Lesson 7: RAAS
Lesson 7: Renin-Angiotensin-Aldosterone System (RAAS)
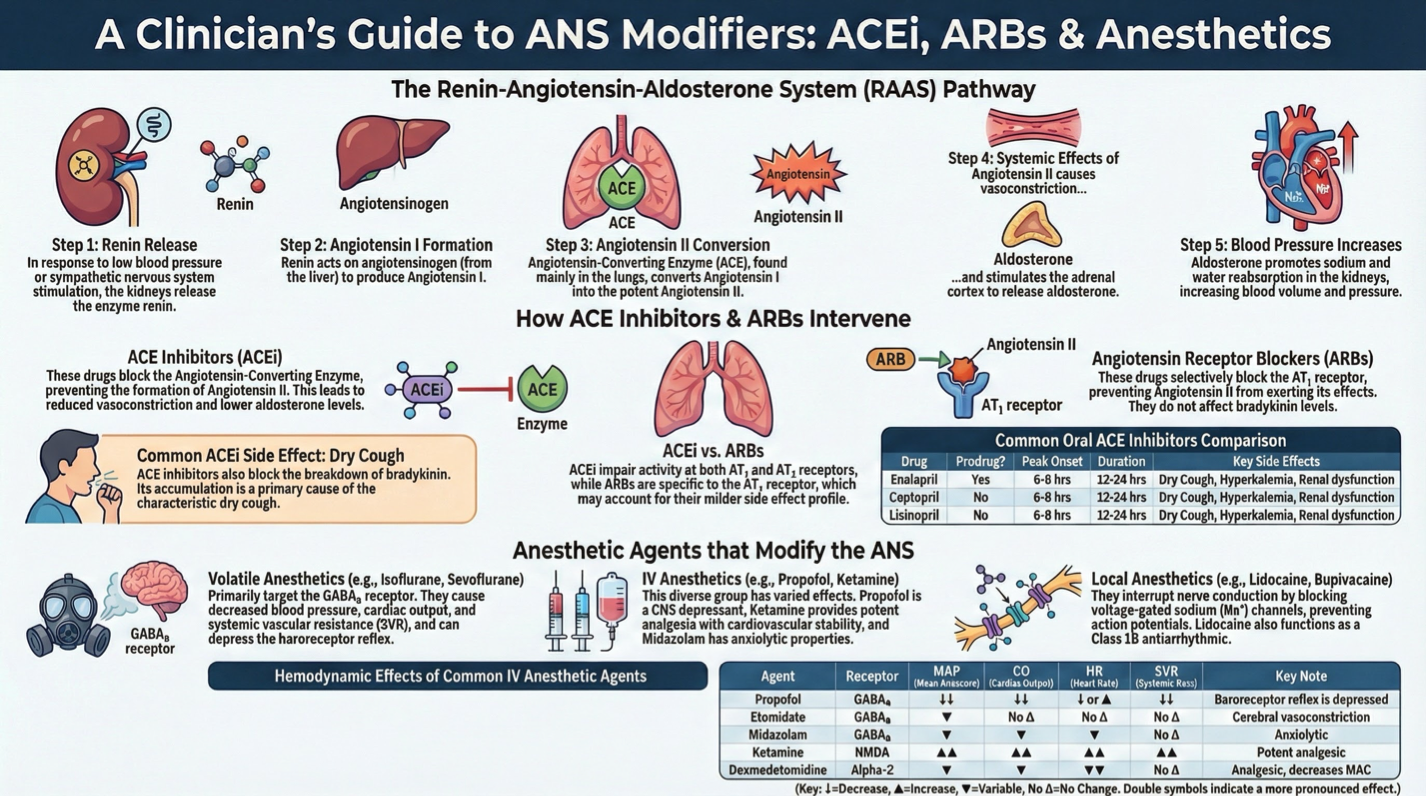
Essential for cardiovascular homeostasis
ACE inhibitors (ACEi) and Angiotensin Receptor Blockers (ARBs) manage hypertension
Modulation of the Autonomic Nervous System (ANS) by Anesthetic Agents
Isoflurane, sevoflurane, desflurane modify ANS affecting consciousness and immobility
Propofol is the most common IV induction drug, has CNS, respiratory, and cardiovascular depressant effects
Ketamine, etomidate, midazolam: careful use to avoid side effects
ACE Inhibitors
Widely prescribed for hypertension, CHF, and LV dysfunction
Main effects:
Decrease angiotensin generation
Lower left ventricular afterload
Fall in plasma aldosterone levels
Increased bradykinin levels cause dry cough
Risk of angioedema
Profound hypotension risk during anesthesia
Angiotensin Receptor Blockers (ARBs)
Selective for AT1 receptors, generally fewer side effects than ACE inhibitors
Similar effectiveness to ACEis for blood pressure moderation and heart failure
Provide renal protection without the side effect of dry cough
Volatile Anesthetic Agents
Enhance GABA function, depressive effects on CNS
Common effects:
Decreased BP, CO, CI, SVR
Myocardial depression and vasodilation
Impacts on respiratory drive and cerebral blood flow regulation
IV Anesthetic Agents
Propofol: reduces BP, causes bronchodilation, potential hemodynamic instability
Etomidate: cerebral vasoconstriction, minimal cardiovascular changes
Ketamine: good cardiovascular stability, analgesic properties, possible side effects like hallucinations
Midazolam: depresses airway reflexes, reduces BP and SVR
Local Anesthetics
Interrupt conduction of electrical impulses, provide anesthesia
Bind to Na+ channels, halting action potential propagation
Key agents: Lidocaine (Class 1B antiarrhythmic), bupivacaine, ropivacaine
Unique properties of cocaine: enhances endothelin, inhibits nitric oxide production