Voltage-Gated Ion Channels in Cardiac Physiology
Overview:
The heart’s rhythmic contractions depend on precise, timed changes in membrane potential, driven by voltage-gated ion channels (VGICs).
These channels open or close in response to changes in voltage across the plasma membrane, allowing ion fluxes that underlie cardiac action potentials (APs).
Understanding VGICs links genotype to phenotype, as mutations in their genes directly lead to cardiac channelopathies such as Long QT and Short QT syndromes.
The lecture focuses mainly on voltage-gated Na⁺ (NaV) and K⁺ (KV) channels, which determine the initiation and termination of each heartbeat.
Membrane Transport and Ion Gradients:
Membrane proteins involved in ion movement:
Ion channels – allow selective, passive diffusion down an electrochemical gradient.
Carriers (facilitated transporters) – bind substrates and change conformation to move them across the membrane.
Pumps (active transporters) – move ions against their gradients using ATP hydrolysis (e.g. Na⁺/K⁺-ATPase).
Resting Membrane Potential (RMP):
Typical cardiac RMP: –80 to –90 mV.
Maintained by:
Na⁺/K⁺-ATPase: 3 Na⁺ out / 2 K⁺ in (net + charge out).
K⁺ leak channels: allow passive K⁺ efflux → inside becomes negative.
Intracellular fluid: high [K⁺], low [Na⁺]
Extracellular fluid: high [Na⁺], low [K⁺].Nucleic acids and proteins contribute to intracellular fixed negative charge, reinforcing the electrical gradient.
❗Nucleic acids and proteins contribute to intracellular fixed negative charge, reinforcing the electrical gradient.
Action Potential Fundamentals:
Depolarisation:
Voltage-gated Na⁺ channels open, leading to a rapid Na⁺ influx and so the membrane potential becomes positive.
Repolarisation:
Na⁺ channels inactivate; voltage-gated K⁺ channels open, leading to a K⁺ efflux which restores negativity.
Hyperpolarisation & Refractory Period:
K⁺ permeability remains high briefly which prevents immediate re-excitation, ensuring unidirectional signal conduction.
Overall:
The AP is a transient reversal of electric polarity, converting chemical energy into electrical activity essential for excitation-contraction coupling.
Cardiac Action Potentials:
1. Ventricular Myocytes (Contractile Cells):
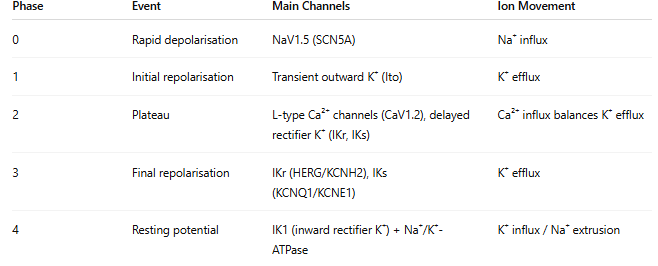
The plateau (Phase 2) is unique to cardiac muscle, preventing tetanus and allowing full relaxation between beats.
— — — — —
2. Pacemaker Cells (Sinoatrial Node):
No true resting potential — exhibits spontaneous depolarisation.
Phase 4 (Pacemaker potential):
Slow Na⁺ entry via funny current (If, HCN channels) and Ca²⁺ via T-type channels.
Phase 0:
Depolarisation via L-type Ca²⁺ channels (Na⁺ channels are largely absent here).
Phase 3:
Repolarisation via delayed rectifier K⁺ channels.
❗Continuous cycling of depolarisation initiates heartbeat, and the action potential is propagated through the conduction system to the ventricles.
Voltage-Gated Sodium Channels:
Structural Features:
Main α-subunit: four homologous domains (I–IV), each with six transmembrane segments (S1–S6).
S1–S4: Voltage-sensing domain (S4 carries repeated positively charged arginines or lysines).
S5–S6: Pore-forming region with selectivity filter.
β-subunits: Auxiliary proteins modifying gating kinetics and expression.
Selectivity filter (DEKA motif):
D (Asp) and E (Glu) are negatively charged → attracts Na⁺.
K (Lys) helps repel larger cations (e.g. K⁺).
A (Ala) provides neutral spacing.
Highly specific to Na⁺ ions, discriminating based on hydration shell and ionic radius.
— — — — —
Gating Mechanism:
Resting state: activation gate closed, inactivation gate open.
Depolarisation: voltage sensor (S4) moves → activation gate opens → Na⁺ influx.
Inactivation: intracellular “ball-and-chain” structure occludes pore within milliseconds.
Repolarisation: channel resets as potential returns to RMP.
— — — — —
Pharmacology and Toxins:
Tetrodotoxin (TTX) and saxitoxin: bind extracellular pore, blocking Na⁺ conduction which leads to paralysis, cardiac arrest.
Certain local anaesthetics (e.g., lidocaine) act by binding the intracellular site and stabilising the inactivated state.
Voltage-Gated Potassium Channels (KV):
Structural Features:
Composed of four separate α-subunits forming a tetrameric pore.
Each α-subunit: six transmembrane segments (S1–S6) + cytoplasmic N- and C-termini.
S1–S4: Voltage-sensing domain.
S5–S6: Pore domain containing the selectivity filter (TVGYG sequence) — confers >1000-fold selectivity for K⁺ over Na⁺.
Auxiliary β-subunits (KCNE family): modulate gating, conductance, and trafficking.
Functional Characteristics:
Voltage sensing (S4): outward movement upon depolarisation triggers opening.
Pore helix: stabilises the selectivity filter and ensures precise ion dehydration/re-hydration during transit.
Key example:
KCNQ1 (α-subunit) + KCNE1 (β-subunit) → forms the slow delayed rectifier current (IKs) crucial for cardiac repolarisation.
Regulation of Cardiac Potassium Channels (KCNQ1):
1. Accessory Subunit KCNE1:
Slows activation/inactivation → lengthens repolarisation.
Provides stability under sustained depolarisation.
Mutations (e.g., S74L, R98W) alter kinetics, producing abnormally fast current decay → electrical instability.
2. Phosphatidylinositol 4,5-bisphosphate (PIP₂):
A phospholipid second messenger anchored in the inner leaflet of the membrane.
Binds the intracellular portion of KCNQ1, increasing pore diameter and favouring the open state.
Reduced PIP₂ binding (e.g., due to mutation near S4–S5 linker) which leads to impaired activation and a Long QT phenotype.
3. Calmodulin (CaM):
Calcium-binding regulatory protein interacting with KCNQ1’s C-terminal domain.
Modulates channel activity in a Ca²⁺-dependent manner.
Competes with PIP₂ for binding which creates fine-tuned feedback control linking cytosolic Ca²⁺ to membrane excitability.
Experimental Techniques:
Patch-Clamp Electrophysiology:
Allows measurement of ionic currents at single-channel or whole-cell level.
By applying controlled voltage steps, one can determine activation thresholds, current amplitude, and kinetics.
Used to characterise mutant channels (e.g., altered time constants or current-voltage relationships).
Findings:
KCNQ1 alone → fast activation;
KCNQ1 + KCNE1 → delayed activation;
Mutant subunits → aberrant kinetics consistent with arrhythmic phenotypes.
Long QT and Short QT Syndromes:
Electrocardiogram (ECG) Overview:
P wave: Atrial depolarisation.
QRS complex: Ventricular depolarisation.
T wave: Ventricular repolarisation.
QT interval: Duration of ventricular depolarisation + repolarisation (normally 360–480 ms).
Long QT Syndrome (LQTS):
Prolonged QT (>480 ms) leads to delayed repolarisation which causes a predisposition to arrhythmias.
Causes:
Loss-of-function in K⁺ channels (KCNQ1, KCNH2).
Gain-of-function in Na⁺ channels (SCN5A).
Types:
LQT1: KCNQ1/KCNE1 defect (IKs current).
LQT2: KCNH2/HERG defect (IKr current).
LQT3: SCN5A mutation (persistent Na⁺ current).
Pathophysiology:
Delayed repolarisation extends AP duration → early after-depolarisations which leads to ventricular fibrillation.
Symptoms: Syncope, seizures, sudden cardiac death, especially under stress or exercise.
— — — — —
Short QT Syndrome (SQTS):
QT interval <360 ms.
Mechanism: Accelerated repolarisation.
Gain-of-function in K⁺ channels (e.g., KCNH2, KCNQ1).
Loss-of-function in Na⁺ or Ca²⁺ channels.
Clinical features: Palpitations, atrial fibrillation, risk of sudden death due to shortened refractory period.