Spotlight F: Childhood Nutrition
Identify four primary objectives for sound nutritional guidance for children
Provide an overview of patterns of growth and development from preschool-aged children to early adolescence (puberty)
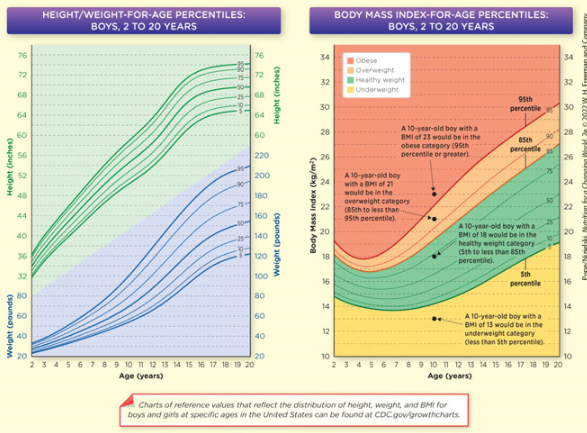
Describe how body mass index is used to assess if children are at a healthy weight for their age
Identify at least three nutritional challenges for children and adolescents
Describe how changes governing the types of foods that are offered at schools are expected to improve the nutrition profile of school meals
Describe how parents can use MyPlate to help in planning a healthy diet for their children
Describe at least three ways parents can foster positive eating habits and food choices
Discuss the consequences of childhood obesity on future health
Describe how food allergies develop, and identify four food allergens that are common among children
Hygiene Hypothesis
Less exposure to dirt and germs
Reduced exposure to childhood
infections in developed countriesImpairs normal maturation and
regulation of the immune systemMay explain the increasing prevalence of food allergies and other immune disorders, such as asthma
Growth Charts
Indication of adequate nutrition
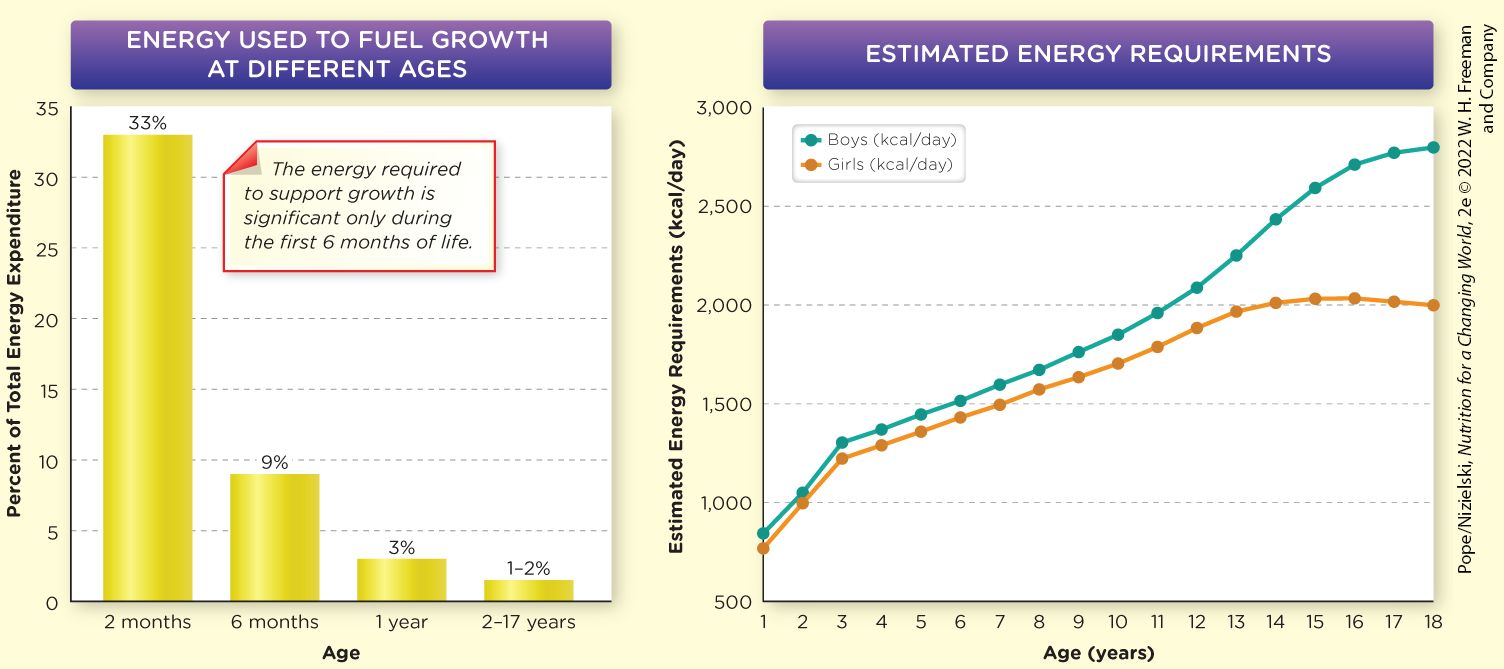
Growth in Early Childhood
• Rapid growth during infancy
• Growth slows in preschool
children aged 2-5 years
• Average increases
– Weight ↑ 4.5-6.6 pounds/year
– Height ↑ 3-4 inches/year
Growth in School-aged Children
Vary in height, weight, and build during the school years
Due to genetics, nutrition, and exercise patterns
Ages 6 to 11
Growth spurts = Periods of accelerated physical development
Average increases
• Weight ↑ 6.5 pounds/year
• Height ↑ 2+ inches/year
Growth During Puberty
A time of development with periodic growth spurts
Changes in body size, shape, composition, and sex-
specific maturation~50% of adult body weight is gained during puberty
Boys
– Typically begins at age 12 or 13
– Span of about 4 years
– Average increase~2.5 inches in height/year
11+ pounds in weight/year
Girls
– Typically begins at age 10 or 11
– Average increase~2 inches in height/year
~9 pounds/year in fat and lean mass
Dietary Intake for US Children
Diets of children in the U. S. are typically:
– ↑ energy-density
– ↓ nutrient-density
– ↓ greens and beans
– ↓ fiber
– ↓ vegetables
– ↓ whole grains
– ↓ plant proteins
According to the 2020 DGA, US children and adolescents aged 5-18
~ 80% exceeded added sugars
~ 80% exceeded saturated fats
> 95% exceeded sodium
More meals away from home
Fast-food tends to be energy-dense and nutrient-poor
Children who eat the most fast-food have higher intakes of
total energy, saturated fat, and sodium
Larger portions
Children tend to eat less when can serve themselves
Fewer family mealtimes at home
Children who eat at home tend to eat more nutritious food
Drink less milk and more soft drinks
On average, children consume close to 10% of total calories from sugar-sweetened beverages
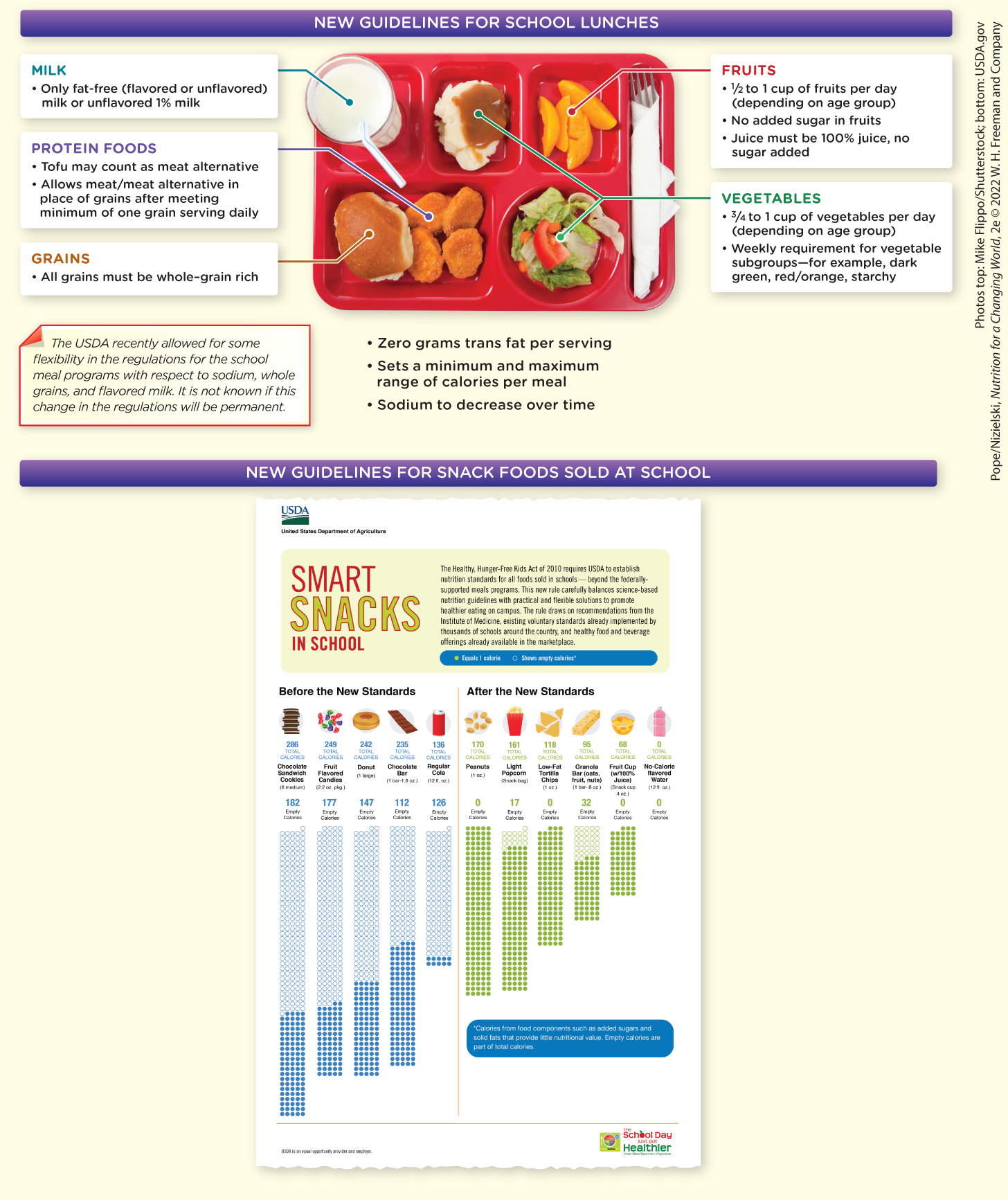
National School Lunch Program
Millions of children participate
Federally assisted program
Provides nutritionally balanced, low-cost or free meals to children each school day
2010 Healthy, Hunger-Free Kids Act
USDA issued new standards in 2012 to ensure meals align with Dietary Guidelines for Americans
Increase fruits and vegetables
Emphasize whole grain–rich food
Serve only low-fat and nonfat milk
Limit calories
Reduce saturated fat and sodium
DGA are the foundation for nutrition standards for NSLP

Shaping Eating Behaviors of Children
Eating behavior is strongly influenced by:
Physical & Social Environment
Parental Influence
Children as young as 2 should control the quantity of
food consumed to avoid excess intake and habitual
overeating
Fostering positive eating behaviors & habits
– Provide a variety of nutritious foods
– Repeat exposure to nutritious foods
– Encourage, but do not force, nutritious foods
– Model food choices and practices
Food Jags
Habits or rituals formed by children
– Ex. Eat only sandwiches cut into squaresDevelopmentally “normal” as they strive for more
independenceGenerally outgrown with patience and guidance
Physical Activity
Lower activity associated with lower diet quality
US Department of HHS recommend children and adolescents
older than 6 years engage in:60 minutes or more of physical activity per day
Include aerobic & muscle- & bone-strengthening activities
75% of U.S. youth do not meet physical activity guidelines
Health benefits
– Lower risk excessive weight gain
– Improved bone health and weight status
– Improved cognitive function
– Improved quality of sleep
– Reduced symptoms depression and anxiety
Nutrients of Concern in Childhood
American children consume low levels of several
important nutrientsCalcium
– Important for bone health and optimizing bone massIron
– Supports growth and prevents iron-deficiency anemia
– Replaces iron lost through menstruation in adolescent girlsFiber
– Alleviates constipation
– Shown to reduce the risk of chronic diseasesVitamin D
– Crucial for skeletal health and optimal bone development
– Healthcare providers may recommend supplementation as
intake recommendation recently increased by 50%
Childhood Obesity
Prevalence has more than tripled since 1980
US children & adolescents (aged 2–19) 2017 - 2020
Almost 20% obese
Nearly 15 million obese
Childhood Obesity and Disease
• Obese children are at increased risk for multiple physical
and psychological problems:
– High blood pressure
– High cholesterol
– Type 2 diabetes
– Asthma
– Joint problems
– Fatty liver disease
– Psychological problems
– Negative stereotyping and bullying
– Obesity as adults
Factors of Childhood Obesity
Genetic
Overweight and obese parents
– Body’s ability to regulate appetite and satiety is overwhelmed by
conditions that influence decisions and food choice
Diet
– Energy-dense diets
– Larger portion sizesActivity
– Sedentary lifestyles
– Screen timeChildren ages 8-12 spend 4-6 hours a day
Teens spend up to 9 hours a day
Television and advertising appear to have negative effect on dietary quality
Socioeconomic
– Living at poverty level
– Living in food deserts
Preventing Obesity
National, state, and private programs are working to
reduce and prevent prevalence of childhood obesity
– Education
– Health-related legislation
– Food industry changesPrograms and initiatives
Alliance for a Healthier Generation
Robert Wood Johnson Foundation Healthy Children, Healthy Weight
National Heart, Lung, and Blood Institute: We Can!
Action for Healthy Kids
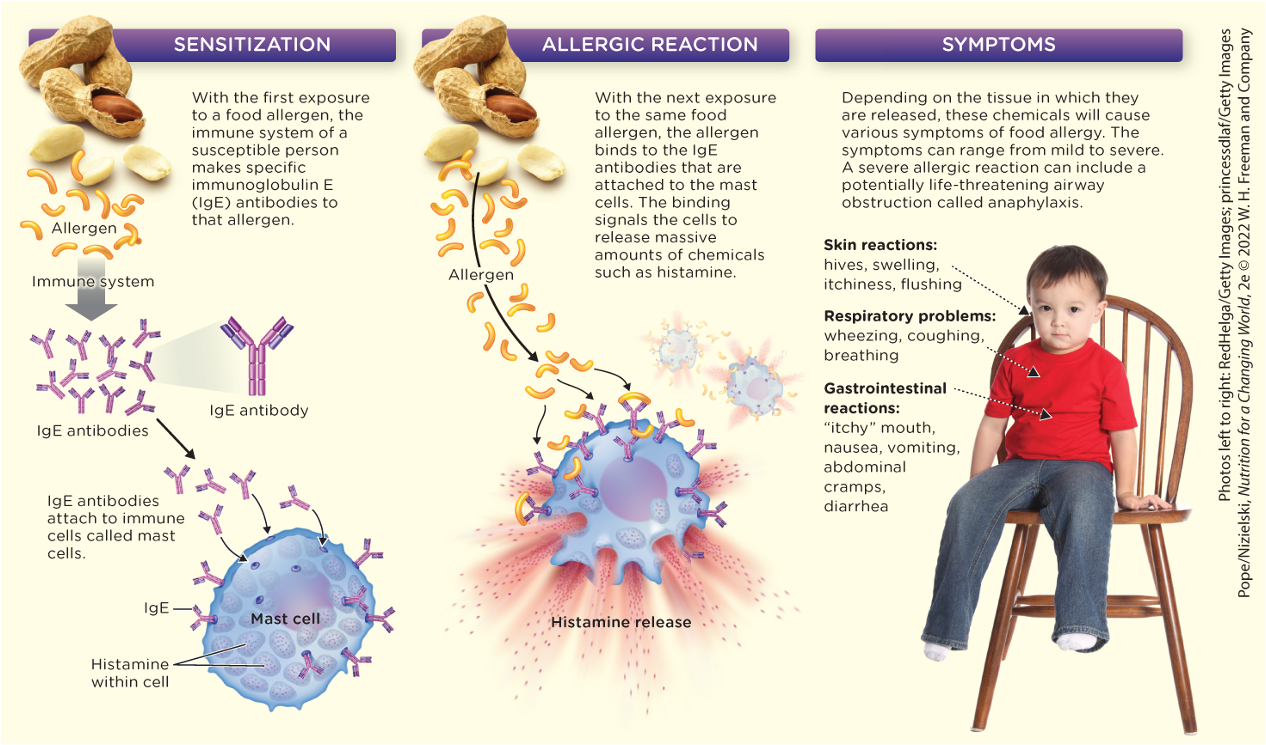
Food Allergies
Reproducible, adverse reaction to a food
Caused by an immune response to an allergen
Number of people with food allergies is growing without
a clear reason whyCDC reported a 50% increase in food allergies in children
between 1997 and 2011Thought to affect as many as 7% of U.S. adults and 8% of
childrenOne in every 18 US children has a food allergy
Most Common Food Allergens
According to the CDC cause 90% of allergic reactions
Milk
eggs
Peanuts
shellfish
Fish
soy
Wheat
Tree nut
Why are they becoming more common?
Heightened awareness
Hygiene hypothesis
Changes in food manufacturing and processing
Inadequate intake of
Food Intolerance
A reproducible adverse reaction to food, that is not a direct result of an immune response
Celiac disease, lactose intolerance
Not usually life-threatening
Can induce allergy-like GI and respiratory symptoms
Food Allergies
Why are they becoming more common?
– Heightened awareness
– The hygiene hypothesis
– Changes in food manufacturing and processing
– Inadequate intake of certain nutrients may contribute to risk of food allergies in childrenVitamin D, omega-3 fatty acids, folate
– The timing of when foods are introduced to childrenDelaying introduction of allergenic foods may be detrimental
Food Allergen Labeling
Food allergies
– Not “cured”
– Managed by avoiding allergenFood Allergen Labeling and Consumer Protection Act of 2004
Manufacturers must declare presence of major food allergens on food packages
Tips to Minimize a Child’s Risk of Developing Food Allergies
From the Academy of Nutrition and Dietetics
Exclusive breastfeeding for at least four months
decreases the risk of atopic dermatitis, cow’s milk
allergy, and wheezing when compared to feeding infants cow’s milk-based formulaSoy formula does not seem to affect allergy risk
Solid foods should not be introduced before 4‒6 months of age
Delaying beyond this does not appear to be more protective
Avoiding common allergens such as fish, eggs, and peanuts during pregnancy, breastfeeding, or beyond 4‒6 months of age does not seem to be protective
Introducing Allergenic Foods during Infancy
2017 new guidelines issued advising early introduction of foods containing peanuts to infants to reduce risk of peanut allergy
Introduce to infants at high risk for peanut allergy as early as 4-6 months
While still receiving majority of calories from breastmilk and not receiving other solid foods
LEAP study showed that introducing peanut-containing foods to infants at high risk of the allergy was safe and led to an 81% reduction in subsequent peanut allergy
Consult with healthcare provider for guidance and possible in-office supervision
Keeping Kids with Allergies as Safe as Possible
Academy of Nutrition and Dietetics recommendations for parents of a child with allergy:
Read food labels carefully
Educate family members, caregivers, and teachers about their child’s allergy severity
Teach their child about the allergy at a young age
Consult with a registered dietitian to develop a healthy eating plan that avoids allergen