Pupil Anomalies P2: Anisocoria and Horner's Syndrome
Anisocoria
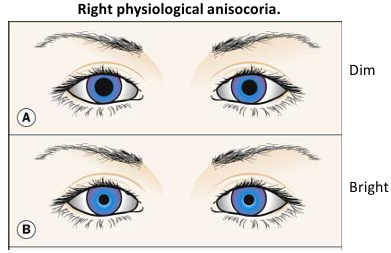
Physiological Anisocoria
20% of the population exhibits physiological anisocoria.
Characteristics:
Asymptomatic.
Direct, consensual, and near reflexes are similar in extent in each eye.
No ptosis and ocular movements are normal.
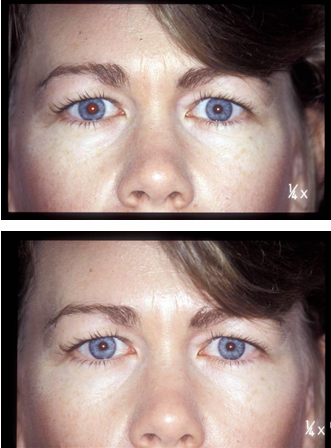
Relative difference in pupil size maintained under differing levels of illumination.
Pathological Anisocoria
Caused by lesions affecting sympathetic or parasympathetic pathways (efferent pathway) or local iris disease/trauma.
Afferent pathway lesions do not affect pupil size or produce anisocoria.
Evaluation:
Does the degree of anisocoria change with increasing or decreasing room illumination?
Look for evidence of: ptosis, motility defects, strabismus, heterophoria, head or eye injury.
Significance of Anisocoria
The significance lies in whether the anisocoria increases more in light or in dark conditions.
This difference helps determine which efferent pupillomotor pathway is affected.
Types of defects:
Parasympathetic pupillomotor defects: Anisocoria is greater in the light than in the dark.
iris sphincter is affected.
The larger pupil is the affected one (e.g., 3rd nerve palsy, Adie’s tonic pupil).
Sympathetic pupillomotor defects: Anisocoria is greater in the dark than in the light.
iris dilator is affected
The smaller pupil is the affected one (e.g., Horner’s syndrome).
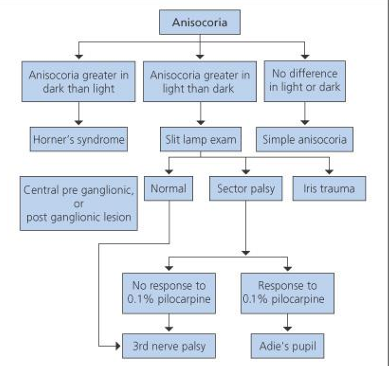
Clinical Checklist for Anisocoria
Anisocoria greater in the dark than in light:
Horner's syndrome
Central pre-ganglionic, Normal
Or post ganglionic lesion
Anisocoria greater in the light than in dark:
Slit lamp exam
Simple anisocoria
3rd nerve palsy
Adie's pupil
No difference in light or dark:
Sector palsy
Iris trauma
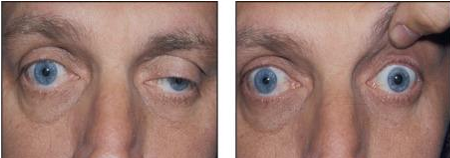
Parasympathetic Defects: 3rd Nerve Palsy
Anisocoria greater in light than dark.
Affected pupil is dilated and poorly reactive to light and near stimuli.
Presence of ipsilateral ptosis, motility disturbance, or both almost always signifies a partial third nerve palsy.
oculomotor nerve innervates the levator muscle, IR, IO, MR → px with 3rd nerve palsy only have LR and SO = eye to look out and down.
Internal ophthalmoplegia.
ciliary muscle is innovated by the third cranial nerve, so px will have trouble focussing , resulting in blurred vision and difficulty accommodating for near tasks.

Acute Onset 3rd Nerve Paralysis
May be associated with severe head pain.
Pupil dilated – suggestive of ANEURYSM.
Pupil spared – suggestive of ISCHAEMIA.
HOWEVER: Cause until proven otherwise must be assumed to be an aneurysm.
Patient must be referred as an emergency (need urgent imaging of brain)
Parasympathetic Defects: Adie’s Tonic Pupil
Caused by damage to the ciliary ganglion or post-ganglionic fibers to the iris sphincter.
A common cause of anisocoria.
Typically affects women in their 3rd to 4th decade.
May follow viral illness, sometimes idiopathic.
Occasionally inherited in an AD pattern.
Often associated with diminished or absent tendon reflexes of the lower limbs.
Unilateral in 80% of cases.
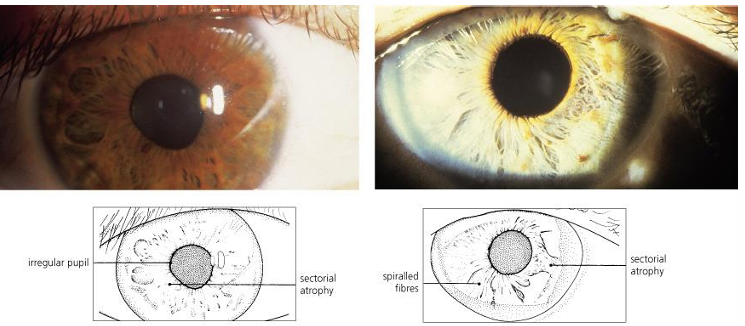
Clinical Presentation of Adie's Tonic Pupil
Pupil enlarged; anisocoria greatest in light.
Pupil slightly misshapen.
Reacts poorly to light.
Sector palsy of the sphincter, sector atrophy, spiraled iris fibers.
under the slit lamp only sections of the pupil respond to light.
May see sectorial reaction to light or vermiform (wormlike) movements of segments of the sphincter under slit lamp.
The pupil responds slowly (tonic) to near (sluggish constriction with prolonged stimulation), following which re-dilatation is also slow.
>30 secs or more needed for near work.
Accommodation may manifest similar tonicity, with slowed and impaired focusing for near and prolonged re-focusing in the distance.
Pharmacological Testing for Adie’s Tonic Pupil
Denervation super sensitivity is evident.
The iris sphincter becomes supersensitive to acetylcholine and similar substances (e.g., pilocarpine - parasympathomimetic).
Pharmacological testing: An Adie's pupil will constrict in response to 0.1% pilocarpine (a direct-acting parasympathomimetic drug). This concentration should not constrict a normal pupil.
45 minutes following instillation of 0.1% pilocarpine.

With time, the tonic pupil may eventually become miotic.
Paralysis of accommodation improves, but light tonicity worsens.
Adie’s tonic pupil is generally considered to be a benign condition.
not associated with any significant pathology.
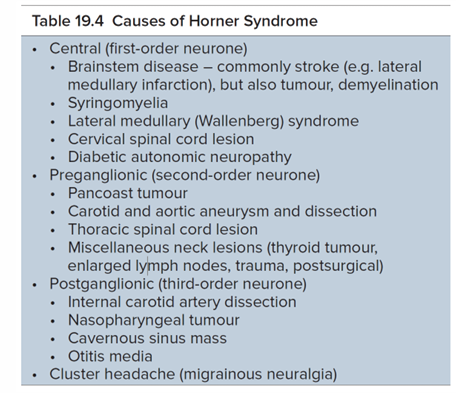
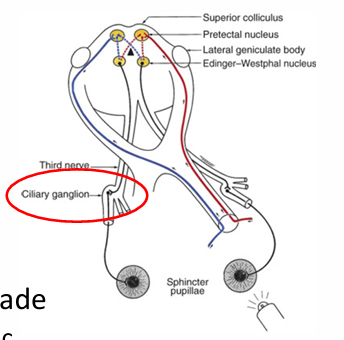
Sympathetic Defect: Horner’s Syndrome
Oculosympathetic palsy.
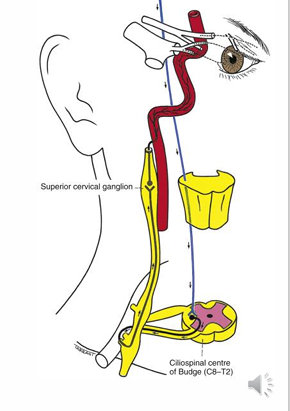
The sympathetic pathway is at 3 levels:
First-order neuron: posterior hypothalamus to brainstem to ciliospinal center.
stroke or problem in brainstem
Second-order neuron: from ciliospinal center to superior cervical ganglion, closely associated with the subclavian artery and apical pleura.
apical lung tumour or aneurysms of the arteries near the lungs
Third-order neuron: SCG along the internal carotid to join the ophthalmic division of the trigeminal nerve via the nasociliary and long ciliary nerves to the CB and dilator of the iris.
carotid artery disease or aneurysm of the internal carotid artery.
cavernous sinus disease.
Horner’s syndrome is caused by a partial or total interruption of this sympathetic chain.
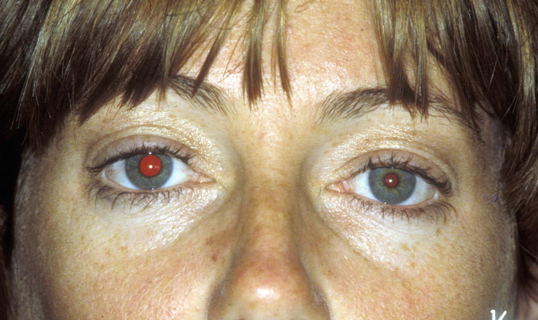
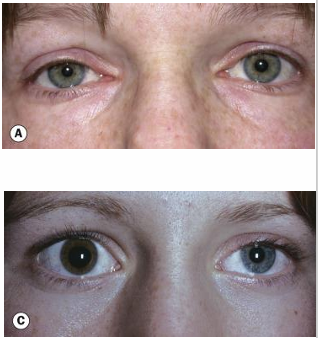
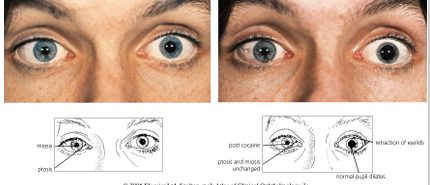
Characteristics of Horner’s Syndrome
Miosis of the affected eye.
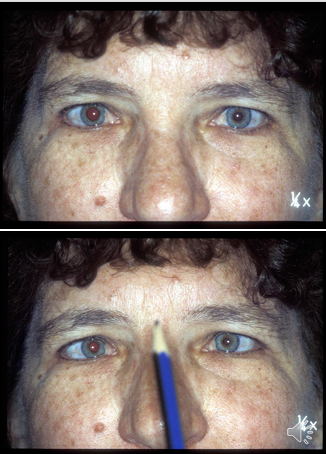
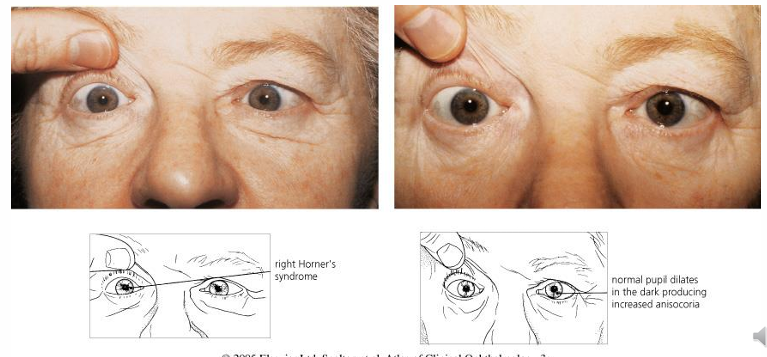
Anisocoria greater in the dark.
Intact pupil reflexes (to light and near).
Dilation lag: the affected pupil will dilate in the dark more slowly compared to the unaffected side (anisocoria diminishes with time spent in the dark environment).
Moderate degree of ptosis due to paralysis of Müller’s muscle.
Elevation of the lower lid (upside down or inverse ptosis) due to paralysis of smooth muscles attached to the tarsus.
Apparent enophthalmos due to apparent narrowing of palpebral fissure.
Reduced ipsilateral facial sweating (anhidrosis), but because the sudomotor fibers supplying the skin of the face run along the external carotid artery, this occurs only if the lesion is below the superior cervical ganglion.
Heterochromia is present only if congenital or acquired in early infancy (the affected eye is lighter).
Pharmacological Testing for Horner’s Syndrome
Pharmacological tests can aid in diagnosis and indicate which order neurons are affected.
Classical test:
4-10% cocaine, 1 drop each eye
Blocks reuptake of norepinephrine at the synaptic cleft.
The normal eye pupil dilates and lids retract because of this blockade.
Horner’s eye has no epinephrine release to be blocked, so no change in pupil size.
The cocaine test confirms the presence of Horner’s syndrome.
not readily available to optometrists
Apraclonidine 0.5% (an alpha agonist) will dilate a Horner’s pupil with no change to the normal pupil (due to denervation supersensitivity in Horner’s).
available to optometrists = can be performed in clinics.
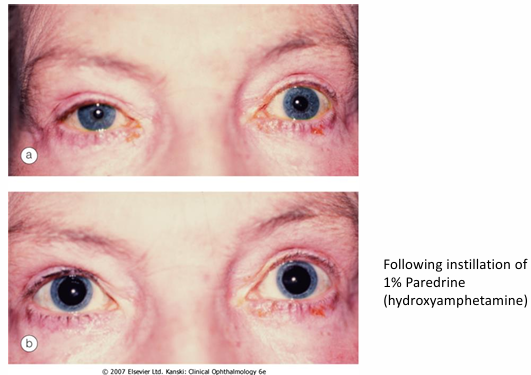
Pharmacological testing can also assist in localizing Horner’s syndrome as being central (first-order) or pre-ganglionic (second-order) or post-ganglionic (third-order).
1% hydroxyamphetamine (Paredrine) - stimulates release norepinephrine into synapses from post-ganglionic nerve endings.
If 1st or 2nd order neurons are damaged and the final 3rd order pathway (i.e., post-ganglionic) is intact, 3rd order neurons can still produce and store norepinephrine.
When paredrine is instilled, pupils will dilate because 3rd order neurons are still able to transport and store norepinephrine.
If 3rd order neurons are also damaged, the affected eye will not dilate.
The Paredrine test, therefore, differentiates 3rd order Horner’s from 1st and 2nd order.
First and second-order lesions are important, as many have sinister causes (e.g., Pancoast’s tumor of the lung).
Requires referral!
Phenylephrine 1% will dilate a post-ganglionic Horner’s - due to sympathetic denervation sensitivity. It will not dilate pre-ganglionic Horner’s.
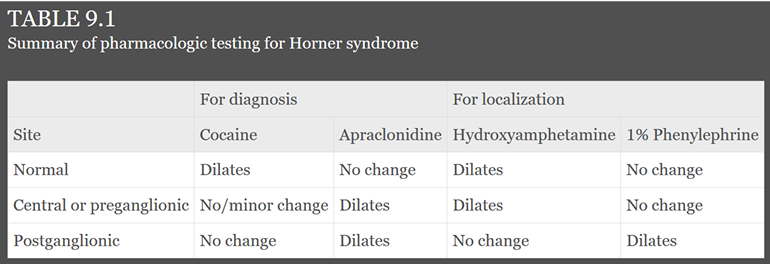
Summary of Pharmacologic Testing for Horner Syndrome
Normal | Central or preganglionic | Postganglionic | ||
|---|---|---|---|---|
Cocaine | Dilates | No/minor change | No change | |
Apraclonidine | No change | Dilates | Dilates | |
Hydroxyamphetamine 1% | Dilates | Dilates | No change | |
Phenylephrine | No change | No change | Dilates |

Acquired Horner’s Syndrome
Acquired Horner’s needs urgent referral due to pathological basis.
The long path of sympathetic innervation means many potential (and significant) causes.