open Apex, Vital Pulp Process
Remove all caries
Remove pulp in chamber: High speed diamond bur for cauterization
Disinfect with NaOCl then sterile water
Hemostasis (damp cotton pellet, light pressure)
Place 3mm MTA plug/barrier
Definitive restoration or damp cotton pellet and temporize
Instant apexification – irreversibly inflamed, uncontrollable pulpal bleeding or necrotic pulp
Indications
Immature permanent with irreversible pulpitis or necrotic pulp
0.7 -1.5 mm
Contraindications
Very short roots
Root fractures
Replacement resorption (ankylosis)
Problems: susceptibility to fracture for immature teeth (thin dentin walls of roots)
Open Apex, Necrotic Pulp Process
“Instant” Apexification
1 appt vs 2 appt (today vs 2-4 weeks)
MTA apical barrier
Consider Matrix (CollaTape/CollaPlug)
4 mm thick
4-6 hours to set
GP backfill with gutta gun/flowable
Composite Restoration
Pulp regeneration - necrotic pulp in younger patient with wide open apex
Indications
Pulpal necrosis
Large open the apex
Compliant patient and family
Contraindications
Case selection…compliance, age, time, resorption, fracture
Non-compliant patient and family
Medical compromise…prone to infection, bleeding
Large Open Apex, Necrotic Pulp Process
Access and measure canal length
Rinse with NaOCl, minimal instrumentation
Medicate for 2-4 weeks
Triple antibiotic paste orCalcium Hydroxide
Rinse NaOCl, minimal instrumentation
Stimulate bleeding – revascularization induction
Scaffold, growth factors, cells
MTA
Glass Ionmer
Restore
Follow regularly
Focus
Realistic Expectations
Infection, lack of tooth structure, age of pt are all negatives for long term success
Diagnose properly
Pick right treatment
Hope for the best, plan for…
Open Apex
Also referred to as blunderbuss apex
Pulpal Necrosis
If the pulp undergoes necrosis before root growth is complete, dentin formation ceases and root growth is arrested
The canal and the apex will be very wide
The lateral dentin walls will be very thin
Other Etiology for open apex
Apical Resorption after orthodontic treatment
Inflammatory apical resorption
Choices for treatment of open apex
IT IS IMPERATIVE TO ESTABLISH IF PULP IS VITAL OR NOT!
Vital Pulp Therapy
Apexogenesis = Vital Pulp Therapy
The maintenance of pulp vitality to allow continued development of the root and for apical closure to occur
Treatment Techniques
Pulp cap
Calcium hydroxide or MTA
Pulpotomy
Calcium hydroxide or MTA
Remember
Vital, normal pulp or reversible pulpitis only
Partial Pulpotomy
Also known as Cvek pulpotomy
Used for large carious lesions
Pulp has to be vital
Remove caries (do not worry if pulp is exposed)
Remove exposed pulp with bur
Place MTA
Pulp Remains Vital
Root development continues
Apex will close
Canals get smaller
Follow-up
Recall every 3 to 6months
Signs of success
The pulp remains vital
No symptoms: no pain, swelling, sinus tracts, radiolucency etc.
Continued growth of the root and narrowing of the canal, indicating formation of dentin
Apexification with calcium hydroxide
Apexification = Root-End Closure
The process of creating an environment within the root canal and periapical tissues after pulpal necrosis that allows a calcified barrier(dentin/cementum/ bone/osteo-dentin) to form across the open apex
Treatment technique
Working length short of apex
Thorough instrumentation with gentle circumferential filing
Dry RCS
CaOH mixed with saline or local anesthetic packed into RCS
Place permanent fill
Follow-Up
Initial recall at 4-6 weeks take x-ray
Make sure Ca(OH)2 did not dissolve if it did it needs to be replaced
Next recall is at 3-6 months take x-ray replace Ca(OH)2only if it appears “washed out”
Recall in another six months if there is evidence of an apical barrier remove Ca(OH)2 and obturate with guuta-percha
Signs of Success
No signs or symptoms
Presence of a calcific barrier across the apex verified by x-rays or careful tactile probing with a hand file
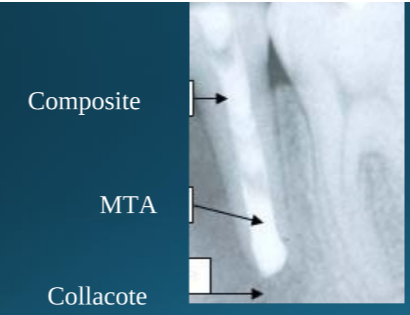
Apical Barrier with MTA
MTA on apical 1/3
Reschedule (MTA has to set)
Fill rest of canal with gutta-percha (Thermoplastisized Gutta-percha good here
Bonded composite in access and coronal 1/3 of canal (Tohelp prevent root fracture)
Can use resorbable collagen barrier such as Collacote (to prevent MTA extrusion)
Solves compliance problem
Signs of success
No signs or symptoms
MTA barrier remains intact
No evidence of resorption
Pulp Revascularization
What is the advantage?
If pulp can be reestablished dentin formation will continue and will have thicker dentin walls
This reduces the likelihood of fractures
Also research shows that calcium hydroxide will weaken dentin
Radiographic Assessment
Proximity of carious lesion to pulp
Calcific degeneration (reparative dentin, denticles)
Periodontal membrane: widening; loss of continuity
Periapical pathology + Root resorption
Internal / External resorption
Inter-radicular pathology
Vital Pulp Therapy
Treatment Objectives:
Eradicate potential for infection
Maintain tooth in a healthy state
Preserve “natural tooth” for space maintenance
Capitalize on reparative ability of pulp
Determine importance of radiographic vs. clinical signs
Indirect Pulp Treatment (IPT)
Indications:
Tooth with deep carious lesion
Incomplete caries removal
No pulp exposure
Permanent teeth only!
Controversial in primary teeth
Direct Pulp Capping Primary Teeth
Indications
Mechanical exposures only
Very small exposure
Only when tooth is ready to exfoliate
Contraindications
Toothaches
Spontaneous pain
Tooth mobility
Thickening of the PDL or lesion
Hemorrhage not easily controlled with dry cotton pellet
Purulent or serous exudate at exposure
Large exposure-->1.0mm
Carious exposures
Radiolucency
Treatment
ZOE cap or MTA
Base
Restore tooth
Pulpotomy Primary Teeth
Indications
Reversible to early irreversible symptoms
Large carious exposure
Tooth restorable
Minimal mobility and resorption
Contra indications
Irreversible or necrotic pulp
Loose with resorption
Not restorable
Root canal Treatment for Primary Teeth
Indications
Irreversible pulpitis
Pulpal necrosis (partial or total)
Minimum of root resorption and/or bony destruction in the bifurcation
Can have some swelling
Sinus tract
Restorable
Contraindications
Non-restorable
Periradicular involvement extending to 2°
Pathological resorption of at least 1/3 of root
Excessive internal resorption
Chamber floor opening into furcation
First primary molars usually extracted
Treatment
Working length
Clean and shape RCS gently— Be careful not to go too big
Fill canals with non-reinforced ZOE (fill needs to be resorbed along with root)
Fill chamber with reinforced ZOE (IRM)
Stainless steel crown