Psychopharmacology
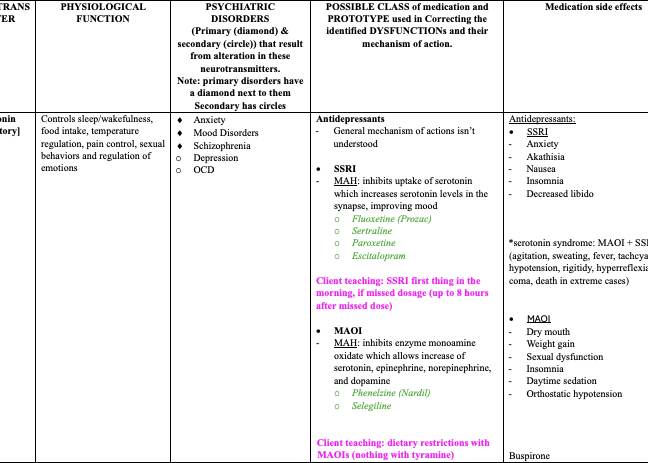
NEUROTRANS MITTER | PHYSIOLOGICAL FUNCTION | PSYCHIATRIC DISORDERS (Primary (diamond) & secondary (circle)) that result from alteration in these neurotransmitters. Note: primary disorders have a diamond next to them Secondary has circles | POSSIBLE CLASS of medication and PROTOTYPE used in Correcting the identified DYSFUNCTIONs and their mechanism of action. | Medication side effects |
Serotonin [Inhibitory]
| Controls sleep/wakefulness, food intake, temperature regulation, pain control, sexual behaviors and regulation of emotions | ¨ Anxiety ¨ Mood Disorders ¨ Schizophrenia o Depression o OCD
| Antidepressants - General mechanism of actions isn’t understood
· SSRI - MAH: inhibits uptake of serotonin which increases serotonin levels in the synapse, improving mood o Fluoxetine (Prozac) o Sertraline o Paroxetine o Escitalopram
Client teaching: SSRI first thing in the morning, if missed dosage (up to 8 hours after missed dose)
· MAOI - MAH: inhibits enzyme monoamine oxidate which allows increase of serotonin, epinephrine, norepinephrine, and dopamine o Phenelzine (Nardil) o Selegiline
Client teaching: dietary restrictions with MAOIs (nothing with tyramine)
Atypical Meds o Duloxetine o Venlafaxine o Bupropion o Mirtazapine o Venlafaxine o Trazadone
Client teaching (in general): safety measures (fall precautions, no driving, no alcohol)
Anxiolytics - MAH: partial agonist activity at serotonin receptors o Buspirone(long term management)
Client teaching: safety measures, avoidance of alcohol, no abrupt discontinuation
| Antidepressants: · SSRI - Anxiety - Akathisia - Nausea - Insomnia - Decreased libido
*serotonin syndrome: MAOI + SSRI (agitation, sweating, fever, tachcyardia, hypotension, rigitidy, hyperreflexia, coma, death in extreme cases)
· MAOI - Dry mouth - Weight gain - Sexual dysfunction - Insomnia - Daytime sedation - Orthostatic hypotension
Buspirone - Dizziness - Sedation - Nausea - headache |
GABA [inhibitory]
| Moderates other neurotransmitters | ¨ Anxiety o Schizophrenia o Mania o Huntington’s disease o Seizures | Anxiolytics · Benzodiazepines (short term) - MAH: binds to GABA receptors and increase GABA function o Alprazolam (Xanax) o Lorazepam o Chlordiazepoxide o Clonazepam o Diazepam
Client teaching: safety measures, avoidance of alcohol, no abrupt discontinuation
Anticonvulsants - MAH: increase levels of GABA o Carbamazepine (Carbatrol) o Divalproex (valproic acid & o Sodium divalproex) o Lamotrigine o Topiramate
| Anxiolytics - Respiratory depression - CNS depression - Death - Sedation - Tolerance
Anticonvulsants - Drowsiness - Sedation - Dry mouth - Blurred vision - Rashes, orthostatic hypotension (carbamazepine) |
Acetylcholine [Excitatory or inhibitory]
| Alertness of muscles, controls sleep and wakefulness cycle | ¨ Alzheimer’s Disease ¨ Dementia o Myasthenia Gravis
| Anticholinesterase & Acetylcholinesterase Inhibitors - MAH: prevent breakdown of acetylcholine o Donepezil (Aricept) o Rivastigmine o Memantine o Galantamine | Anticholinesterase/ Acetylcholinesterase Inhibitors - Nausea - Vomiting - Insomnia - Abdominal pain |
Dopamine [excitatory]
| Regulates emotional responses, motivation, cognition and can control complex movements | ¨ Parkinson’s Disease ¨ Schizophrenia o ADHD o Dementia
| Antipsychotic medications o MAH: Block dopamine receptors and reducing dopamine activity o First-generation (conventional - old): chlorpromazine, fluphenazine, thioridazine, o haloperidol, loxapine. o Second-generation (atypical): clozapine, risperidone, olanzapine, quetiapine. o Third-generation (dopamine stabilizers): aripiprazole.
Client Teaching: Adherence, side effect management, actions for missed doses. (within 4 hours)
Stimulants o MAH: block reuptake of various neurotransmitters and promote release of neurotransmitters from the presynaptic nerve terminals o Methylphenidate (Ritalin) o amphetamine, o dextroamphetamine o Disulfiram o Modafinil Client teaching: dose after meals, avoidance of caffeine, sugar and chocolate, proper storage and out of reach of children
((client teaching (disulfiram) – avoidance of alcohol, including products that contain shaving cream, deodorant, OTC cough medications | Antipsychotics: - Dystonia (acute rigidity and crampings, stiff/thick tongue) (treatment: anticholinergic drugs or diphenhydramine) - Pseudo parkinsonism (stooped posture, masklike facies, shuffling gait) - Akathisia (restlessness, anxiety and agitation_ - Neuroleptic malignant syndrome (high fever, delirium, diaphoresis, pallor, high unstable BP) (treatment: stop all antipsychotics) - Tardive dyskinesia (involuntary movements) – irreversible (need to know time fram of start of sxs) - Anticholinergic side effects (dry mouth, hypotension, urinary retention, dry eyes) - Weight gain - Increases blood prolactin levels - Metabolic syndrome
*agranulocytosis (clonzapine)
Stimulant - Anorexia - Weight loss - Nausea - Irritability - Dizziness - Dry mouth - Blurred vision - Palpitations
Disulfiram - Fatigue - Drowsiness - Halitosis - Tremoir - Impotence - Drug interactions with phenytoin, isoniazid, warfarin, barbiturates, long-acting benzos |
Norepinephrine (adrenaline) [excitatory]
| Mood, sleep and wakefulness, learning and memory, causes changes in attention | ¨ Depression ¨ Anxiety o Mania o Schizophrenia o BPD (mood stabilizer)
| Antidepressants · TCAs (Cyclic) - MAH: block the reuptake of norepinephrine primarily o Amitriptyline (Elavail) o Imipramine o Desipramine o Nortriptyline Client teaching: TCA at night, if missed dosage (up to 3 hours after missed dose)
SNRI’s - Duloxetine (Cymbalta)
Mood Stood Stabilizers - MAH: normalizes /blocks reuptake of certain neurotransmitters (lithium specifically) o Lithium (Lithane) o some anticonvulsants (carbamazepine, valproic acid; gabapentin, topiramate, oxcarbazepine, and lamotrigine) Client teaching: periodic monitoring of blood levels (12 hours after last dose), take with meals, safety measures | Cyclic Antidepressants - Dry mouth - Constipation - Weight gain - Sedation - Orthostatic hypotension - Tachycardia
Mood Stabilizers (Lithium) - Mild nausea - Anorexia - Polydipsia - Polyuria - Fatigue - Lethargy - Acne - Diarrhea - Weight gain
Toxic effects of mood stabilizers(lithium) - Severe diarrhea - Vomiting - Drowsiness - Muscle weakness - Renal failure - Death
Carbamazepine and valproic acid: - drowsiness, sedation, dry mouth, blurred vision (stevens-Johnson syndrome) Carbamazepine: - rash, orthostatic hypotension Valproic acid - weight gain, alopecia, hand tremor Topiramate: - dizziness, sedation, weight loss |