W11: Abnormal Colour Vision
Abnormal Colour Vision
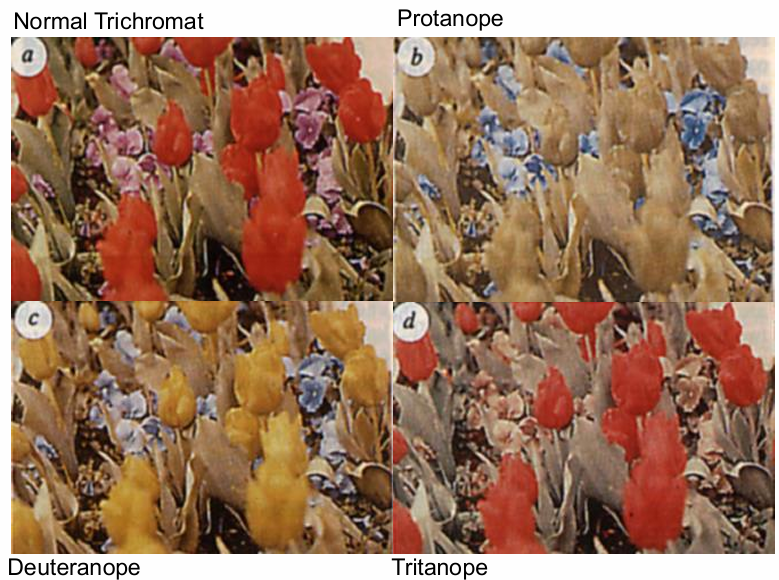
Normal Trichromat
Protanope
Deuteranope - losses in red-green pathway - no M cone
Tritanope
Colour Vision Learning Outcomes
Characteristics of Human Colour Vision
Visual Function (e.g., hue and saturation discrimination)
Abnormal Colour Vision
Monochromacy and Dichromacy
Types of colour vision deficiencies (congenital, acquired)
Characteristics of abnormal human colour vision
Colour perception of people with CVD’s
Colour confusions
Acquired colour vision deficiencies
Clinical testing for abnormal colour vision (pseudoisochromatic plates, arrangement tests, Rayleigh colour matching)
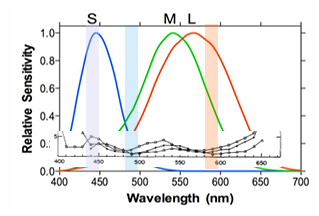
Characteristics of Human Colour Vision: Hue and Saturation Discrimination
Hue (chromatic) discrimination ability
Moving parallel to spectral locus changes hue
Hue/wavelength discrimination: the smallest change in wavelength (hue) which can be distinguished as a change in colour
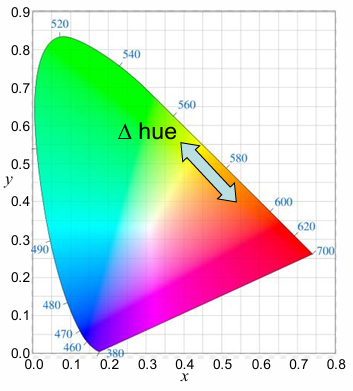
To measure hue discrimination, determine how much a wavelength can be changed before a colour difference is perceived.
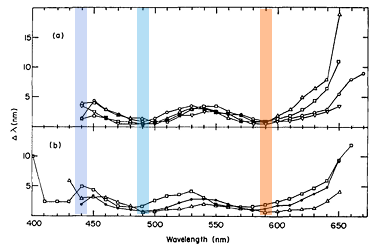
Discrimination ability varies with wavelength
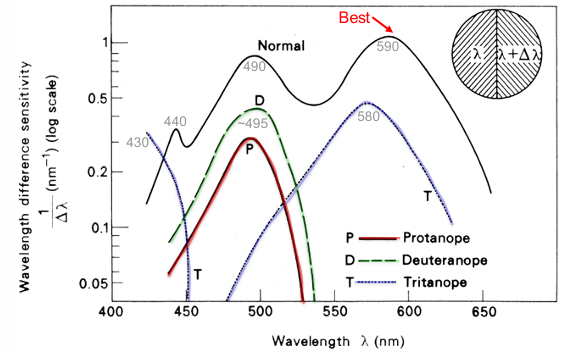
Trichromat has 2 regions of best discrimination (minima) at 490nm & 590nm; can detect 1-2nm (3rd region at ~440nm)
poorer discrimination in-between & at spectral extremes (maxima at ~460nm & 530nm)
short and long wavelengths have reduced discrimination
To discriminate between different wavelengths, the ratio of each cone photoreceptor output to the light is compared
Discrimination is best when the difference in photoreceptor output is highest
when outputs are close together, thats when you start to require greater spectral differences to notice.
Saturation Discrimination
Calculate
Moving out from white changes saturation
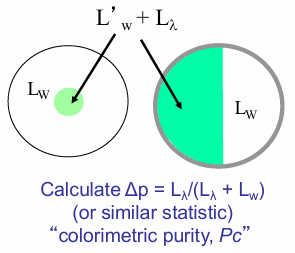
Saturation discrimination: Amount of colour added to a white stimulus so that the stimulus first appears coloured ( )
Peak at 570-580 nm (yellow): Yellow is the “least saturated” spectral hue
Saturation Discrimination is best (minimum) near 400 nm and intermediate at mid spectrum & long
To measure saturation: Calculate (or similar statistic) “colorimetric purity, Pc”
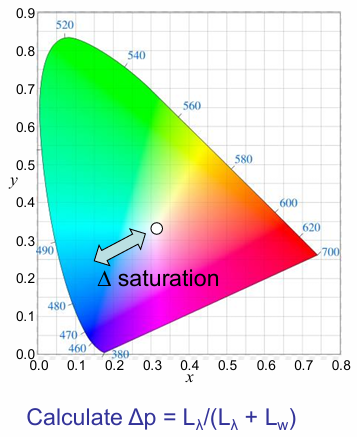
best saturation discrimination is at shorter wavelengths and longer wavelengths.
worst saturation discrimination is in the intermediate wavelengths near yellow.

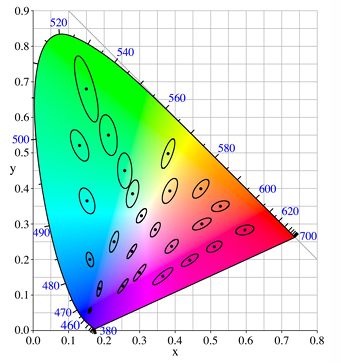
MacAdam Ellipses
Precision of colour matching limited by sensitivity to small colour differences
Within these ellipses all samples appear identical to observer
in green region need a larger change to detect discrimination (i.e., worse discrimination)
allows more errors in green region than in blues in manufacturing industries.
Vary in size & orientation in different areas of colour space
Abnormal colour vision
Colour Blindness Fatal Consequences
Lagerlunda (Sweden) collision of November 1875; 9 people died in the accident
Driver did not see red stop lamp and thought the line was clear…
Beginning of campaign for colour vision screening of railway employees and the development of Lantern colour vision test.
How CV depends on the number of cone photoreceptors?
A photoreceptor only counts the number of photons it absorbs: The Principle of univariance
Photoreceptors cannot discriminate wavelength, therefore a person with a single cone class is completely “colour blind”
The implication is that 1 photoreceptor can match any test with any other by simply adjusting the irradiance
This is a UNIVARIANT (colour) vision system called monochromacy (i.e., rods only), but it is very rare (~1 in 30,000)
2 cone photoreceptor systems
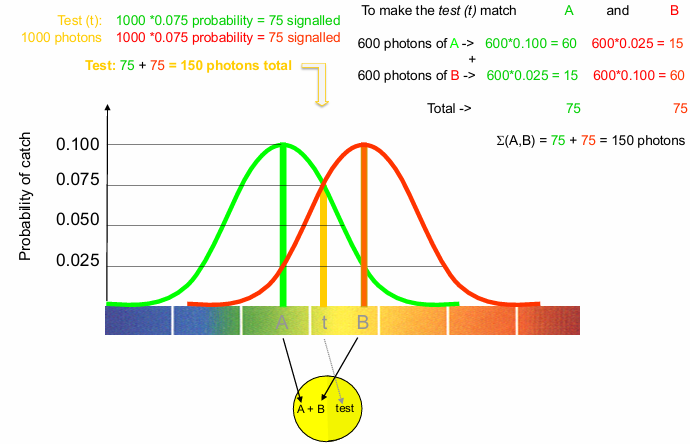
In general, can match any test by adjusting the irradiances of TWO other ‘s.
This is a BIVARIANT colour vision system
Bivariant systems code differences in intensity & 1 dimension of colour: these systems are dichromatic
There are many people with such visual systems….
Colour Vision Deficiencies - Dalton Eye’s
1794 John Dalton (developed atomic theory) analysed his own "strange" colour vision
Saw two main hues only in rainbow spectrum: ROYG - BIV
Brother had same CVD
Thought that all CVD was the same
Proposed CVD was due to blue tinted vitreous (absorbing all red light)
Instructed that his eyes be dissected after his death…
Dalton died age 78 (27 July 1844)
His medical attendant, Joseph Ransome did an autopsy the next day
Collected humours of one eye into a watch glass
Found to be "perfectly pellucid” (i.e. clear)
Lens was normal yellow for age
Other eye left basically intact
Sliced off posterior pole to view through eye
He noted that red and green objects were not distorted
Pity Dalton was not around to believe his own eyes
Ransome found no support for CVD being due to a pre-retinal filtering
Did not discard the eyes, but kept them in air, and they are still intact (more or less) today
Small fragments were taken (1 mm3) for DNA analysis
Confirmed Dalton had DNA to code for only 2 cone types
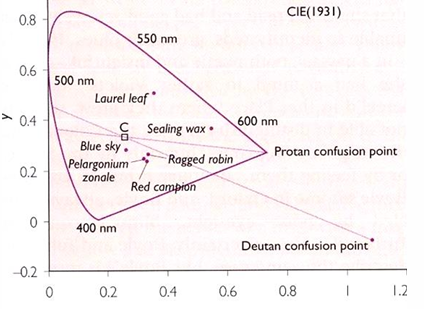
Plotted are flowers that looked blue to Dalton (e.g. red campion, ragged robin).
Dalton also judged red sealing wax & the upper side of a laurel leaf be similar.
The protan and deutan white confusion lines are shown.
What type of CVD might Dalton have had? Dalton was missing a M cone -= deutanope
Deutan confusion - spectral sensitivity of the M cone
Protan confusion - spectral sensitivity of the M cone ????????
Types of Colour Vision Deficiencies
Genetics of Colour Vision
Photopigments are opsins (proteins) coded by genes
In trichromats there are 3 cone opsins (L, M and S) plus rhodopsin & melanopsin
Rod photopigment gene: Chromosome 3
Melanopsin photopigment gene: Chromosome 10
S photopigment gene: Chromosome 7
L and M photopigment genes on X chromosome (one after the other)

Most common CVD are congenital L- & M-cone defects
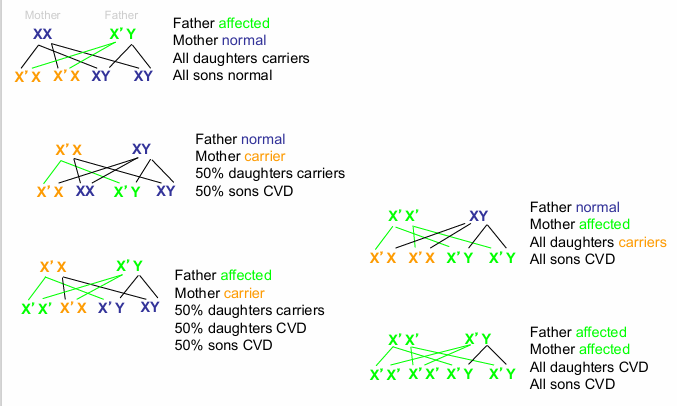
Sex linked recessive means the abnormal gene is carried on the X chromosome & is recessive to the normal gene
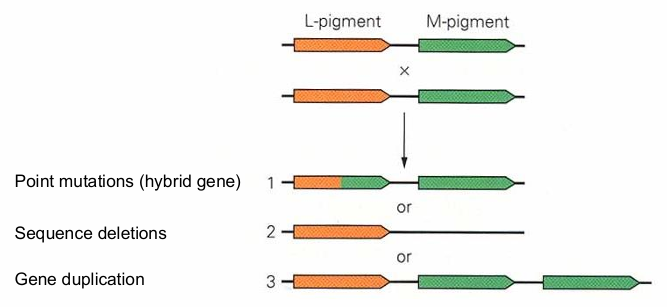
CVD’s can arise due to a recombination of the opsin genes that lead to abnormal genes that are non-functional or compromised because of:
Point mutations (hybrid gene)
Sequence deletions
Gene duplication
Red-green CVD inheritance
Congenital CV Defects: Degree
People with congenital CVD’s have one or more cone pigments that are either missing or altered; this determines the degree of their colour vision deficiency
Two types of monochromats:
Rod monochromat: no functioning cone pigments, low VA, photophobia, nystagmus
Cone monochromat: two cones totally malfunction, S- only?, reduced VA, photophobia? Nystagmus? rare
Dichromatism
One cone type absent
Protanopia: no LWS, L-cone opsin (erythrolabe)
Deuteranopia: no MWS, M-cone opsin (chlorolabe)
Tritanopia: no SWS, S-cone opsin (cyanolabe)
With 2 cone types, can match all colours with 2 primaries
Anomalous Trichromatism
most common type of CVD
3 cone types, but 1 has a shifted (peak) spectral sensitivity
Range in severity (depending on the shift in spectral sensitivity)
Protanomalous: LWS shifted to MWS (10nm peak difference)*
Deuteranomalous: MWS shifted to LWS (6nm peak difference) *
Tritanomalous: Abnormal SWS, reduced blue
3 primaries to make a match; matches differ from trichromats
*DeMarco, Pokorny & Smith (1992): Note that the peak difference in LMS and MWS opsins is ~23nm in trichromats
Inheritance and incidence of colour vision deficiencies
Type | Form | Inheritance | Incidence | Classification |
|---|---|---|---|---|
Protan & Deutan | X-Chromosome linked recessive | 8-10% males <1% females | ||
Protanopia | Missing L-cone photopigment | 1% males | Dichromatic | |
Deuteranopia | Missing M-cone photopigment | 1% males | Dichromatic | |
Protanomaly | Anomalous L-cone photopigment | 1% males | Trichromatic | |
Deuteranomaly | Anomalous M-cone photopigment | 5% males | Trichromatic | |
Tritan | Autosomal Dominant | |||
Tritanope | Missing S-cone photopigment | 0.002 - 0.007% | Dichromatic | |
Tritanomaly | Anomalous S-cone photopigment | Trichromatic |
Rod, cone and atypical monochromacies are very rare
(Female) Carriers of Colour Vision Deficiencies
~15% of women are heterozygous carriers of X-linked red-green CVD
~4.2% are protan carriers; less sensitive to red light: Schmidt’s sign (Schmidt, 1934)
~11.7% are deutan carriers; more sensitive to red light: deVries sign (deVries, 1948)
(Note: deVries sign is more difficult to demonstrate than Schmidt’s sign)
Many carriers present with slight or moderate reductions in colour vision as indicated by:
Increased errors on the Ishihara test
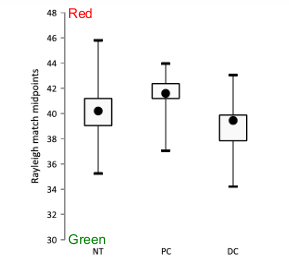
Slight shift in the Nagel match midpoint & enlarged Nagel matching range on Raleigh anomaloscopy
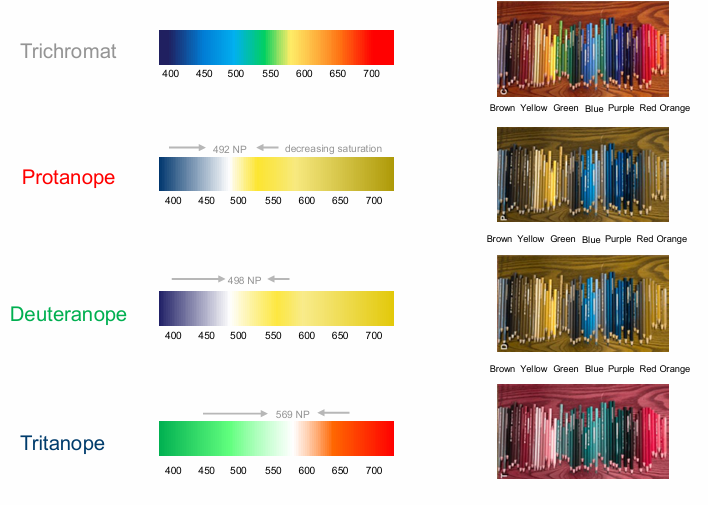
Colour Perception of Persons with Colour Vision Deficiencies
Persons with colour vision deficiencies have:
Confusion of colours which appear very different to a person with trichromatic colour vision
A reduction in the number of separate colours which may be seen
Colour matching in CVD does not look like a match to a person with trichromatic colour vision
However, at mesopic light levels, the rods act as a third photopigment and dichromatic colour matches are comparable to trichromats (Smith & Pokorny, 1977)
The presence of a 3rd, poorly represented cone type, may be involved in this categorisation (Montag & Boyton 1987)
Relative Luminous Efficiency
trichromatic: peak at 555nm
Protanope: Peak shifts to shorter wavelengths (protanope: 530 nm), marked reduction in long wavelength sensitivity
Deuteranope: Peak shifts to longer wavelengths (deuteranope: 565 nm)
Tritanope: Almost normal curve, slight reduction at short wavelengths (<540nm)
Deuteranomaly: M-cone spectrum displaced toward long wavelengths
Protanomaly: L-cone spectrum displaced toward short wavelengths
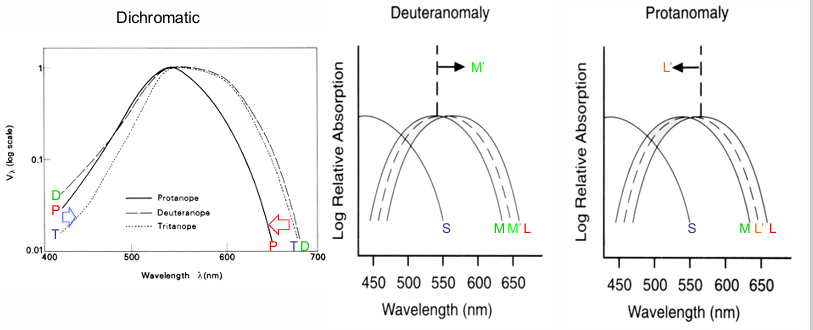
Solid curves show the normal cone absorption spectra, dashed curves the locations of the displaced spectra
Colour Naming in Dichromats
Dichromats can name the appearance of 4°diameter colour samples (from the OSA Uniform Colour Scale) in fair agreement with colour normal observers, including along the red-green dimension (plus the lightness and blue-yellow dimensions)
When stimuli are limited to the central fovea, or when rods are bleached, dichromats cannot categorize colours along the red-green dimension
At scotopic illuminations, dichromats do not assign colour names based on the scotopic lightness or stimulus spectral composition (as do trichromats); their lifetime experience with a reduced photopic colour gamut may contribute to this.
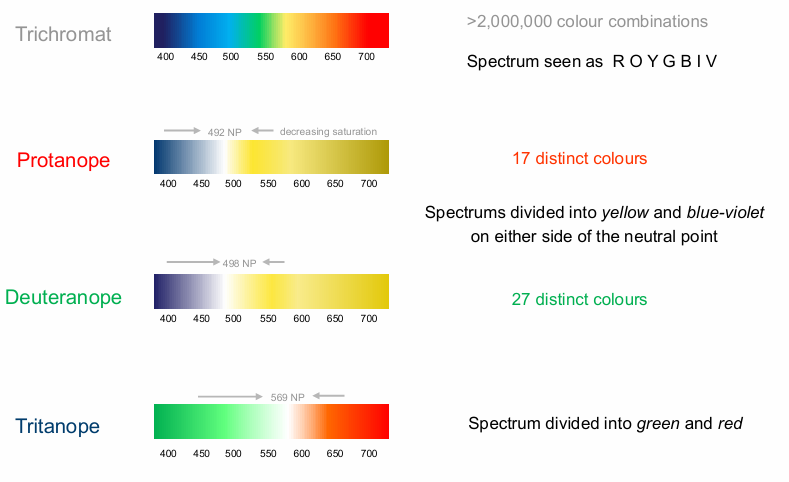
Appearance of the colour spectrum
Normal CV: Ends of spectrum are dim compared to middle two areas. Most white appearing area (desaturated) is in the yellow portion of the spectrum
CV defective: Observations differ depending on defect
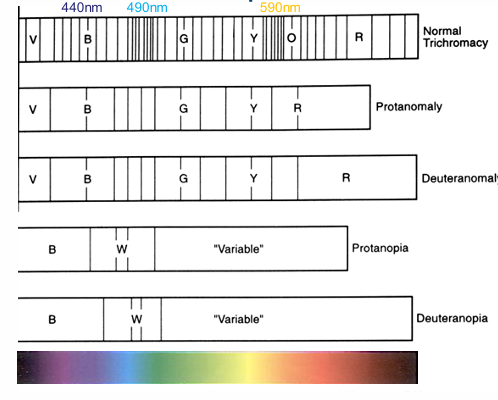
Density of vertical lines reflects wavelength discrimination.
Spectrum for dichromats (protanopes/ deuteranopes) divided into a blue and “variable” region separated by the white neutral point (W).
Variable: observers label these wavelengths based on brightness & context cues
Hue / Wavelength Discrimination
Protanopes/Deutanopes: Single minima at ~495nm, unable to detect differences >520-530nm
Protanomalous/Deutanomalous: Range between the normal & dichromat, minima ~495 & 610, no short wavelength minima
Tritanopes: 2 minima ~430 & 580nm, unable to detect differences between 450 & 480nm
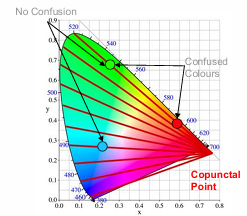
Colour Confusions
Dichromats accept trichromatic colour matches whereas dichromatic colour confusions are easily distinguished by the trichromat
People with CVDs will confuse colours located on the same confusion lines (i.e., are unable to discriminate between equal-luminant colours)
Confusion line passing through white that intersects the spectral locus defines the point in the spectrum which appears achromatic (neutral point)
These neutral points (perceived as grey/achromatic) occur at
492 nm (protanope)
498 nm (deuteranope)
569 nm (tritanope)
Confusion lines converge at a single point, the copunctal point (cp), which is the spectral response of the missing photoreceptor; people with CVDs confuse colours located on the same confusion lines
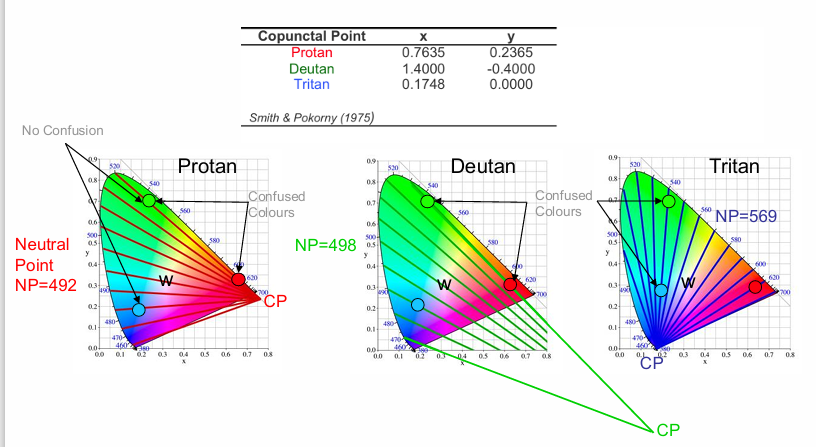
Neutral Point (NP): part of the spectral locus that appears achromatic
draw from CP through white to locus point.
protan and deutan will confuse red and green (same confusion line)
tritan will confuse blue and green (same confusion line)
Dichromatic Colour Gamuts
Trichromat: >2,000,000 colour combinations. Spectrum seen as R O Y G B I V
Protanope: 17 distinct colours. Spectrum divided into yellow and blue-violet on either side of the neutral point
Deuteranope: 27 distinct colours
Tritanope: spectrum divided into green and red
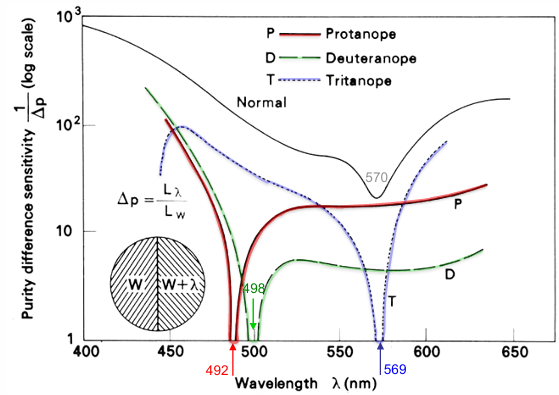
Saturation Discrimination
Normal observer: 570nm least saturated
Protanope: function crosses x-axis at 492nm
Deutanope: at 498nm
Tritanope: at ~569nm
When cross x-axis, these wavelengths appear white: Neutral Points
Acquired Colour Vision Deficiencies
Acquired CV Deficiencies
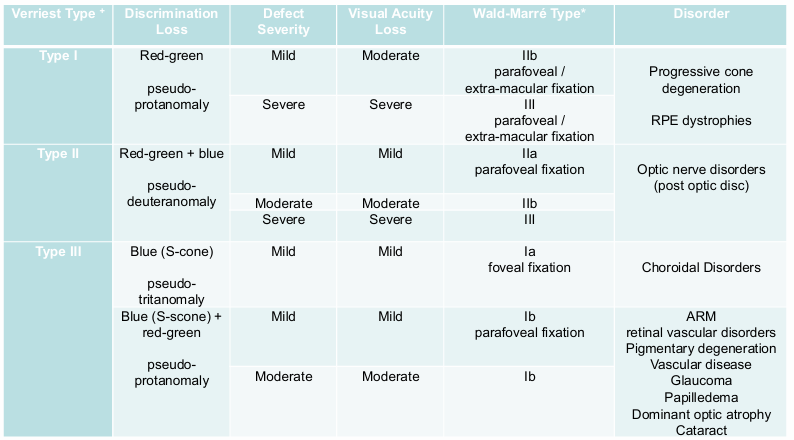
Wald Marre Type = location effected
Distinctions between hereditary and acquired colour vision defects
Hereditary Defects | Acquired Defects |
|---|---|
Typically, red green | Often blue yellow |
More prevalent in males | Equally prevalent in males and females |
Symmetric: Same in each eye | Asymmetric: Often a difference in severity between eyes |
Colour naming errors are rare | Recent history of colour naming errors |
Defect is stable with time | Defect is unstable and changes over time |
Easily classified with standard colour vision tests | Classification often not straightforward |
Not associated with disease | Associated with ocular or system disease |
Testing for Colour Vision Deficiencies
Most tests rely on colour confusions in CVD
Pseudoisochromatic (PIC) Plates (e.g., Ishihara)
Hue discrimination (arrangement) tests: D15, Farnsworth-Munsell 100-Hue, Lanthony desaturated
Colour matching (Nagel anomaloscope)
The tests use colour confusions designed to detect & classify congenital defects, not acquired colour defects
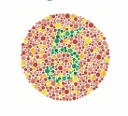
Ishihara Pseudoisochromatic plates
Pseudoisochromatic plates are examples of colour camouflage
Colours within confusion zones can be substituted without a person with a CV defect noticing:
These are "isochromatic" (same colour) pairs for those with CVD
hence "pseudo-" (falsely) "-isochromatic" (same colour)
Ishihara plates screen for red-green CV
American Optical HRR (Hardy Rand Rittler) plates screen for tritan defects
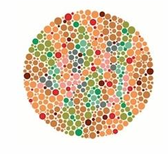
Embeds chromatic differences within spatially varying luminance-contrast noise (spots of different sizes)
Noise ensures detection relies on chromatic discriminations & not luminance differences associated with the different colours (important because individual luminous efficiencies differ)
dichromate cannot use luminance differences to detect target.

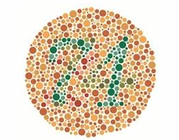
top image: what number?
bottom image: trace path from left side to right side
4 pseudoisochromatic plate designs
Vanishing Design: Perceived by trichromats (e.g. #5), invisible with red-green CVD
Hidden Design: Figure is camouflaged for trichromats, visible to dichromats
Transformation Design: Combines hidden & vanishing concepts: Trichromats perceive one figure (e.g. #74), dichromats perceive another (e.g. # 21)
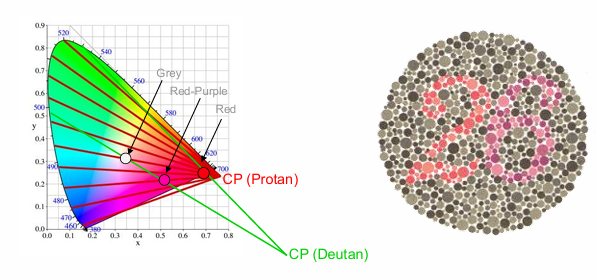
Classification design: Differentiates between protan & deutan: Different confusion loci depending on which cone system is defective
Protans confuse red and grey (perceive 6)
Deutans confuse red-purple and grey (perceive 2)
Hue Discrimination (arrangement) Tests
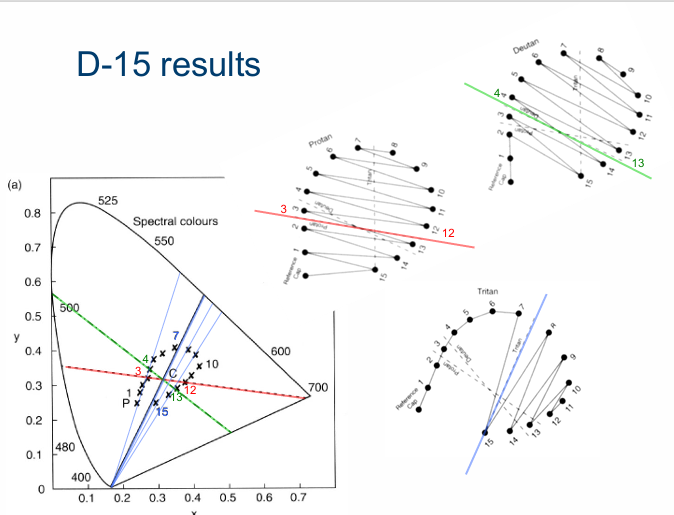
D-15
16 hues (one fixed reference hue): Munsell value = 5, chroma = 4
Patients arrange colour in order
Colours encircle illuminant C
Identifies the CVD type and severity (moderate/severe)

L’Anthony Desaturated D-15
Munsell hue same as D-15 with value = 8, chroma = 2 (desaurated)
Used to analyse defect severity (and for screening acquired CVDs)
D-15 Principle
Isochromatic confusions occur when colours from opposite sides of the hue circle are placed together
Less severe CVDs make fewer confuse isochromatic confusions

Scoring
Number of isochromatic crossings
Sum of the colour differences b/w adjacent colours
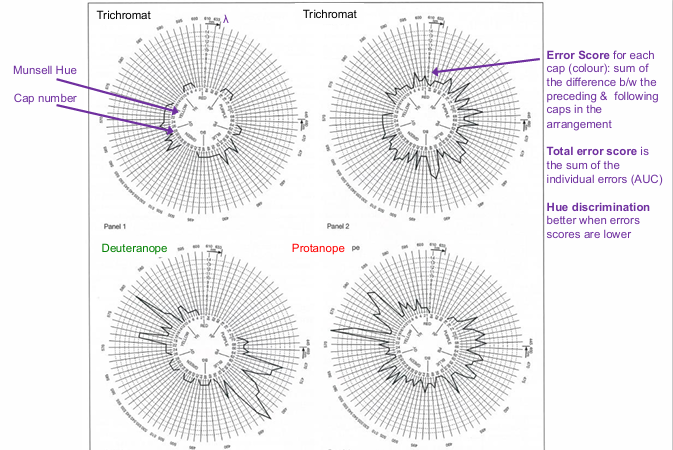
The Farnsworth-Munsell 100 Hue Test
Devised by Farnsworth (1943)
85 coloured samples with similar chroma & value encircle illuminant C
Assesses colour discrimination
Useful for moderate and severe congenital & acquired CVD
Provides a colour aptitude assessment in normal trichromats
Data indicate total error score (incorrect discriminations within a box) & axis

Error Score for each cap (colour): sum of the difference b/w the preceding & following caps in the arrangement
Total error score is the sum of the individual errors (AUC)
Hue discrimination better when errors scores are lower

retinitis pigmentosa - red / green defectsz
optic neuropathy - yellow defects
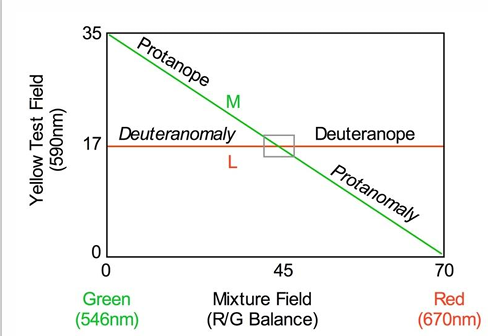
The Rayleigh Match
Spectral locus between 545 & 700nm approximates a straight line; any wavelength on this line can be matched be appropriate combination of 2 lights
The dotted line formed by connecting Red, Yellow & Green primaries correspond to a colour confusion line shared by deuteranopes and protanopes
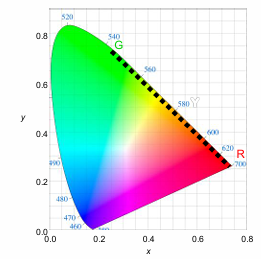
Gold standard colour vision test for protanopia and deuteranopia
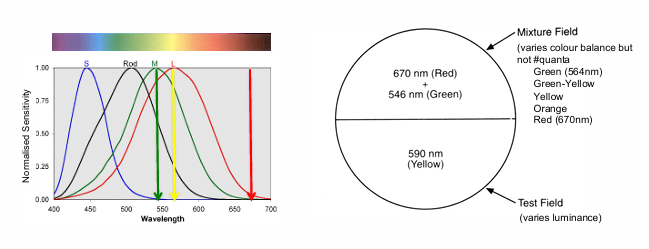
Uses a Rayleigh (1881) match:
Vary proportion of Green 546nm & Red 670nm primaries (varying only in colour balance) to match the yellow 590nm primary (of variable luminance)
The Moreland (1978) equation assesses S-cone function: Match a blue-green bicolour test field with 480 & 580nm to a mixture of 430 & 500nm
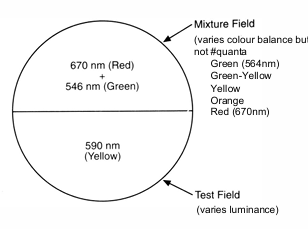
number of quanta remains constant throughout.
2° field (Nagel, 1907), photopic (no rod intrusion)
S-cones insensitive to the 3 primary lights
Anomaloscope set to “deut” mode; spectral sensitivity of deuteranopes involve only L-cones for wavelengths >545 nm & so any R/G balance ratio (# quanta) will match the fixed yellow value (50% or 17 units)
for every combination of red and green, there will only be one amount of quanta in the yellow (~50%) that will match the other mixture field.
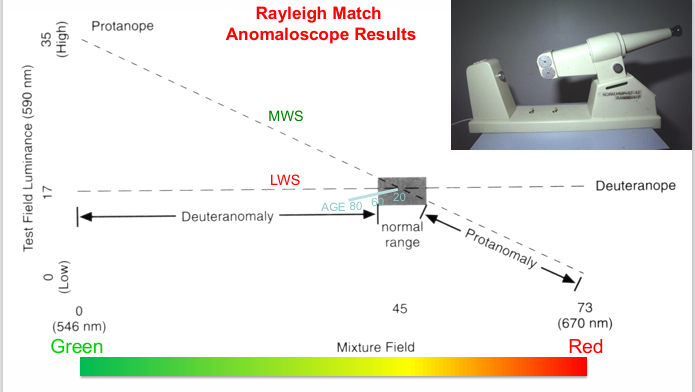
Deuteranope: Matches mixture fields with a constant test field luminance
Protanope: Matches all mixture fields; however, must adjust the test field luminance
Trichromat: Average normal matches occurs at intersection of Protan/Deutan matches
Age: Increased lens absorption causes Rayleigh matches to shift toward the green
Rayleigh matches with the Nagel Anomaloscope
Adjusting the R/G balance changes the colour not number of quanta
Rayleigh Match calibrated for an (L-cone) ('Deut' Mode)
Trichromats accept only a small range of R/G ratios, near the middle (~45)
Deutan:
Due to the “Deut’ calibration, all R/G ratios match 50% yellow whereas only one yellow luminance (i.e., 50%) matches the R/G ratio
Therefore test field (Y) flux is constant for all R/G ratio
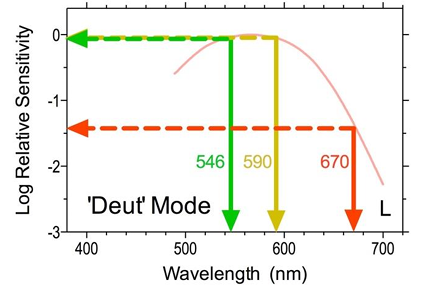
Protan:
Protanope (M-Cone) sensitivity to Y is reduced compared to Deuteranopes (compare middle and lower panels)
Because the R/G balance is calibrated to the irradiance of Y in 'Deut' mode, if R/G mixture ratio was set to all R (i.e., 70), then the mixture field would appear dimmer than the test
The Protan must therefore increase the irradiance of Y and compensate for a reduced sensitivity to R by adjusting the R/G balance toward G to make the match
Questions
How does human saturation discrimination change between trichromats and dichromats?
Discuss the limits of hue and saturation discrimination in humans
Differentiate between hereditary and acquired colour vision defects
How are colour vision tests designed to detect and classify congenital deficiencies in clinical practice?