Module 10: Bonding to Enamel + Dentine
Historical Background
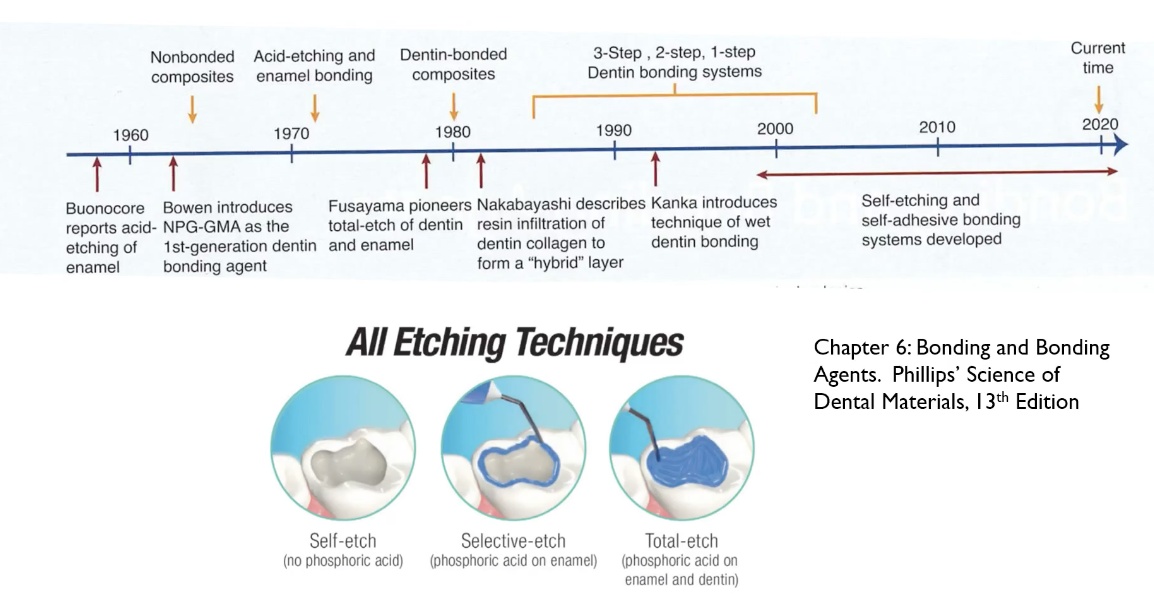
In 1949: development of first dental adhesive for dentine: contained glycerol phosphororic acid dimethacrylate
con: faced interfacial stresses bc of high polymerization, shrinkage stress and high thermal expansion, partly due to unfilled methacrylate resin
In the 1950s: Michael Bonnacore discovered that phosphoric acid was able to etch enamel
modern is less concentrated
leaves a durable micro=mechanical retentive interface with resin base, cements and restorative materials
Late 1970s: Fukayama pioneered total etch system
etch both enamel and dentin
concern: etching dentin can lead to sensitivity
however, the seal of the restoration is more important than sensitivity
1980s: Nakabayashi
described resin infiltration of dentin collagen to form a hybrid layer
with etching, we removed a lot of the inorganic components (calcium + phosphate) leaving collagen exposed
he described the penetratuon of the resin monomers with this area as a “hybrid layer”
Over the next 20 years:
dentin bonding agents and systems progressed
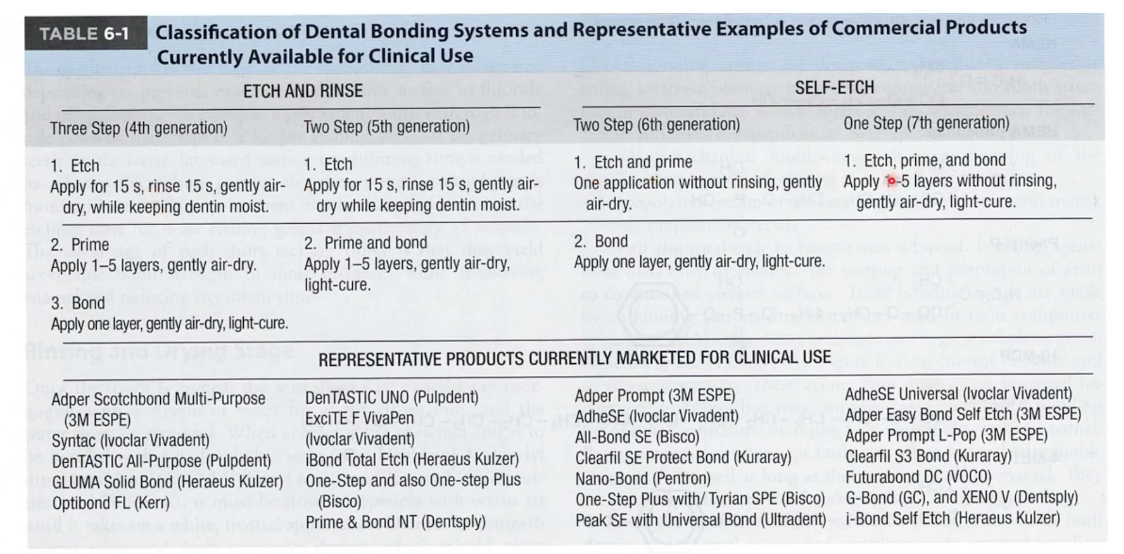
3-step, 2-step, 1-step systems
Mid 90s: Canker
Introduced technique of wet dentin bonding
emphasis on ensuring that the area where dentin etching is not desiccated
keep moist in order for prevent collapse of dentin collagen fibrils and maintain space for penetration + entanglement of resin monomer
Last 20 years:
self-etching and self-adhesive systems
Adhesion:
mechanism of adhesion
fundamentally an exchange of hydroxy-apatite with synthetic resins at tooth surface
remove hydroxyapatite crystals to create micro pores
allowing subsequent polymerization
Adhesive bonds are dependent on
surface energy, contact angle, wettability
adhesive needs to spread over the surace of the prepared tooth surface
need to displace any air pockets and penetrate by capillary attraction into microscopic and sub microscopic irregularities
wettability of any liquid on a solid is defined by the contact angle that forms between the liquid and solid
no wetting = contact angle 180 degrees
absolute wetting = 0 degrees
interpenetration
resin tags form and lock to interpenetrate hard tissue
micromechanical interlocking
penetration of enamel surface in the irregularities created by etching
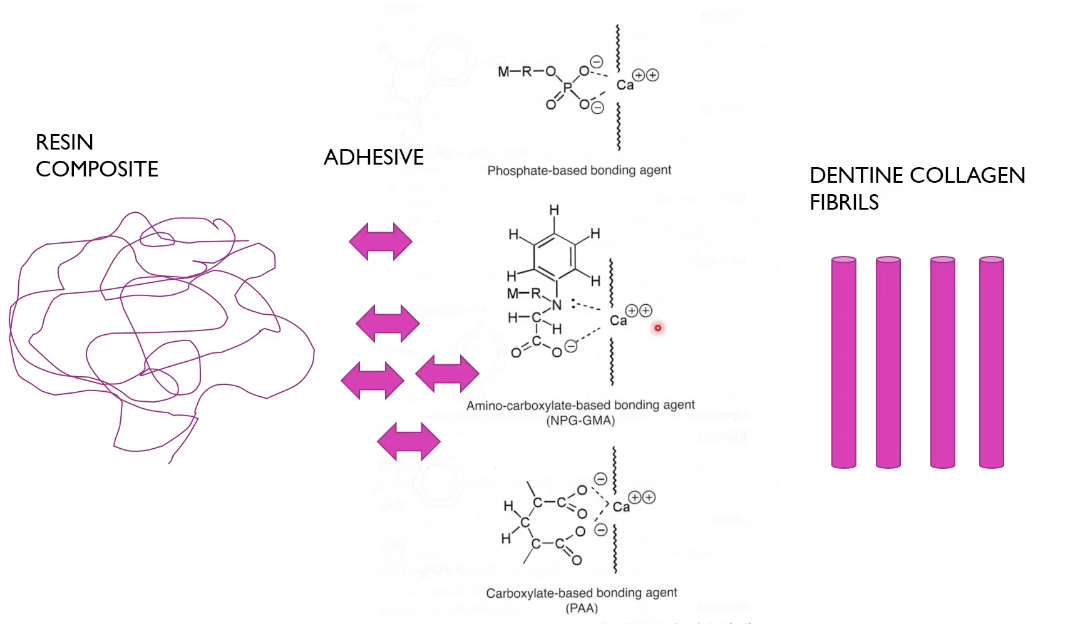
chemical bonding
achieved when acidic monomers with phosphate or carboxyl group potentially forms chemical bond with calcium in the tooth surface
Acid Etching
Enamel etching
removes smear layer 10 microns of enamel surface to expose enamel rods
allows resin monomers to readily wet the surface = better infiltration of mnomers into micropores which polymerize to form resin tags 6 microns in length + 10-20 microns in length
Fukayaama introduced total etch
Nakabayashi demonstrated the ability of hydrophilic resin to infiltrate the layer of demineralized collagen fibres + form hybrid layer
Should see a frosty white surface after drying etched surface
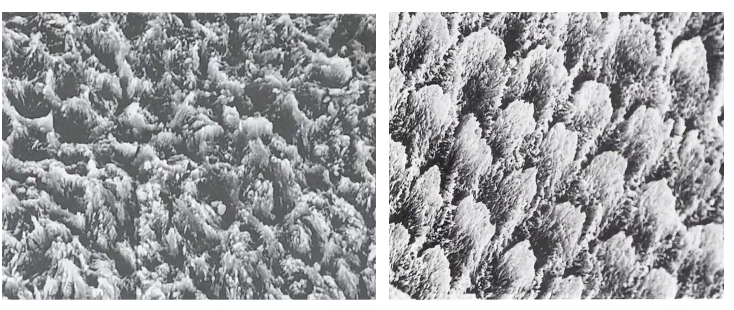
honeycomb surface with high surface enrgy increase the potential for wettability with resin
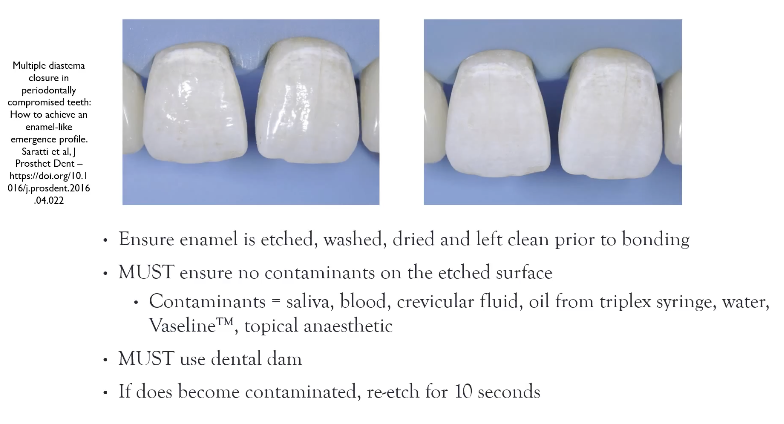
dam cuff should be inverted to prevent contamination
If you have used Vaseline on patients' lips or topical anaesthetic like Xylocaine ointment that has glycerin, which can also reduce your bone strength on your etched enamel.
If there’s any contamination: re-etch for 10 sec and rinse
This step is also useful to make sure you’ve removed all previous restoration resin bc you won’t see white frosting
bond to enamel with resin composite is reliable bc it exceeds 37 megapascals (of pressure)
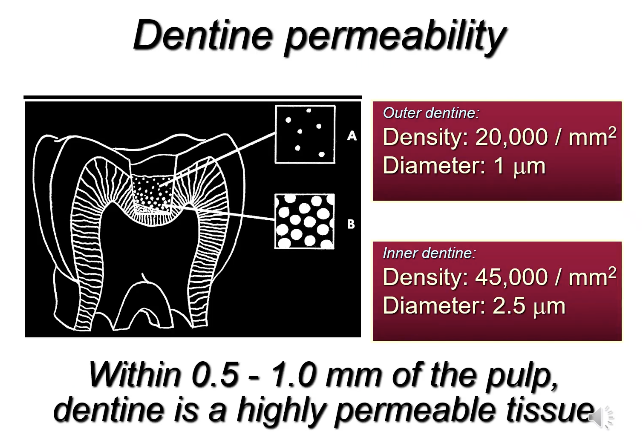
dentin is different because of tubules
outer dentin has 20 000 tubules within a square millimetre of dentin
diameter of tubule lumen = 1 micron
deeper dentin has 45 000 tubules/mm
diameter increases
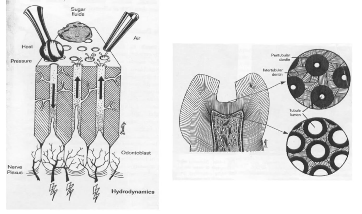
Hydrodynamic theory: heat pressure from a burr will get movement of the dentinal fluid back into the pulpal area
Drying the cavity, eating sweet things, breathing in quickly, outward movement of the fluid within tubules occurs
fluid is derived from odontoblasts which sit in the pulpal chamber + have odonto odontoblastic processes which extend into tubule
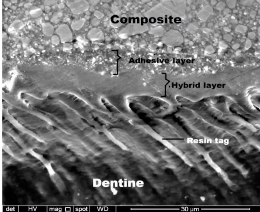
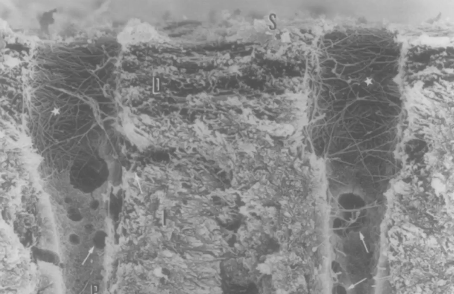
longitudinal section of dentin tubules
above is the adhesive layer
distinguished from resin composite restorative material on top, which has granular components which are the fillers in the resin composite
adhesive or bonding agent has visibly less fillers in order to be of lower viscosity to enable entanglement and impregnation of the collagen fibrils after etching
lower half extensions of polymerized resin tags extending into tubules + middle of image is the hybrid layer
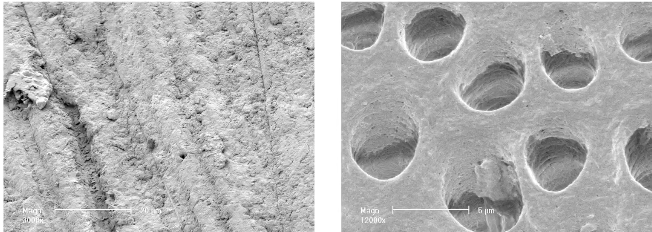
left is covered by a smear layer
right has smear layer removed
smear layer consists of organic and inorganic debris such as bacteria, hydroxyapatite crystald or collagen bundles
generated by mechanical cutting + shattering on the surface of dentin from the use of hand instruments
thickness of a smear layer has been reported to be as thin as 0.5 to 10 microns
smear layer is loosely attached to dentin surface
longitudinal section of dentin that’s been etched w/ smear layer
etch has removed hydoxyapatite from the dentin, peritubular dentin + walls of the dentinal tubule
orfices are lateral cannals that communicate the tubules w/ eachother
resin tags can form here
dentinal tubular fluids
concentration of acid in primer is highest at the top and gets lower
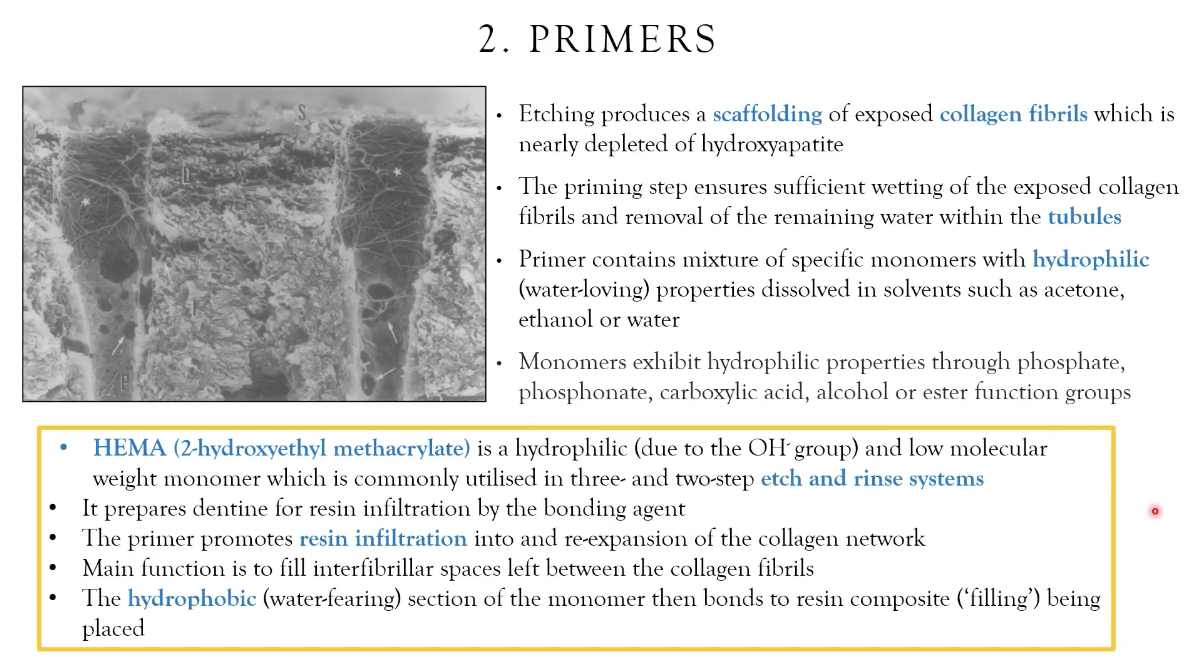
priming ensures sufficient wetting of exposed collagen fibrils + removal of water from dentinal tubule
wetting causes impregnation of the resin in the tubules + removing water helps
low molecular weight = popular, easily distributed
if collagen fibres collapse, it reduces entanglement
squiggly line = collagen surface
forms bonds with calcium
these bonds form during priming
solvents removed by gently blow-drying, too hard desiccates + collapses collagen
dentine surface is hydrophilic
resin material is hydrophobic
What happens to the hybrid layer over time?
Hybrid layer is susceptible to water sorption, hydrolytic degradation and resin leaching
Enzyme Inhibitors:
thus longevity of adhesive interface is increased when nonspecific enzyme-inhibiting strategies are used such as:
chlorhexidine
benzalkonium chloride
These inhibitors are used in therapeutic primers, W in the resin bonds
Future Direction:
may focus on reducing collagen degradations
increasing extent of collagen cross-linking prior to application of adhesive
carbodiimide, glutaraldehyde, proanthocyanidin
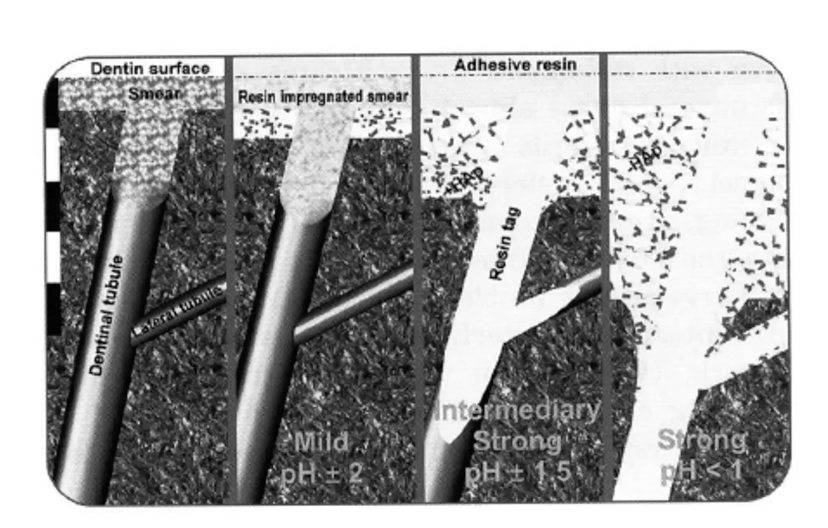
on the left, dentin has smear layer + smear plug
self-etch with mild primer (2) + resin impregnated smear
stronger intermediary = remove smear + plug
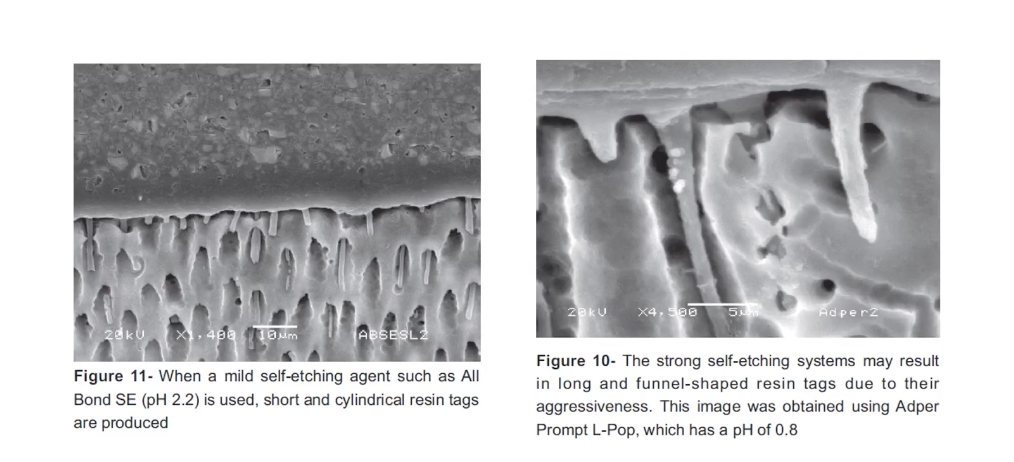
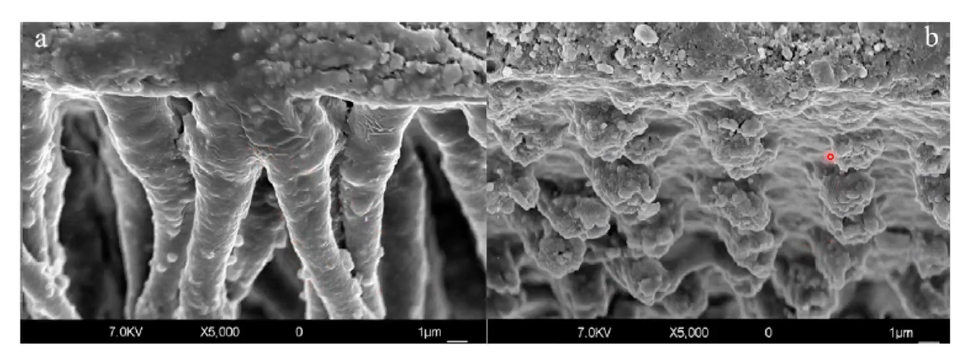
with etch and rinse, more of the smear layer has been removed
resin tags are more extensive w/ a funnel shape
self-etch not as effective bc not as much smear removed and less extensive resin tags
Clinical Performance:
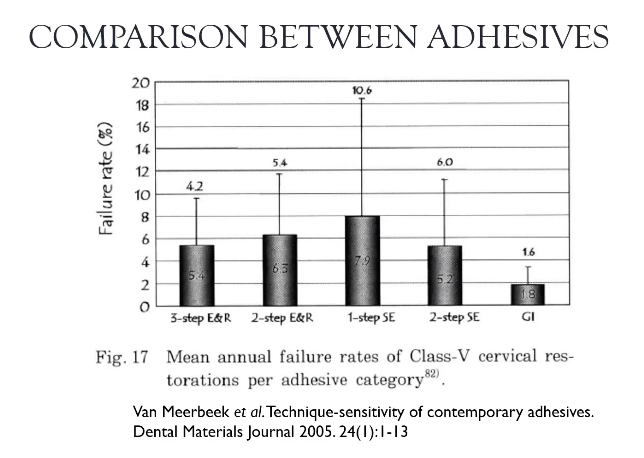
three-step etch-rinse adhesives and two-step self-etch adhesives show clinically reliable and preditably good clinical performance
two-step etch-and-rinse adhesives were less clinically effective
ineffecient clinical performance was found for one-step self-etch adhesives
cervical restorations placed with an etch-and-rinse adhesive shower higher retention than an all-in-one adhesive
clinical evaluation of different adhesives used in restoration of non-carious cervical lesions: 24 month results

Class Notes:
Etch:
rinse etch w same amount of time etch sat
dry thoroughly = white frosty appearance
if not, there are contaminates or previous resin
why is hydrophilic resin important?
dentinal fluid from odontoblasts
don’t dessicate bc collagen fibres collapse + prevent entanglement
want a hybrid layer to form (demineralized collagen + infiltrated resin) - nakabayashi
primer has an acid + has an etchant itself
maintain the smear layer (primer modifies the smear layer while making sure to expose too much collagen fibres)
etch activates enzymes that are imbedded into dentin (can disintegrate collagen)
collagen is wet so we need a hydrophilic component in bond, and resin
when placing primer, don’t dessicate (gentle airdry)
primer on dentin for 20s, modifies the smear layer, gently agitate to remove solvents (or airdry)
place bond, blow to thin layer + remove air bubbles
light cure, then place resin
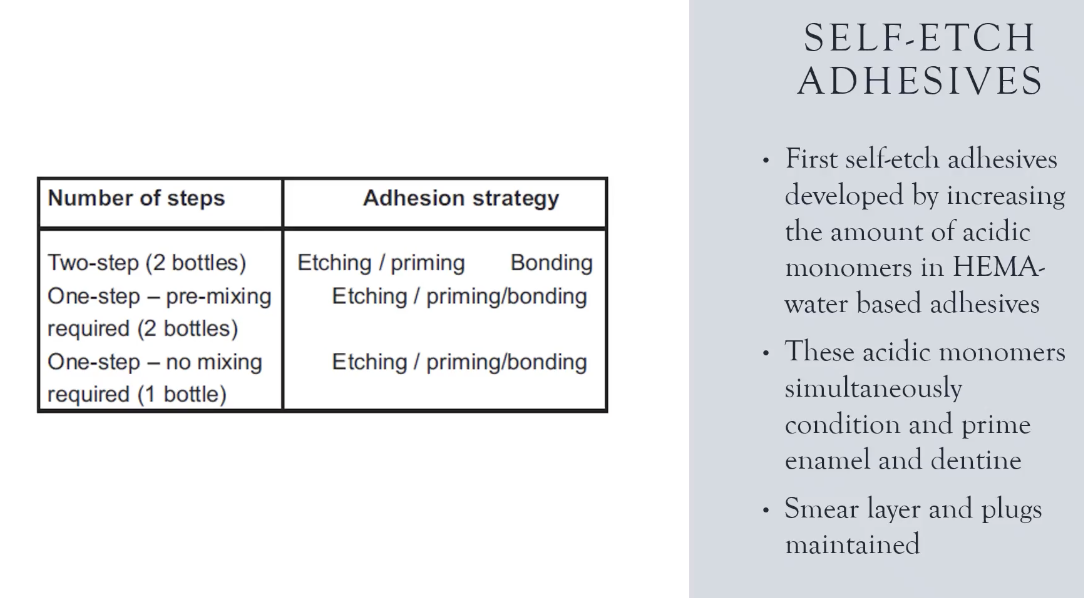
Self-etch adhesive systems combine etching and priming into one step
these principals apply to cementing crowns, bridges, other appliances
Primer:
funnel shape of dentinal tubule because the etchant concentration lowers the further down you go
orfices in the dentinal tubule allow resin to seep in?
entangle + impregnate
bc of liquid from dentinal fluid, fluid is similar to interstitial fluid makes it difficult for resin to enter (causes outwards pressure)
fluid in dentinal tubule would be reduced with adrenaline from local anaesthetic
hybrid layer should be stable
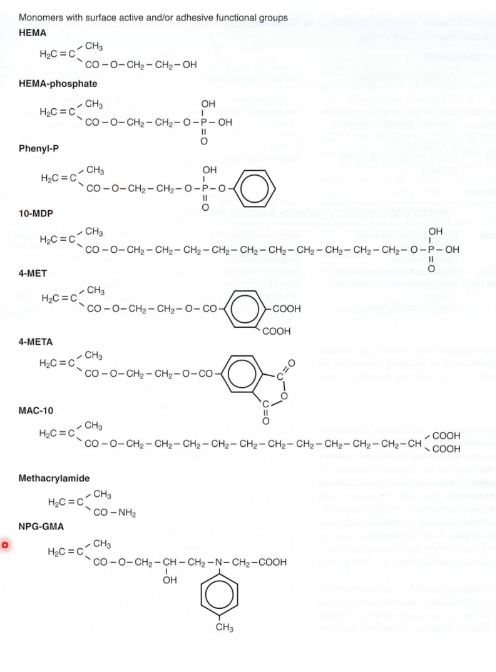
discovery of having HEMA as hydrophilic substance in two step etch and rinse
hydrophobic part of HEMA binds with the resin (interface)
Solvents:
water, ethanol, acetone
water ionizes the acidic monomers as well as expand the collagen network
conditioning the collagen fibres upright to encourage entanglement
ethanol and acetone have water chasing properties to penetrate the tubules
REMOVE SOLVENT
after primer, use microbrush to agitate to evolve the solvent + use for 20 sec + air dry
place bond/adhesive + form interface between collagen fibres + resin composite
3-5% of resin undergoes polymerization shrinkage (leaves a gap between tooth + restorative material)
resin may also pool onto hybrid (causes pulling away from dentin)
flowable composite tends to pool
pulsing cure light allows periods of relaxation and curing
Bond:
bond is intermediary layer between tooth + resin composite
fill interfibrular space + form resin tags
adhesive needs to be both hydrophobic and hydrophilic
resin is hydrophobic
dentinal tubules are hydrophilic
Initiators:
champoroquinone is a photoinitiator
self cure systems exist aswl (may not be able to light cure smtms)
extremely deep cavity
crown
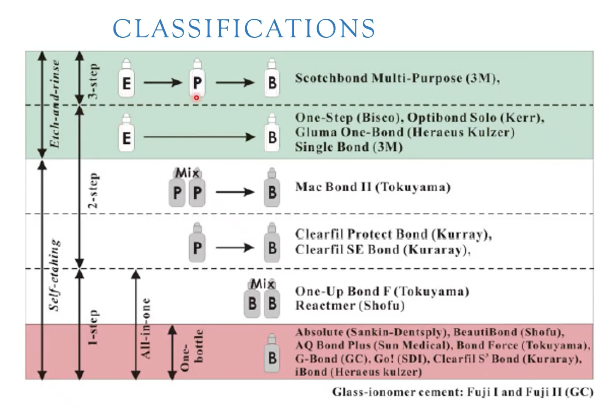
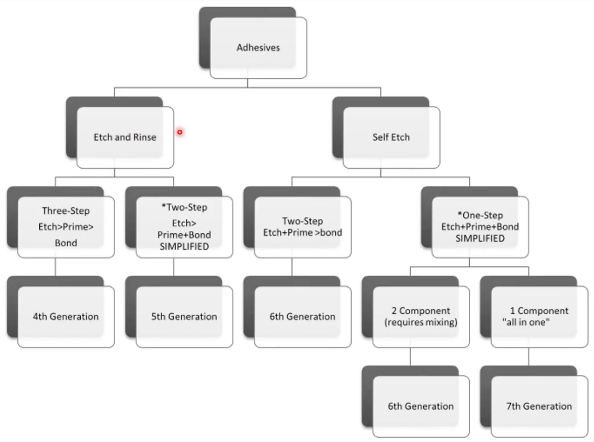
Classifications:
image in slides