5.7 - Introduction to Rheumatology
LECTURE NOTES
RHEUMATOLOGY
Medical speciality dealing with diseases of musculoskeletal system
Includes dealing with bones, joints, muscles, tendons and ligaments
There is particular emphasis on diagnosis and treatment of autoimmune joint and connective tissue diseases
Arthritis is a disease of the joints.
Many types of arthritis but there are two major divisions
Degenerative joint disease (osteoarthritis)
Inflammatory joint disease
This is important because the treatment for the different types of arthritis are different
DEGENERATIVE JOINT DISEASE: OSTEOARTHRITIS
Pathological changes cartilage loss and bony remodelling
Epidemiology
More prevalent with age
Previous joint trauma (e.g. footballer’s knees)
Jobs involving heavy manual labour
Gradul onset - slowly progressive disorder
Symptoms and Signs
Joint pain - worse with activity and better with rest
Joint crepitus - creaking, cracking grinding sound on moving affected joint
Joint enlargement - e.g. Heberden’s nodes (bony swelling at the DIP joints are termed as Heberden’s joints)
Limitation of range of motion
Joints affected are usually
Joints of the hand
Distal interphalangeal joints (DIP)
Proximal interphalangeal joints (PIP)
First carpometacarpal joint (CMC)
Spine
Weight bearing joints of lower limbs
Especially knees and hips
First metatarsophalangeal joints
Radiographic features
Joint space narrowing
Subchondral bony sclerosis
Ostephytes and subchondral cytes
INFLAMMATORY JOINT DISEASE
Inflammation - physiological response that helps us deal with injury or infection
Excessive/inappropriate inflammatory response reactions can damage the host tissues
Clinically manifests with: Redness, pain, heat, swelling and loss of function
Physiological, cellular and molecular changes:
Increased blood flow
Migration of leucocutes into tissues
Activation and differentiation of leucocytes
Cytokine production
TNF-alpha
Causes of inflammation
Infection → septic arthritis and tuberculosis
Crystal arthritis → gout and pseudogout
Immune mediated → rheumatoid or seronegative arthritis and systemic lupus erythematosus (SLE
First two are secondary and immune mediated is primary
First is non-sterile and second 2 are sterile
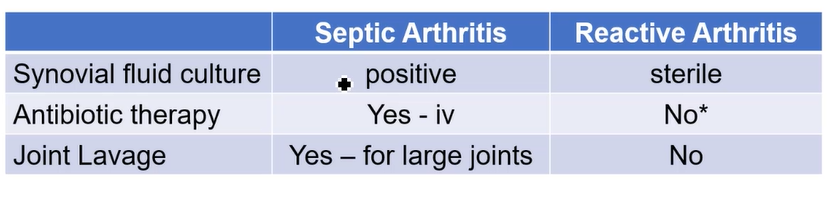
Septic Arthritis
Bacterial infection of a a joint (usualy caused by spread of blood)
Risk factors → immunosuppressed, pre-existing joint damage, intravenous drug use
Septic arthritis is a medical emergency
Untreated, the bacteria can rapidly destroy the joint
Clinical presentation
Acute, red hot painful swollen joint
Usually only 1 joint is affected (monoarthritis)
Typically fever: patient is often systemically unwell
Consider septic arthritis in any patient with an acute painful, red, hot, swelling of a joint especially if there is a fever
Diagnosis is done by joint aspiration and send sample for urgent gram stain and culture
Common organisms: staph. aureus, streptococci and gonococcus (more rare)
Gonococcal septic arthritis is an exception as it is polyarthritis and is less likely to cause joint destructure
Treatment is with a surgical wash-out (lavage) and
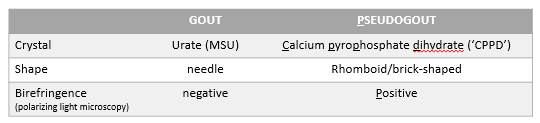
Crystal Arthritis
Two main types - gout and pseudogout
Gout
Caused by deposition of monosodium urate (MSU) crystals around the joint
Tissue depositions of MSU normally cause gouty arthritis or tophi
Tophi are aggregated deposits of MSU in tissue and often develop around hands, feet, elbows and ears
High uric acid levels (hyperuricaemia) is a risk factor gor gout
Causes for hyperuricaemia → genetic tendency, increasing intake of puring rich foods or reduced excretion e.g. due to kidney failure
Clinical features:
Abrupt onset
Usually monoarthritis
Big toe 1st MTPJ (metataophalangeal joints) most commomly affected
Investigations
Bloods: high c-reactive protein and high serum urate
X-rays - usually normal initially. If recurrent attacks/long-standing gout, juxta-articular erosions can develop
Joint aspiration and synovial fluid are best for definitive diagnoses
Pseudogout
Caused by deposition of calcium pyrophosphate dihydrate (CPPD) crystals which cause inflammation
Risk factors: background osteoarthritis, elderly patients, intercurrent infection
Joint aspiration and synovial fluid analysis
Key investigation for any acute monoarthritis
Needle inserted into the joint and fluid is aspirated
Fluid is sent to lab for
Microbiology (gram stain, culutre and sensitivities)
Polarising light microscopy to detect crystals
Gout Treatment
Acute attack - reduce inflammation
Non-steroidal anti-inflammatory drugs (NSAIDs)
Glucocorticoids (steroids)
Chronic - need to reduce uric acid levels
Lifestyle - avoid purine rich food, beer
Pharmacological: allupurinol, febuxostat (xanthine oxidase inhibitors)
IMMUNE MEDIATED INFLAMMATORY JOINT DISEASE
Autoimmune - immune system attacks body’s own tissues - joint inflammation
3 main categories
Rheumatoid arthritis
Serognegative inflammatory arthritis
System lupus erythematosus (aka SLE or lupus)
Rheumatoid Arthritis
RA = chronic autoimmune disease
Primary site of pathology is in the synovium
Synovitis - inflammation of the synovial membrane
Synovium is found at
Synovial joints,
Tenosynovium surrounding tendons
Bursa
Chronic, polyarthritis
Common feature is early morning stiffness in and around joints
May lead to joint damage and destruction → joint erosion on radiographs
Auto-antibodies usually detected in blood
Extra-articular disease can occur
e.g. ocular inflammation, interstitial lung disease, nodules and vasculitis
Rheumatoid arthritis: pattern of joint involvement
Symmetrical
Affects multiple joints (polyarthritis)
Affects small and large joints, but particularly hands, wrists and feet
Mostly affects (MCJPs, PIPJs, wrists, knees, ankles and MTPJs)
Pathogenesis
Healthy synovial membrane contains macrophage like (type A) and fibroblast like (type B synoviocyte) cells, type I collagen and maintenance of synovial fluid
In RA synovium becomes a proliferated mass of tissue due to
Neovascularisation
Lymphangiogenesis
Inflammatory cells (activated T and B cells, plasma cells, mast cells, activated macrophages)
Recruitment activation and effector functions of these cells is controlled by a cytokine network
Excess of pro-inflammatory cytokines compared to anti-inflammatory cytokine imbalance can also cause this
TNF-alpha: cytokine tumour necrosis factor alpha, is the dominant pro-inflammatory cytokine in the rheumatoid synovium
Its pleotropic actions are detrimental in this setting
Dominant detrimental role of TNF-alpha in rheumatoid arthritis validated by the therapeutic succes of TNF-alpha inhibition
TNF-alpha inhibition is achieve via vintravenous infusion or sub-cutaneous injection of antibodie or fusion proteins
Blood Test: RA vs OA and SA
Haemoglobin - decreased or normal in RA, normal in OA and SA
Mean Cell Volume - normal for RA, OA and SA
WCC is usually normal in RA, normal in OA but increased (leucocytosis in SA)
Platelet count is normal or high in RA and SA but normal in OA
ESR (erythrocyte sedimentation rate) is usually high in RA, normal in OA and normal or high in SA
C-reactive protein is high in RA, normal in OA and high in SA
Autoantibodies
Two types of antibodies are found in the blood of RA patients
Rheumatoid factor - antibodies that recognise the Fc protion of IgG as their target antigen
Positive in approximately 80% of RA patients
Can also be found positive in other conditions
Antibodies to citrinulated protein antigens (ACPA)
Clinicl test = anti-cyclic cirtrulinated peptide antibody anti-CCP antibody
Anti-CCP antibodies are more specific for RA than RF
Anti-CCP Ab positivity is associated with more aggressive/erosive diseases
Citrulination = post-translational modification where arginine gets converted to citrulline by PADs
X-Ray
Radiographic features of RA
Soft-tissue swelling
Peri-articular osteopeniai
Bony erosions - only occur in established disease. The aim of modern therapy is to treat early before erosions (permanent damage) has occurred
Essentially if you are finding out about this through the X-Ray then it’s probably too late.
Ultrasound
Much better for detecting synovitis
Synovial hypertrophy (thickening)#
Increased blood flow (Seen as doppler signal)
May detect early ersosions not seenon plain X-Ray
Ultrasound usually of hands and wrists can be performed alongside clinical assessmen in a dedicated early arthritis clinic
Principles of Management
Treatment goal: prevent joint damage
Requires
early recognition of symptoms, referral and diagnosis
prompt initiation of treatment, joint destruction = inflammation x time
aggressive pharmacological treatment to suppress inflammation
Pharmacological treatments
Glucocorticoid therapy - useful acutely but avoid long term use because of side-effects
DMARD's’ = disease modifying anti-rheumatic drugs
Immunomodulatory drugs that halt or slow the disease process
First line normally combination of anti-rheumatic drugs, typically methotrexate + hydroxychloroquine an sulfasalazine plus IM or short course of oral steroids
If disease still present we will escalate to one of the biological therapies like anti-TNF
Historically in the treatment of rheumatoid arthritis nonsteroidal anti-inflammatory drugs like ibuprofen or their stronger cousins like naproxen were used.
Less relevant now because they have long term renal damage and cardiovascular risks
RHEUMATOID VS OSTEOARTHRITIS
Age at onset: RA happens a bit younger
RA onset a lot quicker
RA is bilateral and symmetrical, OA is asymmetrical
Movement is better with RA
RA is common in wrist, ankle and elbow
Positive serolody seen with RA
Systemic symptoms seen with RA
Joint swelling is red, warm and effusion with RA, bony with OA
SERONEGATIVE INFLAMMATORY ARTHRITIS
Family of conditions with overlapping clinical features and pathogenesis
Unlike rheumatoid arthritis, rheumatoid factors and seronegative and CCP antibodies are not present in the blood, hence called seronegative
Still are autoimmune
Psoriatic Arthritis
Skin psoriasis assoiated with this arthritis
Scaly red plaques on extensor surfaces
10% of people with psoriasis will also have joint inflammation
Varied clinnical presentations
Classically presents as asymmetrical arthritis involving IPJs (interphalangeal joints)
Can also manifest as symmetrical involvement of small joints (rheumatoid pattern)
Oligoarthritis of large joints
Spinal or sacroiliac joint inflammation
Severity of skin not proporitonal to severity of joint disease
Reactive Arthritis
Sterile inflammation in joints following infection elsewhere in the body
Septic arthritis in the joint, reactive arthritis is an infection elswehere which causes inflammation to the other joint
Common triggers are urogenital or STIs or GI infections
Inflammation of tendon insertions, skin inflammations or ocular inflammations
Reactive arthritis is occasionally the first manifestation of HIV or Hep C
Genetic predisposition → young adults with HLA-B27 and environmental triggers such as salmonella infections
SLE (Systemic Lupus Erythematous)
Lupus = a multi-system autoimmune disease
Multi-site inflammation can affect almost any organ
Mainly affects joints, skin, kidneys, haematology, also lungs, CNS and cardiac involvement
Associated with antibodies to self antigens (autoantibodies)
Different autoantibodies to RA - instead of RF and CCP
Autoantibodies are antinuclear antibodies (ANA)
Sensitive to SLE not specific
A negative test rules out lupus but a positive test doesn’t solely mean Lupus
Other autoantibody is the Anti-double stranded DNA antibody (anti-dsDNA abs)
High specificity for SLE in the context of appropriate clinical sings
More common in females than males (9:1)
Presentation usually quite young 15-40 years old
Increasd prevalence in African and Asian communities