AP2 Lymphatic and Immune System
A&P 2 Class Work 4 Anatomy of the Lymphatic and Immune Systems
Anatomy of the Lymphatic and Immune Systems |
The immune system is the complex collection of cells and organs that destroys or neutralizes pathogens that would otherwise cause disease or death. The lymphatic system, for most people, is associated with the immune system to such a degree that the two systems are virtually indistinguishable.
The lymphatic system is the system of vessels, cells, and organs that
- carries excess fluids to the bloodstream and
- filters pathogens from the blood.
The swelling of lymph nodes during an infection and the transport of lymphocytes via the lymphatic vessels are but two examples of the many connections between these critical organ systems.
Functions of the Lymphatic System
A major function of the lymphatic system is to drain body fluids and return them to the bloodstream. It drains the excess fluid and empties it back into the bloodstream via a series of vessels, trunks, and ducts.
Lymph is the term used to describe interstitial fluid once it has entered the lymphatic system.
A lymph node is one of the small, bean-shaped organs located throughout the lymphatic system.
Cells of the immune system not only use lymphatic vessels to make their way from interstitial spaces back into the circulation, but they also use lymph nodes as major staging areas for the development of critical immune responses.
Structure of the Lymphatic System
The lymphatic vessels begin as a blind ending or closed at one end capillaries, which feed into larger and larger lymphatic vessels, and eventually empty into the bloodstream by a series of ducts. Along the way, the lymph travels through the lymph nodes, which are commonly found near the
- groin,
- armpits,
- neck,
- chest, and
- abdomen.
The lymphatic system in humans is forced through the vessels by
- the movements of the body,
- the contraction of skeletal muscles during body movements, and
- breathing.
One-way valves (semi-lunar valves) in lymphatic vessels keep the lymph moving toward the heart. Lymph flows from the lymphatic capillaries, through lymphatic vessels, and then is dumped into the circulatory system via the lymphatic ducts located at the junction of the jugular and subclavian veins in the neck.
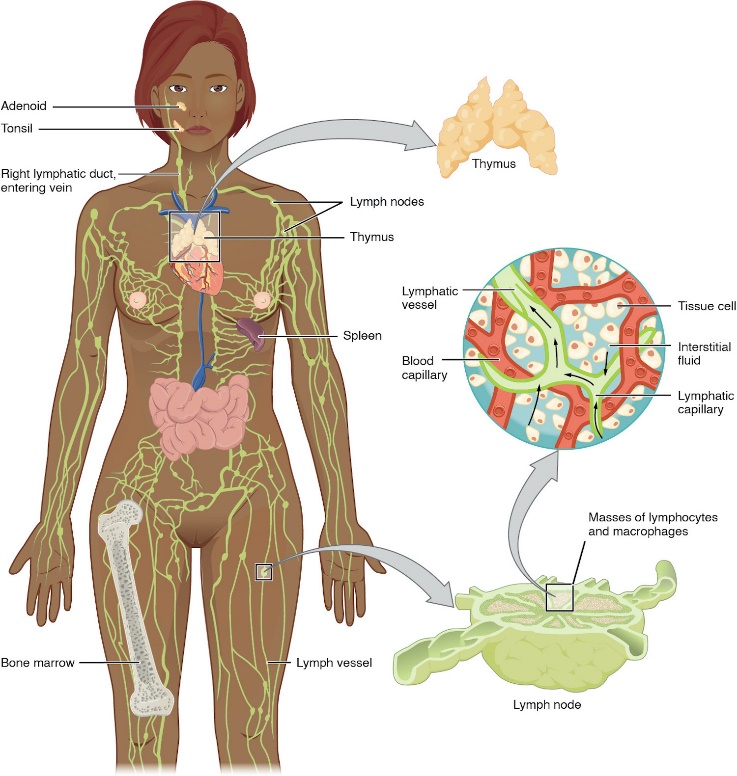
Figure: Anatomy of the Lymphatic System Lymphatic vessels in the arms and legs convey lymph to the larger lymphatic vessels in the torso.
Lymphatic Capillaries:
They are also called the terminal lymphatics, are vessels where interstitial fluid enters the lymphatic system to become lymph fluid. Located in almost every tissue in the body, these vessels are interlaced among the arterioles and venules of the circulatory system in the soft connective tissues of the body.
Exceptions which do not contain lymph vessels are the
central nervous system (CNS)
bone marrow,
bones,
teeth, and the
cornea of the eye.
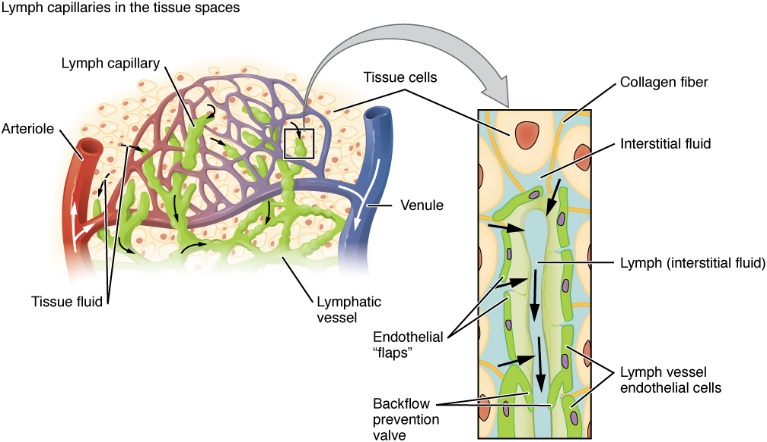
Figure: Lymphatic Capillaries Lymphatic capillaries are interlaced with the arterioles and venules of the cardiovascular system. Collagen fibers anchor a lymphatic capillary in the tissue (inset). Interstitial fluid slips through spaces between the overlapping endothelial cells that compose the lymphatic capillary.
Larger Lymphatic Vessels, Trunks, and Ducts
The lymphatic capillaries empty into larger lymphatic vessels. These one-way valves are located fairly close to one another, and each one causes a bulge in the lymphatic vessel, giving the vessels a beaded appearance.
The superficial and deep lymphatics eventually merge to form larger lymphatic vessels known as lymphatic trunks.
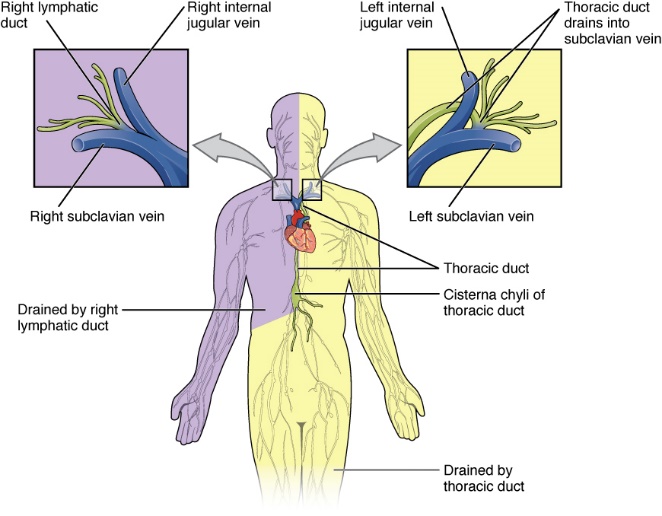
Figure: Major Trunks and Ducts of the Lymphatic System
The thoracic duct drains a much larger portion of the body than does the right lymphatic duct.
The Organization of Immune Function
The immune system is a collection of barriers, cells, and soluble proteins that interact and communicate with each other in extraordinarily complex ways. The modern model of immune function is organized into three phases based on the timing of their effects.
- 3 phases according to time.
The three temporal phases consist of the following:
- 1. Barrier defenses such as the skin and mucous membranes, which act instantaneously to prevent pathogenic invasion into the body tissues.
- Skin and mucous membranes – anything that is exposed to the outside world. Mouth, nose, throat, genetialia.
- 2. The rapid but nonspecific innate immune response, which consists of a variety of specialized cells and soluble factors.
- 3. The slower but more specific and effective adaptive immune response, which involves many cell types and soluble factors, but is primarily controlled by white blood cells (leukocytes) known as lymphocytes, which help control immune responses.
- From Lab - The first line of defense includes physical barriers such as the skin and mucous membranes. The second line of defense includes fever, the inflammatory response, phagocytosis, and a set of more than 20 proteins known as the complement system. The third line of defense is specific, meaning that certain immune system cells are proteins recognize and respond to only one pathogen.
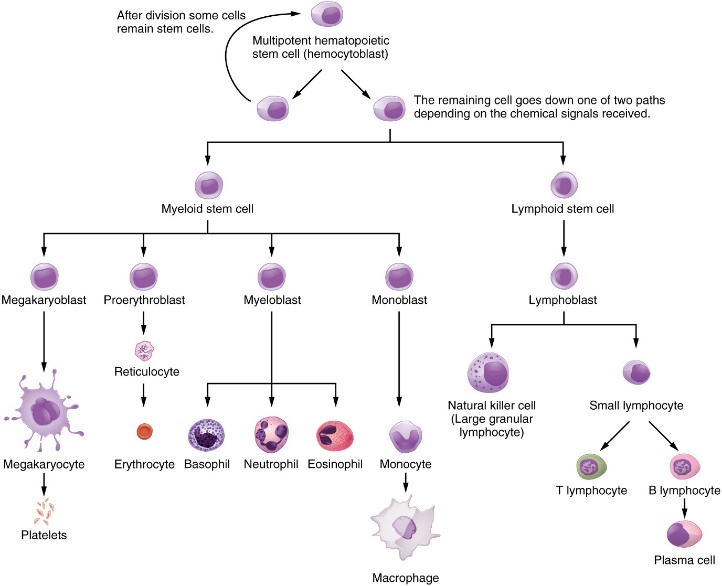
Figure: Hematopoietic System of the Bone Marrow All the cells of the immune response as well as of the blood arise by differentiation from hematopoietic stem cells. Platelets are cell fragments involved in the clotting of blood.
Lymphocytes: B Cells, T Cells, Plasma Cells, and Natural Killer Cells
As stated above, lymphocytes are the primary cells of adaptive immune responses.
The two basic types of lymphocytes, B cells and T cells:
are identical morphologically with a large central nucleus surrounded by a thin layer of cytoplasm.
are distinguished from each other by their surface protein markers as well as by the molecules they secrete.
B cells and T cells are found in many parts of the body, circulating in the bloodstream and lymph, and residing in secondary lymphoid organs, including the spleen and lymph nodes.
B Cells are immune cells that function primarily by producing antibodies.
- B Lymphocytes, when needed, will give rise to plasma cells.
T Cells do not secrete antibody but performs a variety of functions in the adaptive immune response. Different T cell types have the ability to either secrete soluble factors that communicate with other cells of the adaptive immune response or destroy cells infected with intracellular pathogens.
Plasma Cells are B cells that have differentiated in response to antigen binding and have thereby gained the ability to secrete soluble antibodies. These cells differ in morphology from standard B and T cells in that they contain a large amount of cytoplasm packed with the protein-synthesizing machinery known as rough endoplasmic reticulum.
Natural Killer Cells are important lymphocytes and participant in the innate immune response. A natural killer cell (NK) is a circulating blood cell that contains cytotoxic (cell-killing) granules in its extensive cytoplasm. It shares this mechanism with the cytotoxic T cells of the adaptive immune response. NK cells are among the body’s first lines of defense against viruses and certain types of cancer.
- Rough ER is a Cell Membrane Factory. The vesicles that come off of the rough er, fuse with the cell membrane.
Lymphocytes
Type of lymphocyte | Primary function |
|---|---|
B lymphocyte | Generates diverse antibodies |
T lymphocyte | Secretes chemical messengers |
Plasma cell | Secretes antibodies |
NK cell | Destroys virally infected cells |
Primary Lymphoid Organs and Lymphocyte Development
And
Secondary Lymphoid Organs and their Roles in Active Immune Responses
Primary Lymphoid organs – Bone Marrow and Thymus
Secondary Lymphoid organs – Spleen, lymphatic vessels, lymph nodes, adenoids and tonsils, MALT (Mucosal associated lymphoid Tissue) – Galt, Balt, Salt, Nalt.
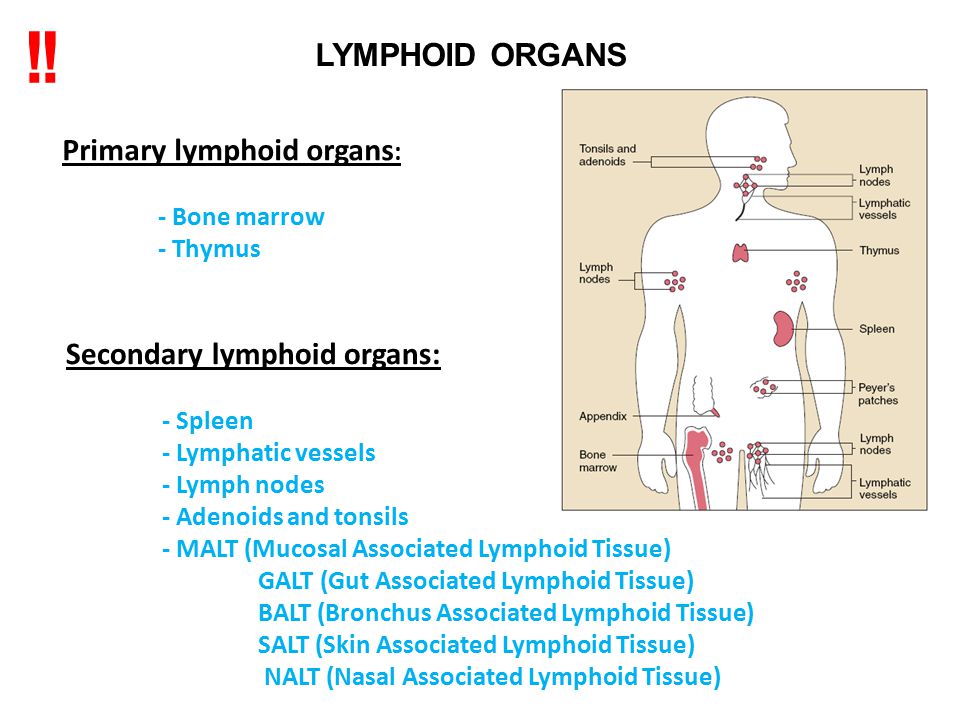
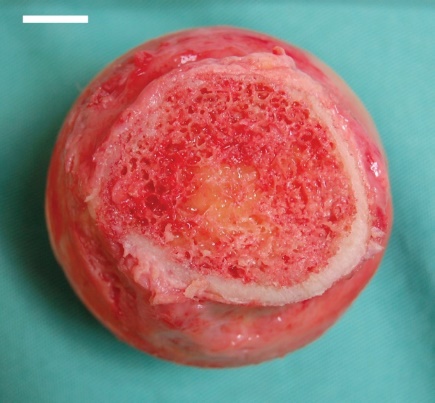
Figure: Bone Marrow Red bone marrow fills the head of the femur, and a spot of yellow bone marrow is visible in the center. The white reference bar is 1 cm.
- Bone marrow is Loose collection of cells where hematopoiesis occurs. Yellow bone marrow is site of energy storage and fat cells.
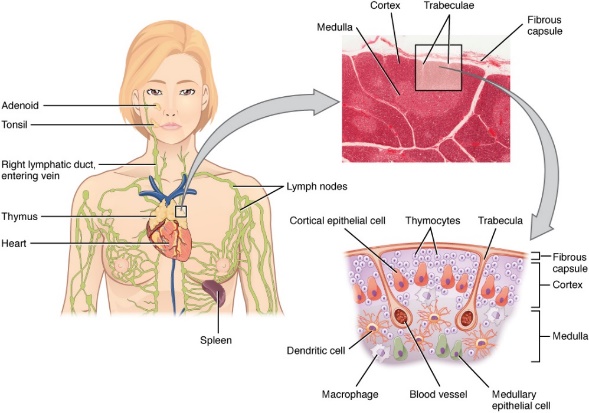
Figure: Location, Structure, and Histology of the Thymus
The thymus lies above the heart. The trabeculae and lobules, including the darkly staining cortex and the lighter staining medulla of each lobule, are clearly visible in the light micrograph of the thymus of a newborn.
- Bilobed organ found in the space between the sternum and the aorta of the heart.
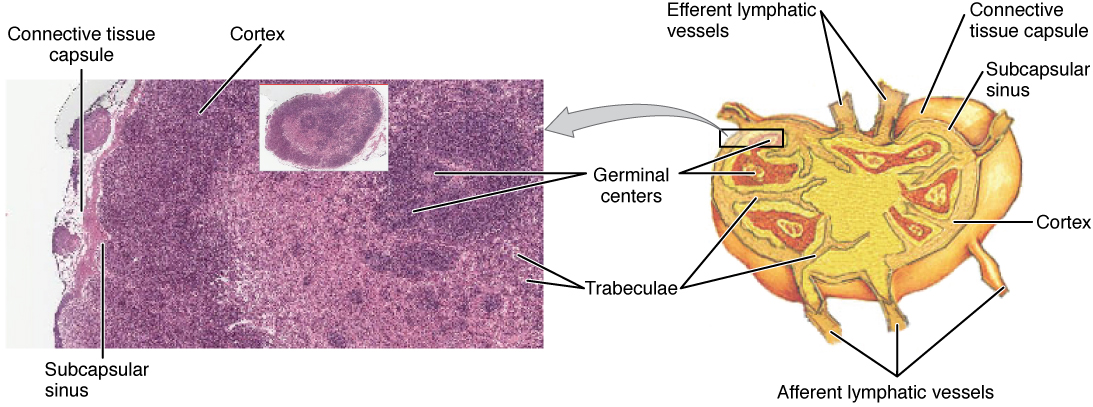
Figure: Structure and Histology of a Lymph Node Lymph nodes are masses of lymphatic tissue located along the larger lymph vessels. The micrograph of the lymph nodes shows a germinal center, which consists of rapidly dividing B cells surrounded by a layer of T cells and other accessory cells. 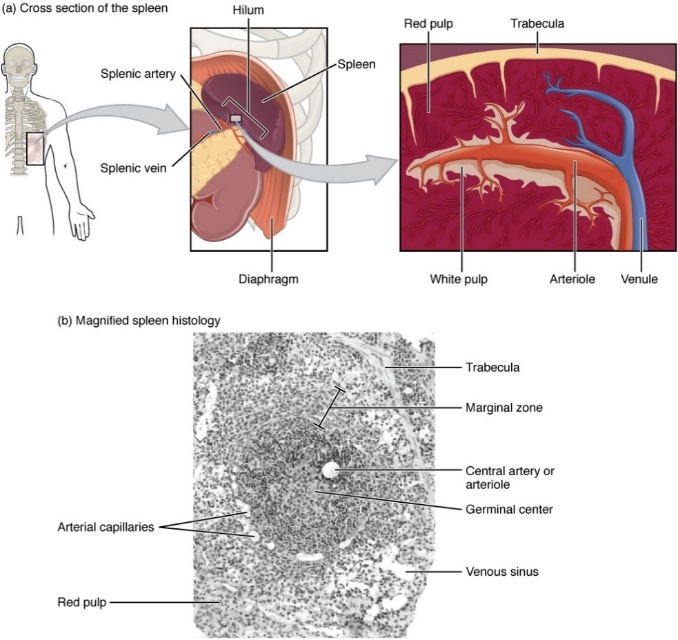
Figure: Spleen
- The spleen is attached to the stomach.
- A micrograph of spleen tissue shows the germinal center. The marginal zone is the region between the red pulp and white pulp, which sequesters particulate antigens from the circulation and presents these antigens to lymphocytes in the white pulp.
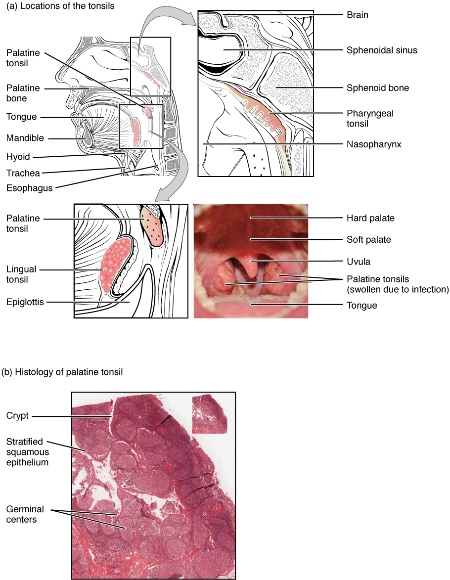
Figure: Locations and Histology of the Tonsils
- The pharyngeal tonsil is located on the roof of the posterior superior wall of the nasopharynx. The palatine tonsils lay on each side of the pharynx.
- A micrograph shows the palatine tonsil tissue.
Barrier Defenses and the Innate Immune Response |
The immune system can be divided into two overlapping mechanisms to destroy pathogens:
the innate immune response, which is relatively rapid but nonspecific and thus not always effective, and
the adaptive immune response, which is slower in its development during an initial infection with a pathogen, but is highly specific and effective at attacking a wide variety of pathogens
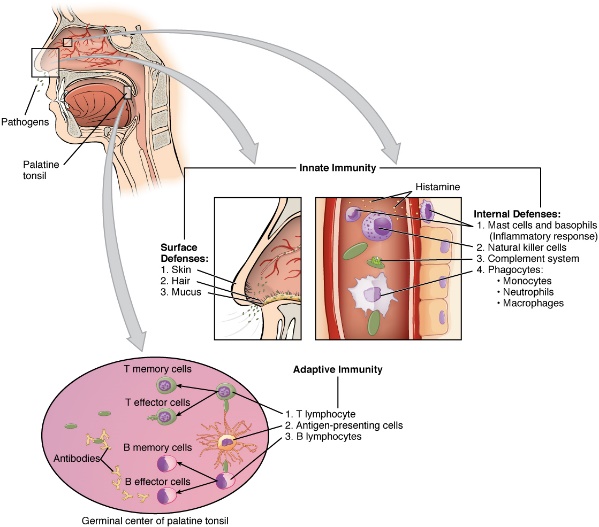
Figure: Cooperation between Innate and Adaptive Immune Responses The innate immune system enhances adaptive immune responses so they can be more effective.
The Innate immune response: First Line of Defense
Any discussion of the innate immune response usually
begins with the physical barriers that prevent pathogens from entering the body, destroy them after they enter, or flush them out before they can establish themselves in the hospitable environment of the body’s soft tissues.
Barrier defenses are part of the body’s most basic defense mechanisms. The barrier defenses are not a response to infections, but they are continuously working to protect against a broad range of pathogens.
Barrier Defenses
Site | Specific defense | Protective aspect |
|---|---|---|
Skin | Epidermal surface | Keratinized cells of surface, Langerhans cells |
Skin (sweat/secretions) | Sweat glands, sebaceous glands | Low pH, washing action |
Oral cavity | Salivary glands | Lysozyme |
Stomach | Gastrointestinal tract | Low pH |
Mucosal surfaces | Mucosal epithelium | Nonkeratinized epithelial cells |
Normal flora (nonpathogenic bacteria) | Mucosal tissues | Prevent pathogens from growing on mucosal surfaces |
Cells of the Innate Immune Response
A phagocyte is a cell that is able to surround and engulf a particle or cell, a process called phagocytosis. The phagocytes of the immune system engulf other particles or cells, either to clean an area of debris, old cells, or to kill pathogenic organisms such as bacteria. Phagocytes are the body’s fast acting, first line of immunological defense against organisms that have breached barrier defenses and have entered the vulnerable tissues of the body.
1 – Phagocytes: Macrophages and Neutrophils
Phagocytic Cells of the Innate Immune System
Cell | Cell type | Primary location | Function in the innate immune response |
|---|---|---|---|
Macrophage | Agranulocyte | Body cavities/organs | Phagocytosis |
Neutrophil | Granulocyte | Blood | Phagocytosis |
Monocyte | Agranulocyte | Blood | Precursor of macrophage/dendritic cell |
2 – Natural Killer Cells
NK cells are a type of lymphocyte that have the ability to induce apoptosis, that is, programmed cell death, in cells infected with intracellular pathogens such as obligate intracellular bacteria and viruses.
Recognition of Pathogens
Cells of the innate immune response, the phagocytic cells, and the cytotoxic NK cells recognize patterns of pathogen-specific molecules, such as bacterial cell wall components or bacterial flagellar proteins, using pattern recognition receptors. A pattern recognition receptor (PRR) is a membrane-bound receptor that recognizes characteristic features of a pathogen and molecules released by stressed or damaged cells.
Soluble Mediators of the Innate Immune Response
The chemical signals can induce cells to change various physiological characteristics, such as the expression of a particular receptor. These soluble factors are secreted:
- during innate or early induced responses, and
- later during adaptive immune responses.
Cytokines and Chemokines
A cytokine is signaling molecule that allows cells to communicate with each other over short distances. Cytokines are secreted into the intercellular space, and the action of the cytokine induces the receiving cell to change its physiology.
A chemokine is a soluble chemical mediator similar to cytokines except that its function is to attract cells (chemotaxis) from longer distances.
Early induced Proteins
Early induced proteins are those that are not constitutively present in the body but are made as they are needed early during the innate immune response.
Example: Interferons
Complement System
The complement system is a series of proteins constitutively found in blood plasma.
Inflammatory Response
The hallmark of the innate immune response is inflammation. It is important to note that inflammation does not have to be initiated by an infection but can also be caused by tissue injuries.
The inflammatory reaction brings in phagocytic cells to the damaged area
to clear cellular debris and
to set the stage for wound repair.
Inflammation is part of a very basic form of immune response. (Acute inflammation, Chronic inflammation).

There are four important parts to the inflammatory response:
- Tissue Injury. Release of mast cell granules. Release histamine initiating inflammatory response.
- Vasodilation. Histamine increases diameter of blood vessels, causing increased blood flow.
- Increased Vascular Permeability. Inflammatory mediators increase the permeability, causing leakage of fluid into interstitial space, swelling.
- Recruitment of Phagocytes. Macrophages recruited to clean up debris.
Overall, inflammation is valuable for many reasons. Not only are the pathogens killed and debris removed, but the increase in vascular permeability encourages the entry of clotting factors, the first step towards wound repair. Inflammation also facilitates the transport of antigen to lymph nodes by dendritic cells for the development of the adaptive immune response.
The Adaptive Immune Response:T lymphocytes and Their Functional Types |
Innate immune responses (and early induced responses) are in many cases ineffective at completely controlling pathogen growth. However, they slow pathogen growth and allow time for the adaptive immune response to strengthen and either control or eliminate the pathogen.
The innate immune system also sends signals to the cells of the adaptive immune system, guiding them in how to attack the pathogen. Thus, these are the two important arms of the immune response.
The Benefits of the Adaptive Immune Response
The specificity of the adaptive immune response (its ability to specifically recognize and make a response against a wide variety of pathogens) is its great strength. Antigens (the small chemical groups often associated with pathogens) are recognized by receptors on the surface of B and T lymphocytes. The adaptive immune response to these antigens is so versatile that it can respond to nearly any pathogen.
The primary adaptive response is the immune system’s first exposure to a pathogen. Symptoms of a first infection, called primary disease, are always relatively severe because it takes time for an initial adaptive immune response to a pathogen to become effective.
The secondary adaptive response is generated upon re-exposure to the same pathogen, which is stronger and faster than the primary response. This secondary response is the basis of immunological memory, which protects us from getting diseases repeatedly from the same pathogen.
Self Recognition: A third important feature of the adaptive immune response is its ability to distinguish between self-antigens (those that are normally present in the body) and foreign antigens (those that might be on a potential pathogen).
T Cell-Mediated Immune Responses
The primary cells that control the adaptive immune response are the lymphocytes, the T and B cells.
T cells are particularly important, as they not only control a multitude of immune responses directly, but also control B cell immune responses in many cases as well.
Thus, many of the decisions about how to attack a pathogen are made at the T cell level, and knowledge of their functional types is crucial to understanding the functioning and regulation of adaptive immune responses as a whole.
T lymphocytes recognize antigens based on a two-chain protein receptor. The most common and important of these are the alpha-beta T cell receptors.
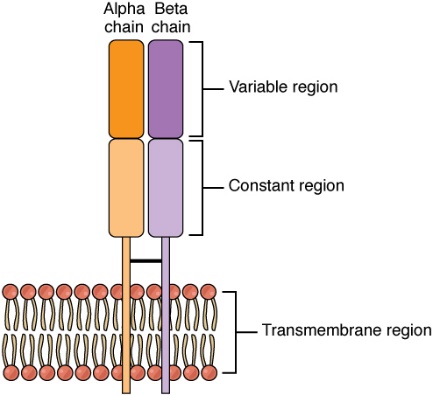
Figure: Alpha-beta T Cell Receptor Notice the constant and variable regions of each chain, anchored by the transmembrane region.
Antigens
Antigens on pathogens are usually large and complex and consist of many antigenic determinants.
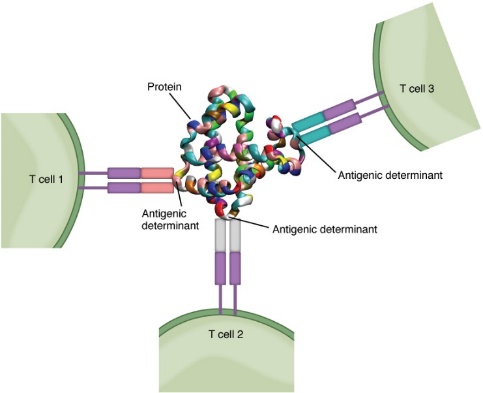
Figure: Antigenic Determinants
A typical protein antigen has multiple antigenic determinants, shown by the ability of T cells with three different specificities to bind to different parts of the same antigen.
Differentiation of T Cells within the Thymus:
Immature T-cells, called thymocytes, enter the thymus and go through a series of developmental stages that ensures both function and tolerance before they leave and become functional components of the adaptive immune response.
Mechanisms of T Cell-mediated Immune Responses
Clonal Selection and Expansion
Stem cells differentiate into T cells with specific receptors (To an antigen), called clones. Each clone is necessarily present in the body in low numbers. Otherwise, the body would not have room for lymphocytes with so many specificities.
T cell response to a typical antigen involves a polyclonal response. A polyclonal response is the stimulation of multiple T cell clones. Once activated, the selected clones increase in number and make many copies of each cell type, each clone with its unique receptor. By the time this process is complete, the body will have large numbers of specific lymphocytes available to fight the infection.
- Clone – Group of lymphocytes sharing the same antigen receptor.
- Clonal Anergy – Process whereby B cells that react to soluble antigens in bone marrow are made nonfunctional.
- Clonal deletion – Removal of self-reactive B cells by inducing apoptosis
- Clonal expansion – Growth of a clone of selected lymphocytes
- Clonal Selection – Stimulating growth of lymphocytes that have specific receptors.
- Polyclonal response – response by multiple clones to a complex antigen with many determinants.
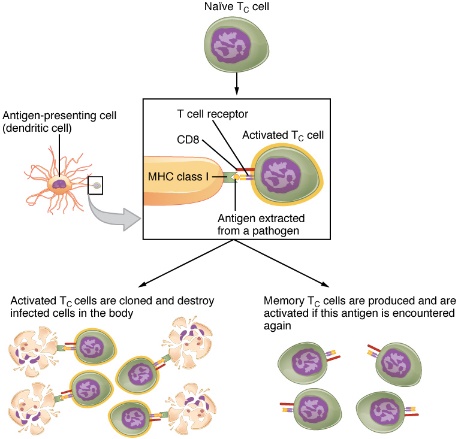
Figure: Clonal Selection and Expansion of T Lymphocytes
The Cellular Basis of Immunological Memory
As already discussed, one of the major features of an adaptive immune response is the development of immunological memory.
T Cell Types and their Functions
Helper T cells (Th), bearing the CD4 molecule, function by secreting cytokines that act to enhance other immune responses. There are two classes of Th cells, and they act on different components of the immune response. These cells are not distinguished by their surface molecules but by the characteristic set of cytokines they secrete.
Cytotoxic T cells (Tc) are T cells that kill target cells by inducing apoptosis using the same mechanism as NK cells.
Regulatory T cells (Treg), or suppressor T cells, are the most recently discovered of the types listed here, so less is understood about them.

Figure: Pathogen Presentation
- CD4 is associated with helper and regulatory T cells. An extracellular pathogen is processed and presented in the binding cleft of a class II MHC molecule, and this interaction is strengthened by the CD4 molecule.
- CD8 is associated with cytotoxic T cells. An intracellular pathogen is presented by a class I MHC molecule, and CD8 interacts with it.
MHC = Major Histocompatibility Complex
CD4 = Cluster of differentiation
The Adaptive Immune Response: B-lymphocytes and Antibodies |
Scientists now know the cause of the agglutination is an antibody molecule, also called an immunoglobulin. – Protein antibody, occurs as one of five main classes.
An antibody protein is essentially a secreted form of a B cell receptor. (In fact, surface immunoglobulin is another name for the B cell receptor.)
There are five different classes of antibody found in humans: IgM, IgD, IgG, IgA, and IgE (Remember DAMGE or GAMED). Each of these has specific functions in the immune response, B cells do not recognize antigen in the complex fashion of T cells.
Antibody Structure
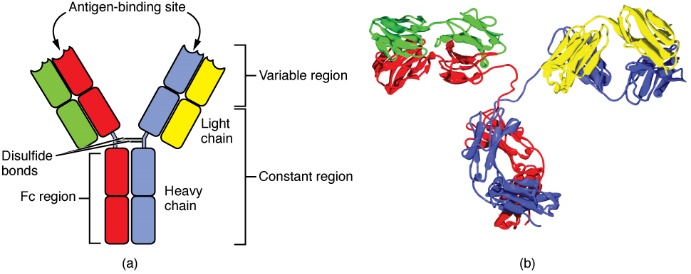
Figure: Antibody and IgG2 Structures
(a) The typical four chain structure of a generic antibody
(b) and the corresponding three-dimensional structure of the antibody IgG2 (b).
- Heavy chains are the ones in the middle that are connected, the light chains are not connected to the FC region. Heavy chain – Larger protein chain of an antibody. Light chain – Small protein chain of an antibody.
- Constant region domain – Part of a lymphocyte antigen receptor that does not vary much between different receptor types.
- Variable region Domain – Part of a lymphocyte antigen receptor that varies considerably between different receptor types.
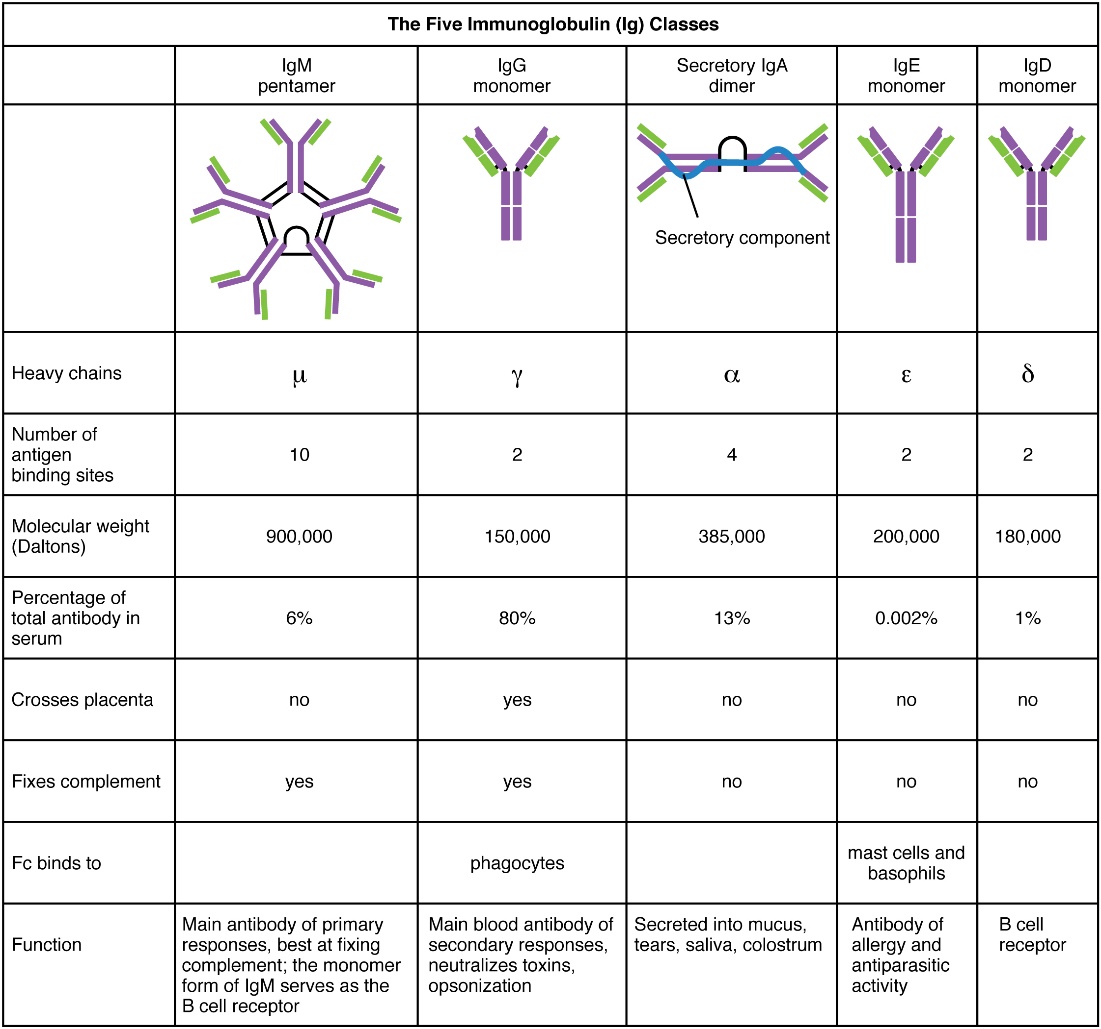
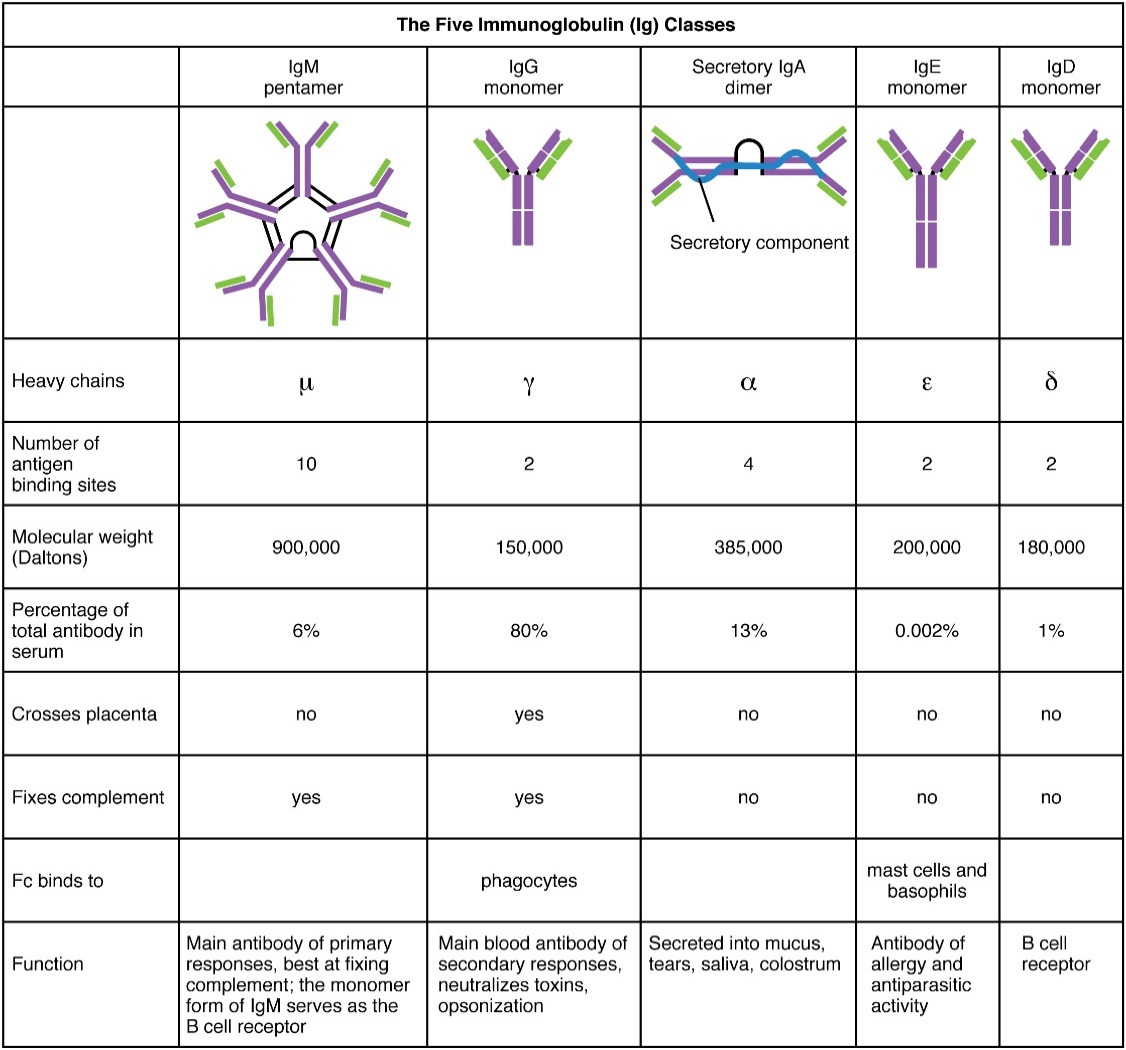
Figure: Five Classes of Antibodies
- Immunoglobulin M – when found in patient it means they are first exposed – Primary response. Antibody whose monomer is a surface receptor of naïve B cells.
- Immunoglobulin G – Main blood antibody of secondary response. If the patient has high IgG then it is not the first time they were exposed. Passed from carrier to unborn child via placenta
- Secretory IgA – Secreted into mucus, tears, saliva, colostrum – when you suspect an infection in one of the organs that contains these secretions, you are looking for IgA. Second most abundant immunoglobulin. Gastrointestinal, respiratory, genitourinary tracts. Especially affective against digestive and respiratory pathogens, and can pass immunity to an infant through breastfeeding.
- IgE – Antibody of allergy and antiparasitic activity – If patient has very high IgE check if there is an allergic situation, or exposed to a parasite.
- IgD – B Cell receptor – Signals for B cells to be activated in order for them to participate in the immune defense. Apparently, IgM and IgD share this role, IgM does it fast, and IgD does it later.
Clonal Selection of B Cells
During a primary B cell immune response, both antibody-secreting plasma cells and memory B cells are produced. These memory cells lead to the differentiation of more plasma cells and memory B cells during secondary responses.
Primary versus Secondary B Cell Responses
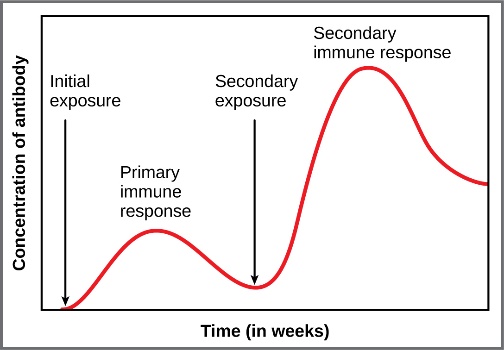
Figure: Primary and Secondary Antibody Responses Antigen A is given once to generate a primary response and later to generate a secondary response. When a different antigen is given for the first time, a new primary response is made.
**Active versus Passive Immunity
Active versus Passive Immunity
Natural | Artificial | |
|---|---|---|
Active | Adaptive immune response | Vaccine response |
Passive | Trans-placental antibodies/breastfeeding | Immune globulin injections |
Active Natural = Adaptative immune response (relatively slow but very specific and effective immune response controlled by lymphocytes.
Active Artificial = Vaccine response
Passive Natural =
Passive Artificial = Just give what will treat the problem – immune globulin injections.
Diseases Associated with Depressed or Overactive Immune Responses |
Immunodeficiencies
A – Inherited immunodeficiencies arise from gene mutations that affect specific components of the immune response.
The most serious of the inherited immunodeficiencies is severe combined immunodeficiency disease (SCID). This disease is complex because it is caused by many different genetic defects. What groups them together is the fact that both the B cell and T cell arms of the adaptive immune response are affected. SCID – Genetic mutation that affects both T cell and B cell arms of the immune response.
B – There are also acquired immunodeficiencies with potentially devastating effects on the immune system, such as HIV.
Hypersensitivities
The word “hypersensitivity” simply means sensitive beyond normal levels of activation. Allergies and inflammatory responses to nonpathogenic environmental substances have been observed since the dawn of history. Hypersensitivity is a medical term describing symptoms that are now known to be caused by unrelated mechanisms of immunity. Still, it is useful for this discussion to use the four types of hypersensitivities as a guide to understand these mechanisms.
Immune Hypersensitivity: Components of the immune system cause four types of hypersensitivity. Notice that types I–III are B cell mediated, whereas type IV hypersensitivity is exclusively a T cell phenomenon.
IgE – Mediated Hypersensitivity: causes localized and systemic anaphylaxis (a severe, life-threatening allergic reaction), seasonal allergies including hay fever, food allergies, such as those to shellfish and peanuts, hives, and eczema
IgG – Mediated Hypersensitivity: RBCs destroyed by complement and antibodies during a transfusion of mismatched blood type or during erythroblastosis fetalis.
Immune Complex – Mediated Hypersensitivity: Most common forms of immune complex disease are seen in:
glomerulonephritis,
Rheumatoid Arthritis, and
Systemic Lupus and erythematosus.
Cell Mediated – Mediated Hypersensitivity: Most common are contact dermatitis, Tuberculin reaction, autoimmune diseases such Diabetes type I, multiple sclerosis, and Rheumatoid Arthritis.
Autoimmune Responses
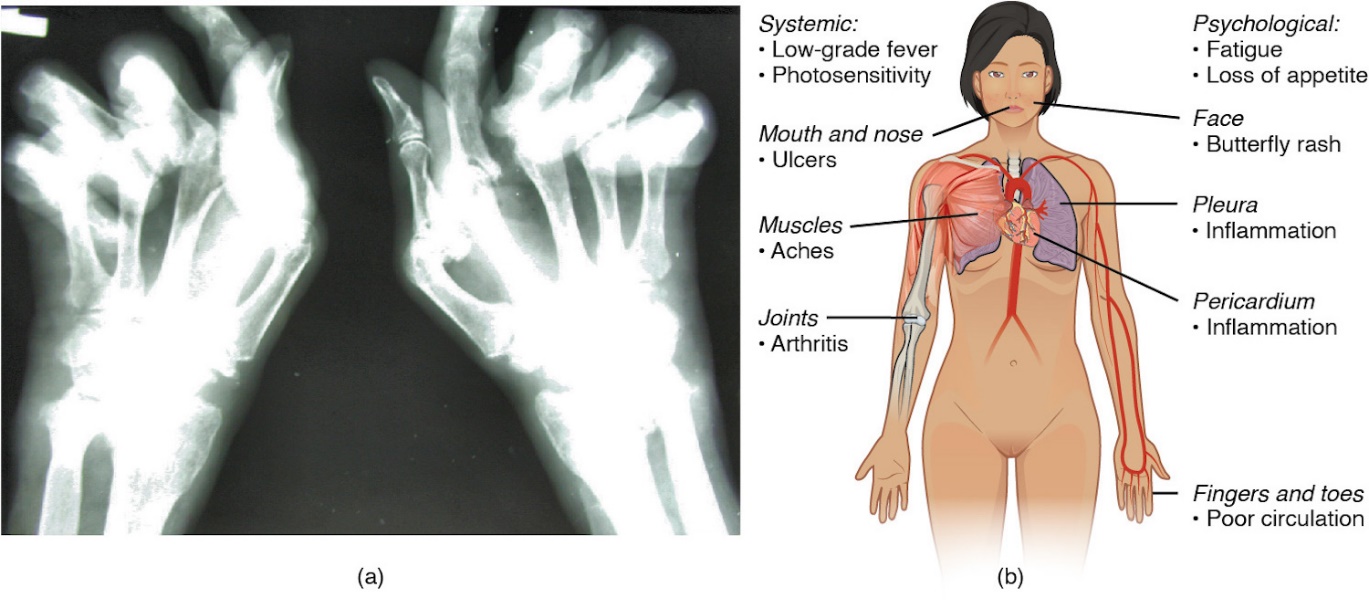
Figure: Autoimmune Disorders: Rheumatoid Arthritis and Lupus
(a) Extensive damage to the right hand of a rheumatoid arthritis sufferer is shown in the x-ray.
(b) The diagram shows a variety of possible symptoms of systemic lupus erythematosus.
Autoimmune Diseases
Disease | Autoantigen | Symptoms |
|---|---|---|
Celiac disease | Tissue transglutaminase | Damage to small intestine |
Diabetes mellitus type I | Beta cells of pancreas | Low insulin production; inability to regulate serum glucose |
Graves’ disease | Thyroid-stimulating hormone receptor (antibody blocks receptor) | Hyperthyroidism |
Hashimoto’s thyroiditis | Thyroid-stimulating hormone receptor (antibody mimics hormone and stimulates receptor) | Hypothyroidism |
Lupus erythematosus | Nuclear DNA and proteins | Damage of many body systems |
Myasthenia gravis | Acetylcholine receptor in neuromuscular junctions | Debilitating muscle weakness |
Rheumatoid arthritis | Joint capsule antigens | Chronic inflammation of joints |