lecture 18
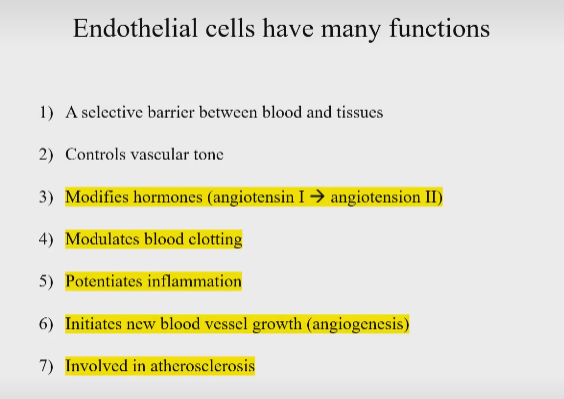
Endothelial Cells Modify Hormones
rednin-angiotensin-aldosterone system
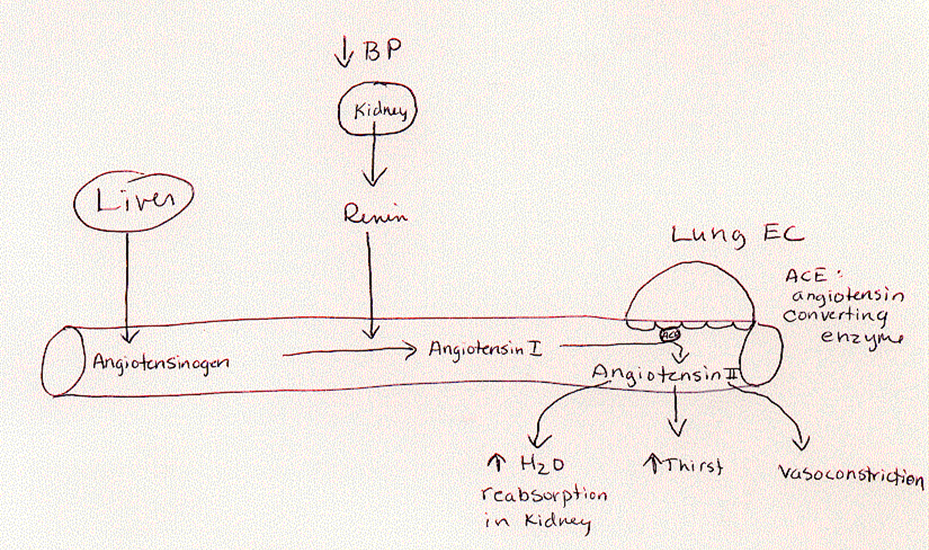
precursor hormone release from liver → angiotensinogen (floating around in blood)
kidney release renin - renin cleaves angiotensinogen (renin is a rate-limitng enzyme)
produced angiotensin I → rapidly converted into Angiotensin II in lungs by ACE
angiotensin II also increases sympathetic nerve action and activity
**endothelial cells are very important bc they have ACE
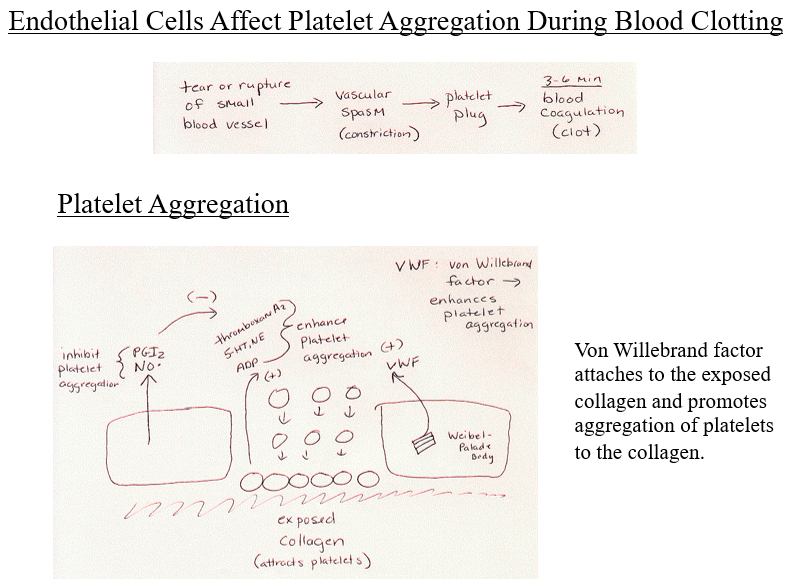
when there is damage, the exposed collagen reacts with the blood
the platelets in the blood are attracted to the collagen
platelets become activited and send out cytokines → cytokines attract more platelets
weibel palade body in the EC nearby release vWF → enhance platelet aggregation
EC not in the damages area will release factors to prevent paltelet aggregation to occur in their region - PGI2, NO* - inhibit platelet aggregation
basally? (i think this means all the time)
ROS impair nitric oxide
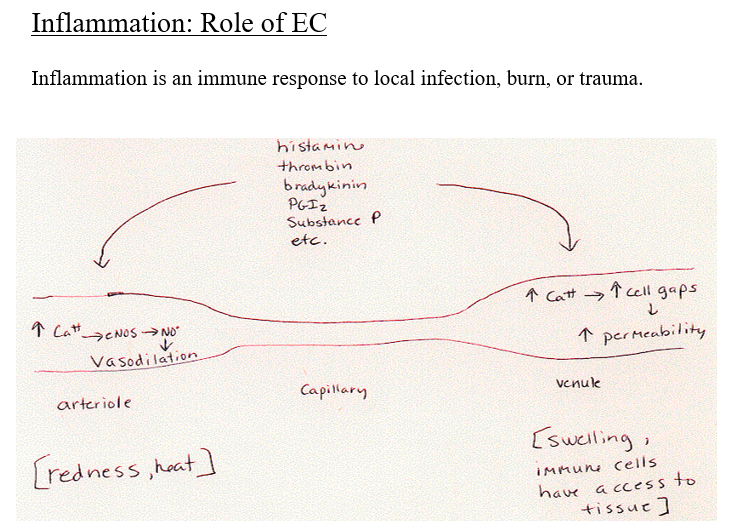
arteriole
increased blood flow
venule
increased fluid into tissue
**maybe watch videos
endothelial cells control infiltration of immune cells (leukocytes) in venules
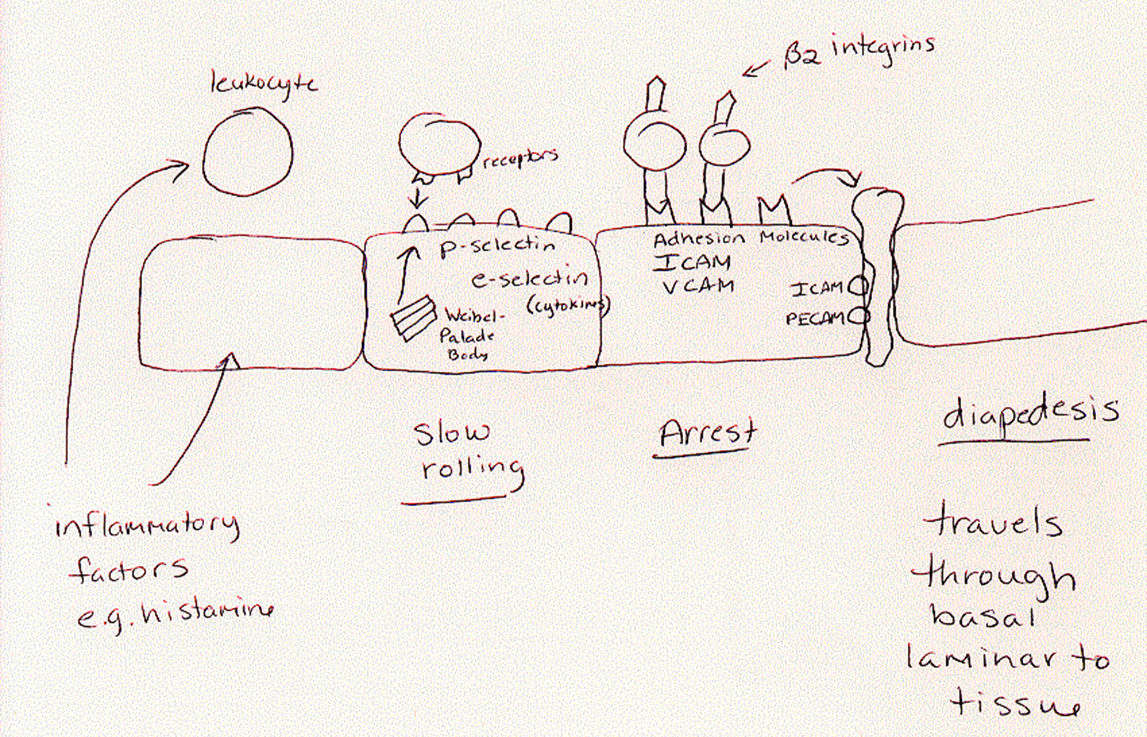
infection in tissues → local immune cells release inflammatory factors (in blood)
slow rolling (loose binding)
this activates EC → start expressing receptors for immune cells
weibell palader body releases P selectin (receptor) that inserts into the membrane
e selectin in the cell (not from weibell body) inserted into memrbane
selectins attract immune cells
immune cells start to express receptors that can bind to selectins
arrest
EC’s start expressin gmore firm receptors - receptors are different shapes
adhesion molecules (ICAM and VCAM) CAM = cell adhesive molecule
leukocytes start expressing different receptor too - will bind tightly
diapedesis
immune cells squeezes through with the help of ICAM and PECAM
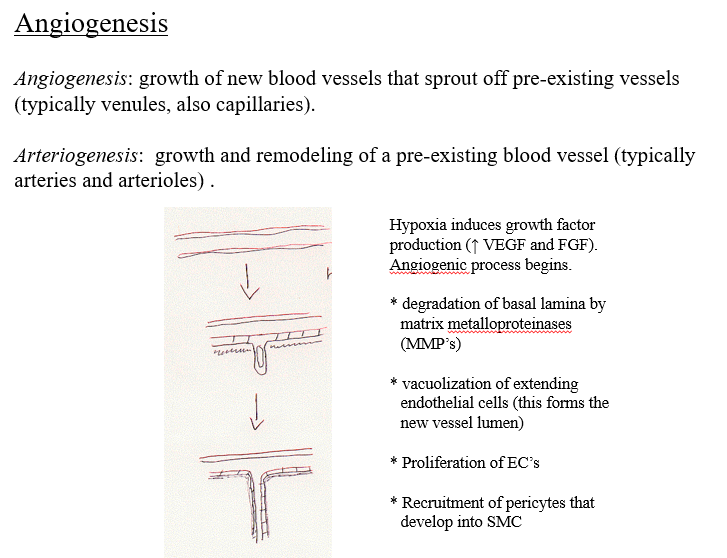
if you have extended hypoxia, you can get lots of new blood vessel growth
stop tumor growth by preventing angiogenic process froom occurring bc tumors need to develop its own supply
3 and 4: remodeling rather than adaptation
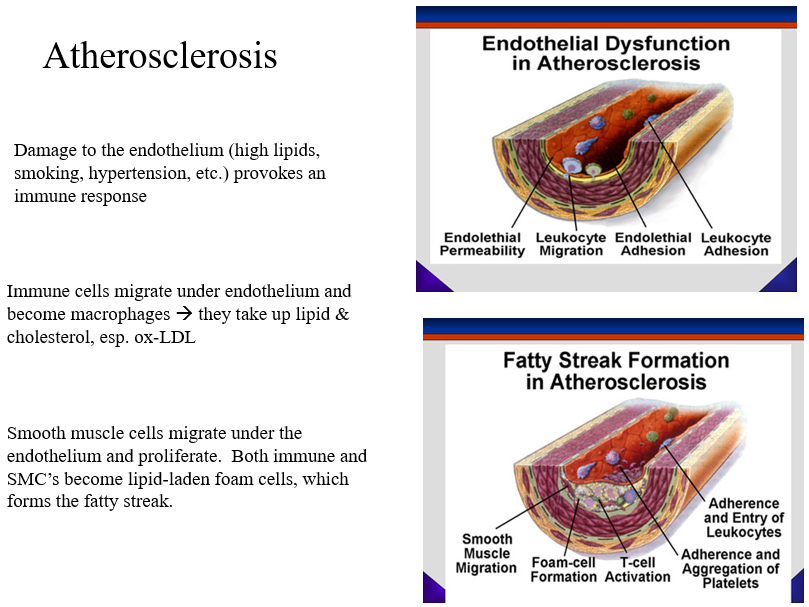
damaged EC’s (dysfunctioinal) provokes immmune cells → activate EC’s
once activated they attract leukocytes
leukocytes infiltrate under EC layer → change into macrophages → then foam cells
macrophages consume LDL chol. (esp oxidized) and small dense LDL
fatty sreak formation from foam cells - lipid laden (full of chol.)
starts in teen years
activated EC’s also cause SMC migration and proliferation
also move underneath EC layer and become macrophages and foam cells
thin cap and big plaque (most dangerous)
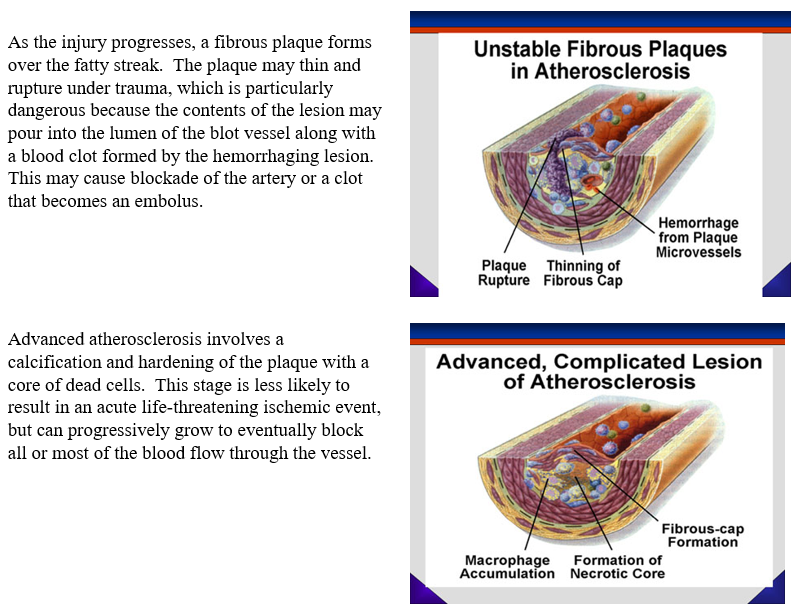
more stable but can block artery