Maternity - Final
AROM vs SROM assessment of the fluid what are you assessing?
AROM = artificial rupture of membrane
intentional break of the amniotic sac using an amnihook
Done when cervix is favorable
SROM = spontaneous rupture of membrane
Amniotic sac breaking on its own NATUTALLY
Assessment of fluid:
COAT
Color of fluid
Odor - is there a smell
Amount - gush or trickle of fluid
Time - when did it break
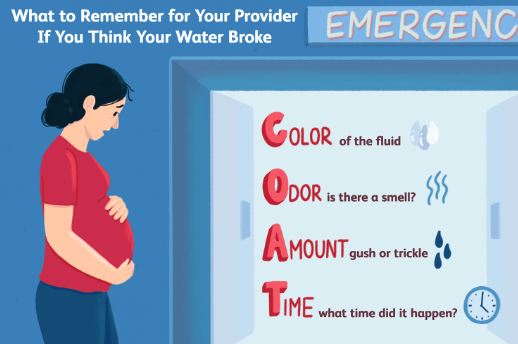
call provider regardless of if there are contractions or not
Put a pad on & bring a towel
Can shower but no swimming or baths
Have a packed bag for hospital → possible induction
Do not put anything in vagina
TPAL, Gravida, Parity
T = term
the number of pregnancies carried to 37 weeks or up
P = preterm
the number of pregnancies born between 20-36.6 weeks
A = abortion
number of losses before 20 weeks
L = living
the number of living children
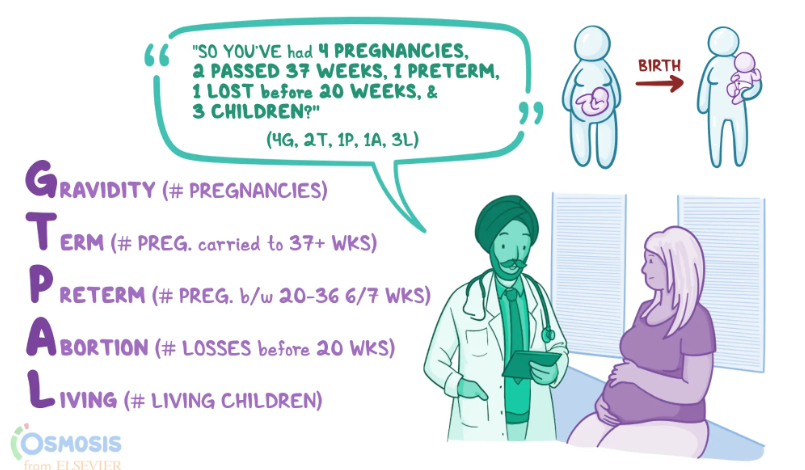
Gravity
# of pregnancies a mother has had
this includes losses
Nulligravid - never been pregnant
primigravida - 1st time EVER being pregnant
multigravida - been pregnant 2+ times
Parity
# of births after 20 weeks gestation
this includes losses after 20 weeks
SAB (spontaneous abortion) = BEFORE 20 weeks
nullipara - never given birth to anyone past 20 weeks
primipara - 1 birth after 20 weeks
multipara - 2+ births after 20 weeks
MULTIPLES (twins, triplets, etc. Count as ONE birth)
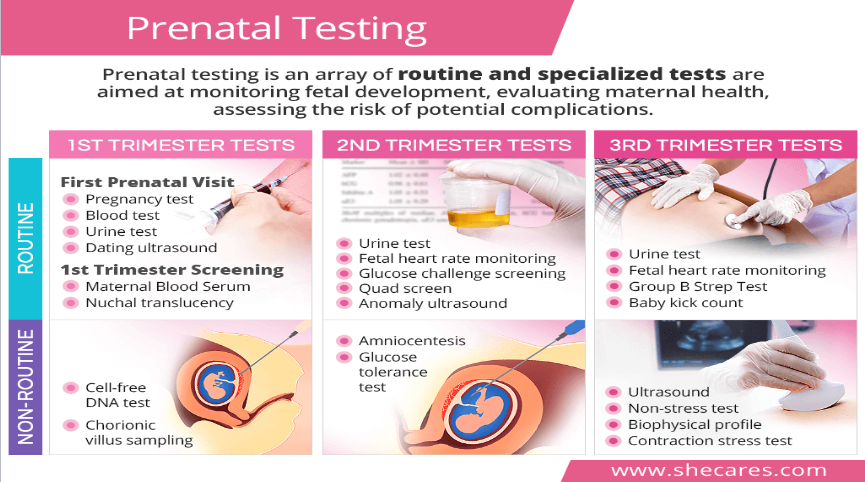
Prenatal testing
tests that monitor fetal development, evaluating mental health, assessing the risk of potential complications
1st trimester tests:
Routine:
first prenatal visit:
pregnancy test
blood test
urine test
dating ultrasound
first trimester screening:
maternal blood serum - screens for down syndrome, neural tube defects, or any other possible complications
nuchal translucency - measure fluid behind baby neck to determine any genetic or chromosomal abnormalities
Non-Routine:
cell-free DNA test - looks at fetal DNA in maternal blood to determine abnormalities
basically takes blood from mother to monitor fetal DNA
NONINVASIVE
chorionic villus sampling - determine birth defects
2nd trimester tests:
routine:
urine test
fetal heart rate monitoring
glucose challenge screening
quad screen - 4 screening for fetal anomaly
anomaly ultrasound - done by a radiologist not done by OBGYN
non-routine:
amniocentesis
glucose tolerance test
3rd trimester tests:
routine:
ultrasound
non-stress test
biophysical profile
contraction stress test
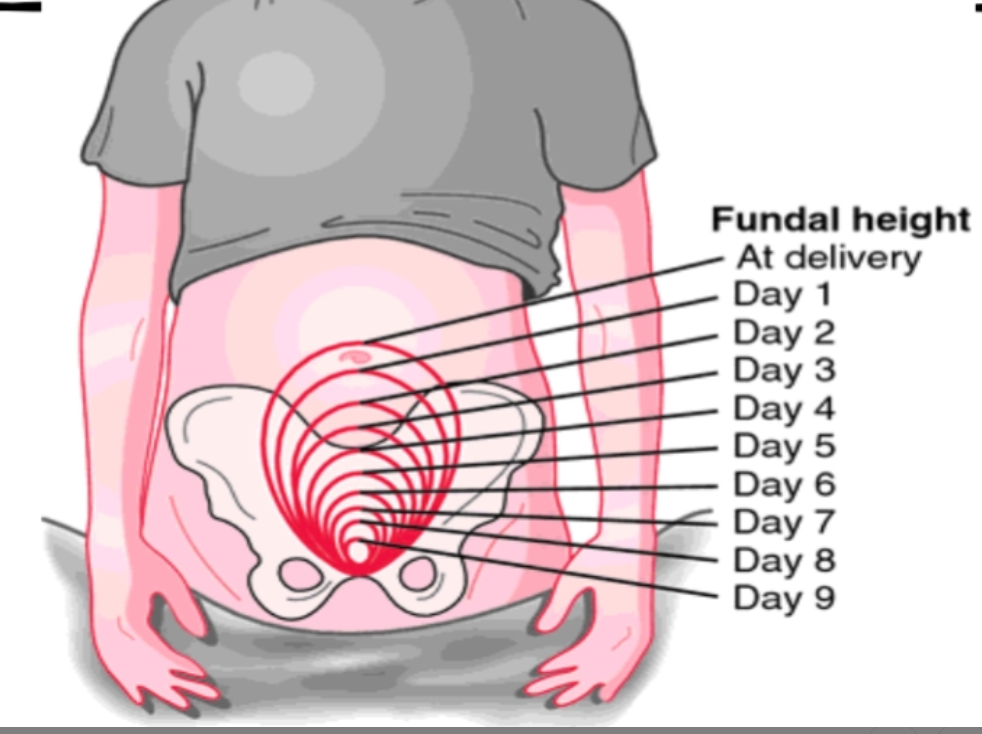
also measures fundal height
group b strep test - vaginal strep culture done near end of pregnancy & beginning of pregnancy
baby kick count - not done anymore
only done if mother says “I don’t feel the baby moving”
non-routine:
ultrasound
non stress test
biophysical profile
contraction stress test
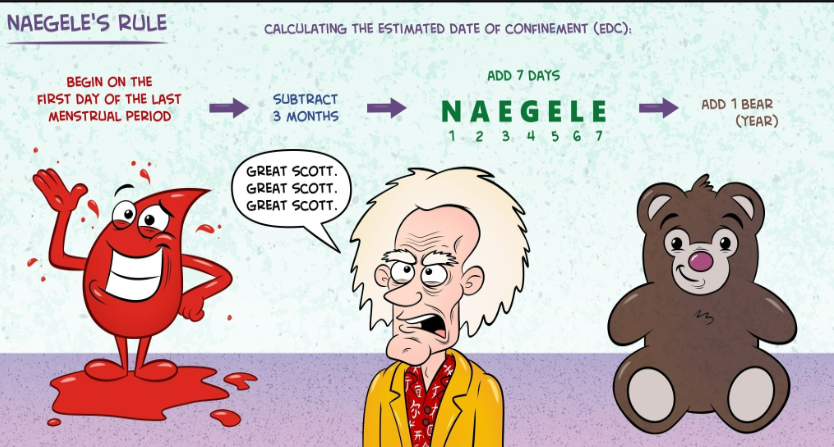
Full-term, preterm, trimesters, EDC
EDC = estimated date of confinement
Use NAEGELE’S rule
1. First day of last menstrual period (LMP)
2. Subtract/go back 3 months
3. Add 7 days
4. Add 1 year
Trimesters
1st trimester
Months 1-3
Weeks 1-13
2nd trimester
Months 4-6
Weeks 14-27
3rd trimester
Months 7-9
Weeks 28-40
Full term = 37-40 weeks of pregnancy
Preterm = born before 37 weeks
extremely preterm: <28 wks
very preterm: 28-31.6 wks
moderate preterm: 32-33.6 wks
late preterm: 34-36.6 wks
Immediate care of newborn, meds, apgar, reflex check, vital signs, typical weight, head circum, chest..skin-to-skin
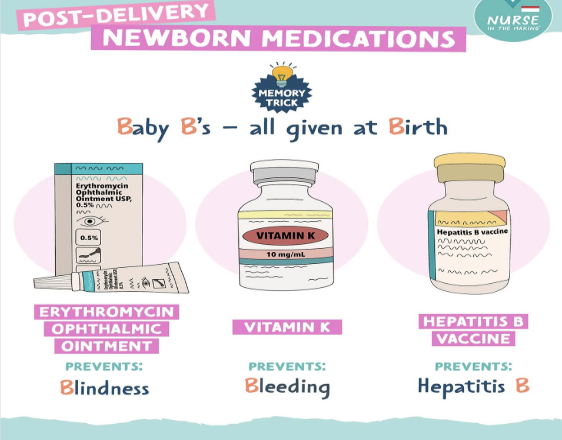
Medication
Vitamin K - babies do not make Vitamin K in the 1st 24 hours of life
Needed for blood coagulation.
Erythromycin eye - prevent against potential vaginal STD that could cause blindness
Hepatitis B vaccine - offered not mandated. Trying to eradicate this disease in the US.
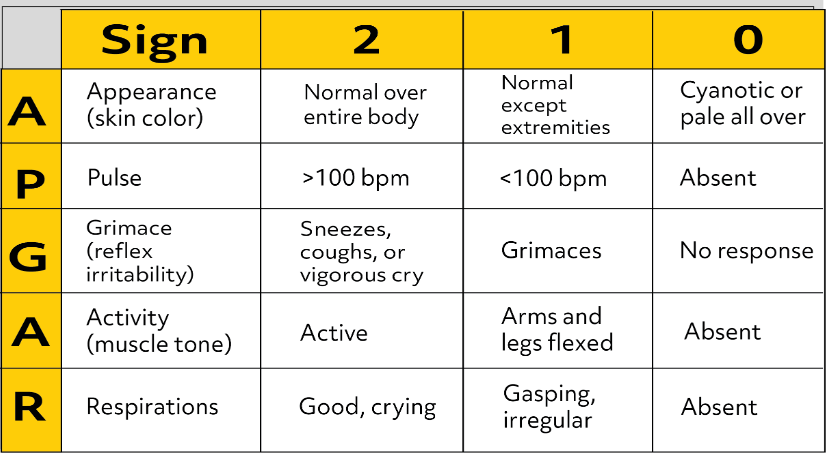
APGAR
Typical Weight
7.5 pounds
Average Head circumference
35CM
Average length
20 inches
Skin to skin contact (1st hour post birth)
uninterrupted time
quiet noises
dim lighting
keep baby skin to skin
delay baby checks
delay cord clamping
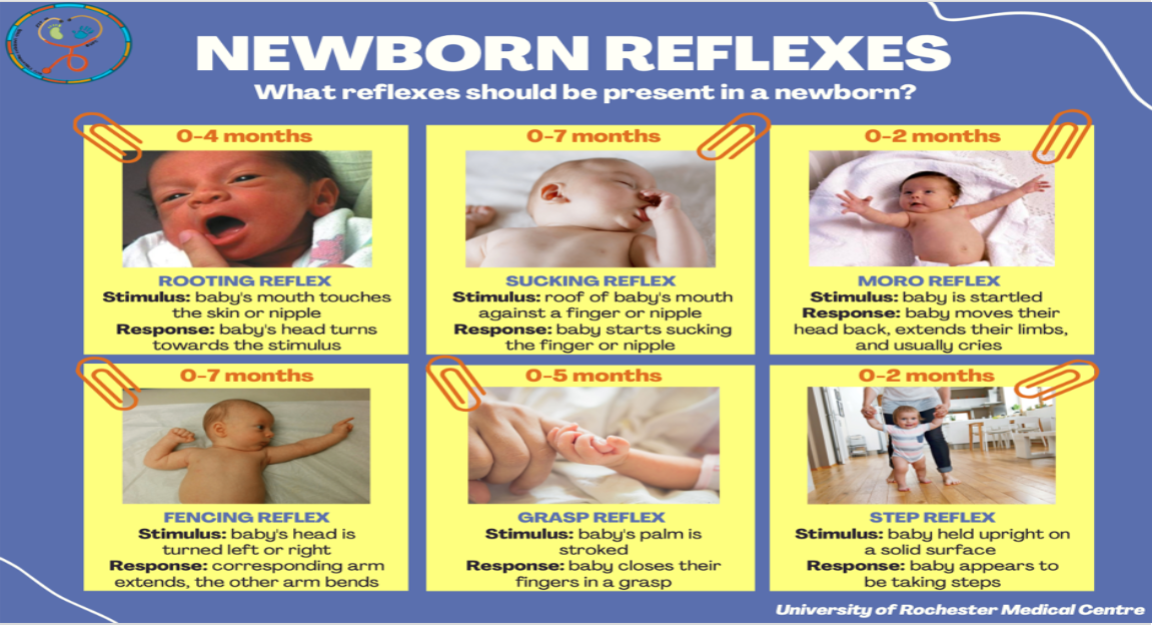
Newborn Reflexes
0-2 months
moro reflex
Stimulus: baby is startled
Response: baby moves their head back, extends limbs & usually cries
Step reflex
stimulus: baby held upright on a solid surface
response: baby appears to be taking steps
0-4 months
rooting reflex
stimulus: baby’s mouth touches the skin or nipple
response: baby’s head turns towards stimulus
0-5 months
grasp reflex
stimulus: baby’s palm is stroked
response: baby closes their fingers in a grasp
0-7 months
sucking reflex
stimulus: roof of baby’s mouth against a finger or nipple
response: baby starts sucking the finger or nipple
fencing reflex
stimulus: baby’s head is turned left or right
response: corresponding arm extends, the other arm bends
ex: the baby’s head is turned right
so the right arm is extended outward & left arm is bent
Vital signs
tips:
start w/ the least invasive VS first
check vital signs q4hr
room temp and clothing may alter temp readings
HR: 120-160 bpm/min
BP:
systolic: 60-80
diastolic: 30-45
Respiratory: 30-60
Temp: 97-100.3 F
axillary or rectal
SpO2:
1 min: 60-65%
2 min: 65-70%
3 min: 70-75%
4 min: 75-80%
5 min: 80-85%
10 min: 85-95%
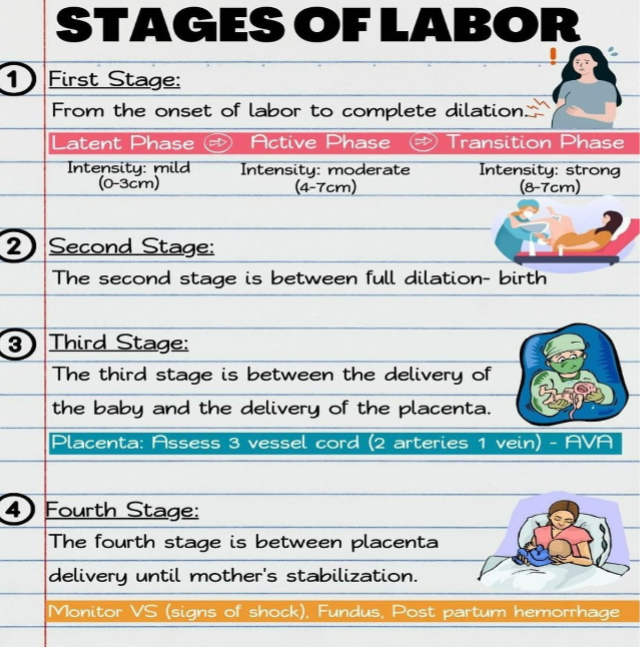
Stages of Labor
Stage 1 - the second you start dilating from 0 to 1 to 10 cm is DILATION
latent phase (or early)
from 0 to 4cm dilation (SEND MOTHER HOME OR WALKING IF THEY’RE NOT MORE THAN 4cm)
active phase
4-10cm dilated
Stage 2 - once mother reaches 10cm
stage 2 ends when WHOLE entire fetus comes out
Stage 3 - delivery of placenta
delivery of placenta AVERAGE takes 1min - 30 min
Stage 4: placenta delivery until mother is stabilized
monitor VS (vital signs) for signs of shock (every 15 minutes for an hour then every 30 minutes for an hour)
check fundus every 15 minutes to make sure she is not hemorrhaging
THESE STAGES WILL BE TIMED & GO INTO CHART
RDS, TTN
RDS = Respiratory Distress Syndrome
occurs within minutes after birth and is more common in infants less than 32 wks gestation
S/S:
noisy breathing grunting
retracting
nasal flaring
chest wall retraction
see-saw respirations
cyanosis
HR 150-180
tachypnea respirations greater than 60
breathing fast or slower than usual
fine inspiratory crackles
silver anderson score greater than 7
altered conscious state
feeding less, less wet nappies
head bobbing or sniffing position
tracheal tug sucking in at the neck
skin feels cool and clammy
treat the infection, CPAP, fluids, vasopressors, surfactant, cluster care glucose monitoring
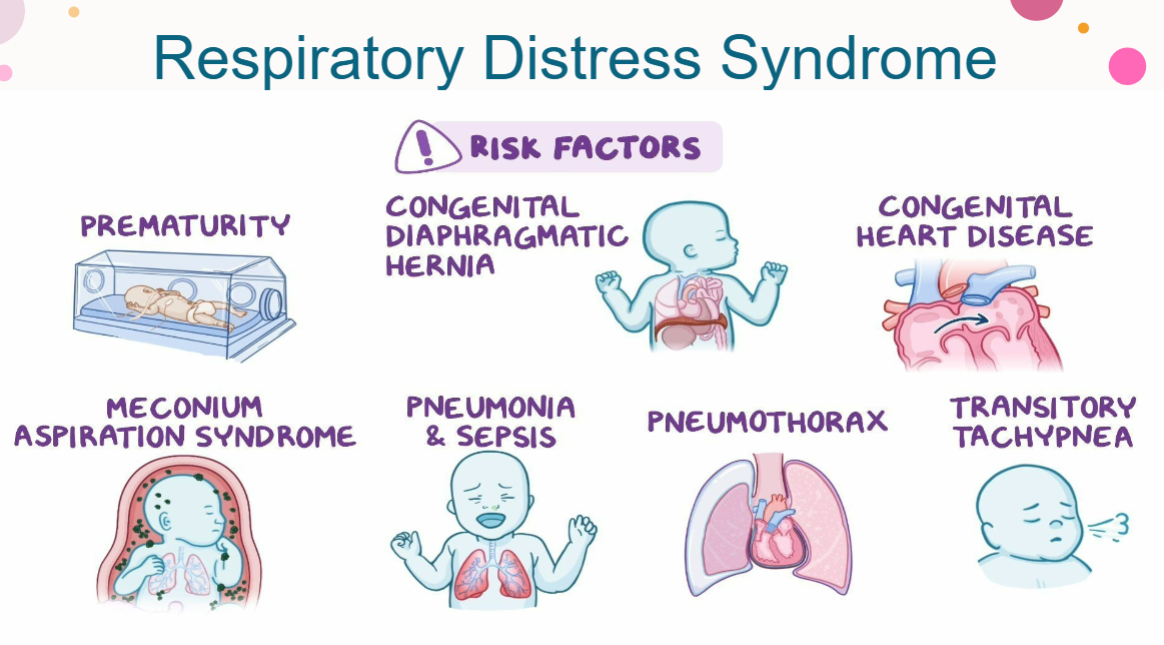
TTN = Transient Tachypnea of the Newborn
occurs with 35 and older infants that are born via c-section about 1-2 hrs after birth
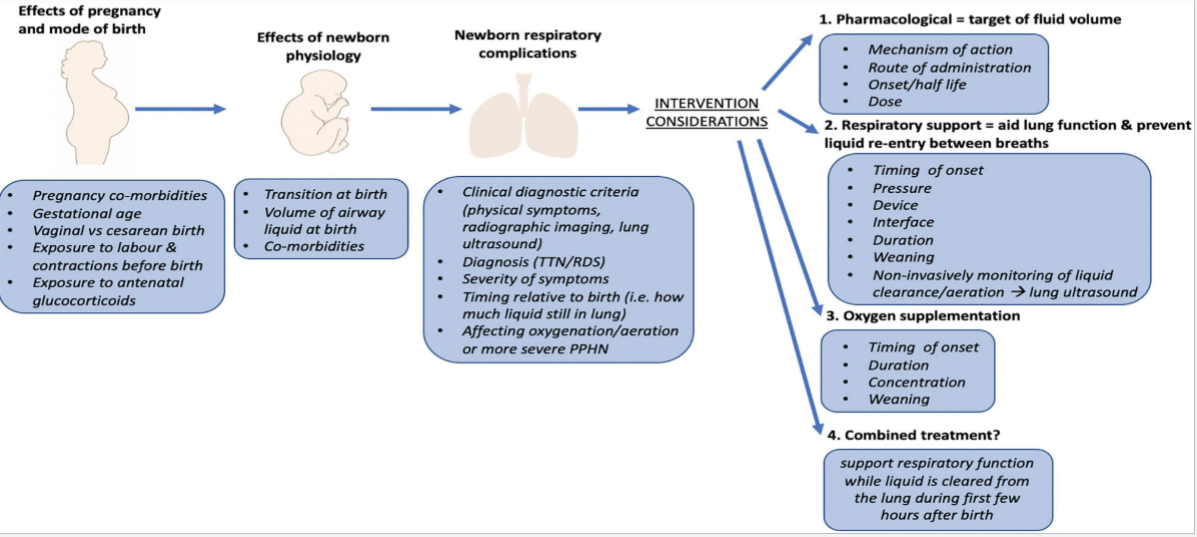
effects of pregnancy and mode of birth
pregnancy co-morbidities
gestational age
vaginal vs. c-section birth
pre-expose baby to TTN
exposure to labor and contractions before birth
exposure to antenatal glucocorticoids
effects of newborn physiology
transition at birth
volume of airway liquid at birth
co-morbidities
newborn respiratory complications
clinical diagnostic criteria (physical symptoms, radiographic imaging, lung, ultrasound)
diagnosis (TTN/RDS)
severity of symptoms
timing relative to birth (i.e. how much liquid still in lung)
affecting oxygenation/aeration or more severe PPHN
TTN interventions?
first 2 hrs post delivery
rapid HR and respiratory
putting baby on belly, skin to skin, apply blow by blow baby (prevents liquid going into airway between each breathe)
pharmacological = target of fluid volume
mechanism of action
route of administration
onset/half life
dose
respiratory support = aid lung function & prevent liquid re-entry between breaths
timing of onset
pressure
device
interface
duration
weaning
non-invasively monitoring of fluid clearance/aeration → lung ultrasound
oxygen supplementation
timing of onset
duration
concentration
weaning
combined treatment?
support respiratory function while liquid is cleared from the lung during first few hrs after birth
Post partum blues, depression, psychosis- symptoms, treatment, risk factors
Post partum blues
Symptoms:
emotional lability - rapid mood swings, feelings of sadness, irritability, and anxiety following delivery
irritability
insomnia
Treatment:
typically resolves within 2 weeks (by post-partum day 10)
self-limiting = resolve on its own
often does not require medical intervention UNLESS it persists past 2 weeks
Post partum depression - major depressive episodes associated with childbirth
Symptoms lasting beyond 6 weeks = post-partum depression
Symptoms:
anxiety
anger
sadness
difficulty sleeping
intrusive thoughts
ex: harm to baby or self
Highly treatable
antidepressants
hormone replacement therapy
Post partum psychosis
surfaces within 3 weeks of giving birth
Symptoms:
sleep disturbances
fatigue
depression
hypomania - persistently elevated mood, increased activity levels, and heightened energy which can also be a part of the bipolar disorder spectrum
Treatment:
medications (ex: antidepressants)
electroconvulsive therapy (ECT)
post-partum psychosis requires immediate treatment usually in the hospital
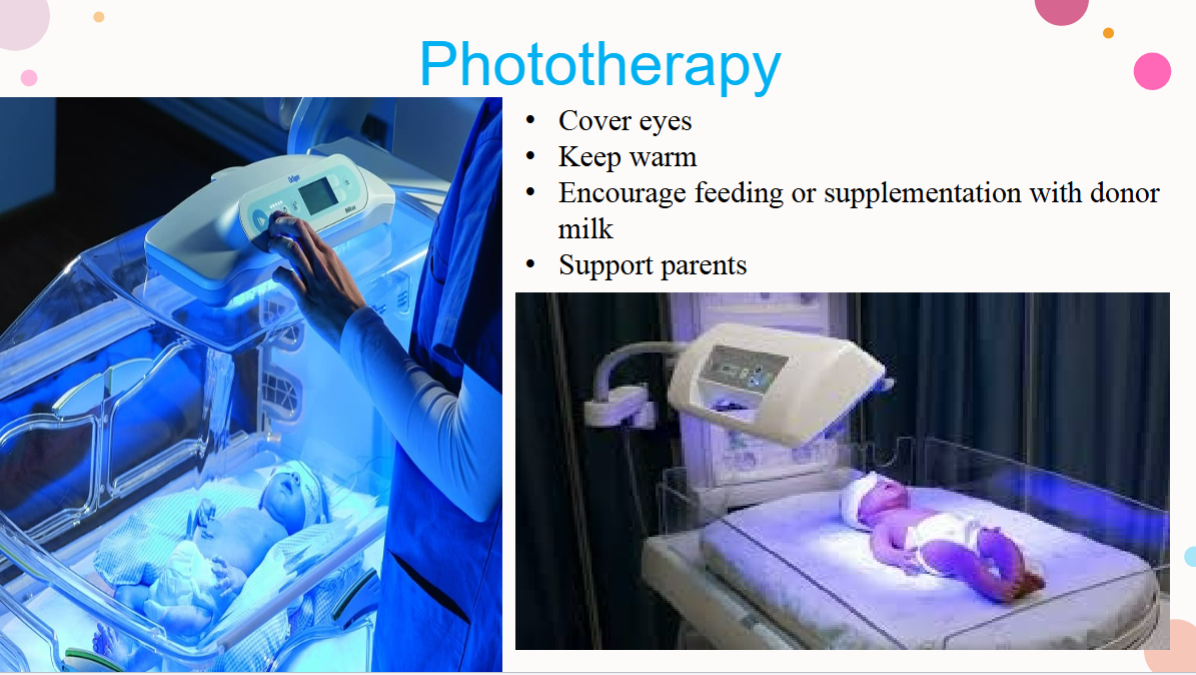
Hyperbilirubinemia -treatments, causes, symptoms
Treatment
phototherapy:
cover eyes
keep warm
remove clothes and just have diaper on
encourage feeding or supplementation w/ donor milk
if mother is breastfeeding, get meconium out of baby, more you feed the more meconium that would get out and the bilirubin levels will go away → inability to break down RBC
support parents
covered in isolet
most optimal
warmer
transcutaneous bilirubinometers market → assess bilirubin level in a newborn
Causes
excessive bilirubin production
SGA
LGA
pre-term
diabetic mother
acquired fetal disorder
hormonal therapies or past surgeries
Symptoms
jaundice, lethargy, high-pitched cry, behavioral changes (jitteriness, irritable), arched back or neck
if left untreated, can turn into kernicterus
DVT risk factors, preventative measures
risk factors: immobility, recent surgery, obesity, smoking, pregnancy, hormonal therapies
preventative measures: sequential compression device, frequent ambulation
Breast feeding, positions, engorgement, feeding cues, mother body response, comfort suggestions, storage.
feeding cues
early cues:
stirring, licking lips
mouth opening
turning head, seeking/rooting reflex
mid cues:
stretching
hand to mouth
increasing movement
late cues:
lots of movement
crying and may turn red
calm crying baby before feeding
cuddling, skin to skin on chest
talking, stroking
mother body response
oxytocin release (“love hormone”)
triggered by the baby’s suckling
causes let-down reflex (milk ejection from alveoli into ducts)
promotes uterine contractions, helping the uterus return to pre-pregnancy size and reducing postpartum bleeding
enhances bonding and maternal feelings of relaxations
prolactin release
stimulate by nipple stimulation and suckling
promotes milk production in mammary glands
higher prolactin levels at night help support nighttime feeding
decreased estrogen and progesterone
postpartum drop in these hormones allows prolactin to act more effectively on milk production
comfort suggestions
ensure proper position
achieve deep, pain-free latch
using soothing products like nipple cream or warm/cold packs
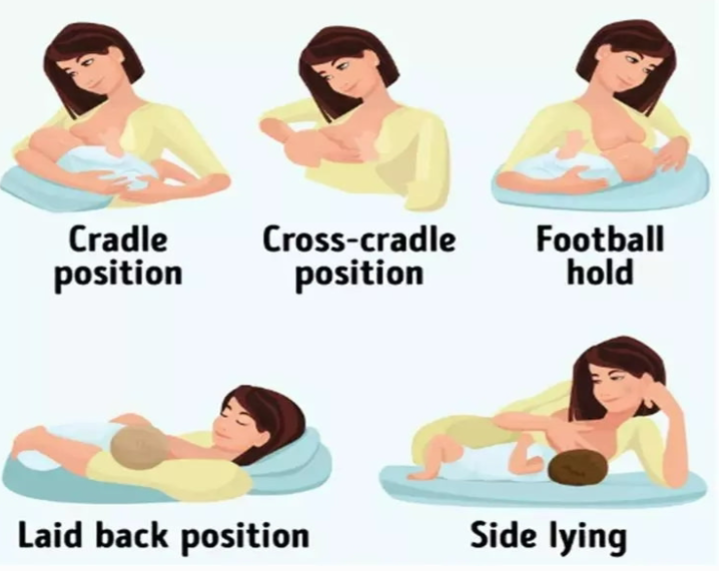
Breast feeding positions
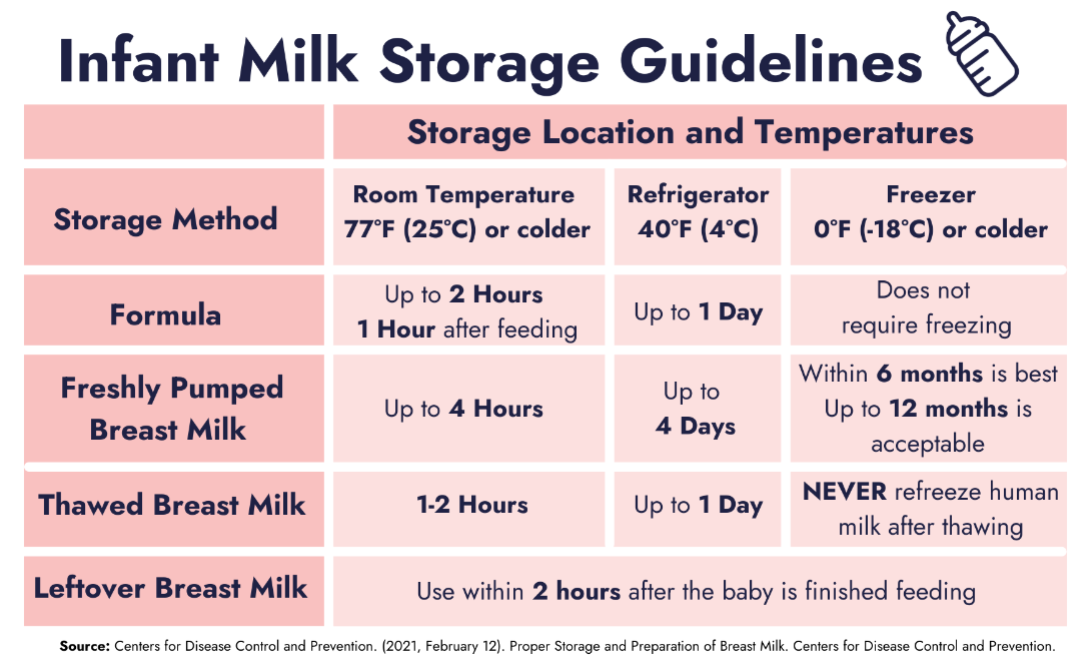
Storage of milk
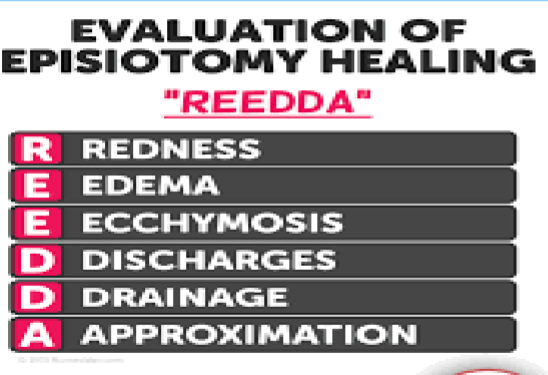
Postpartum vulvar assessment- hematomas, lacerations, episiotomy
week 8 ppt? RE-REVIEW
uterine atony
boggy uterus, fails to contract
lacerations of the vaginal tract
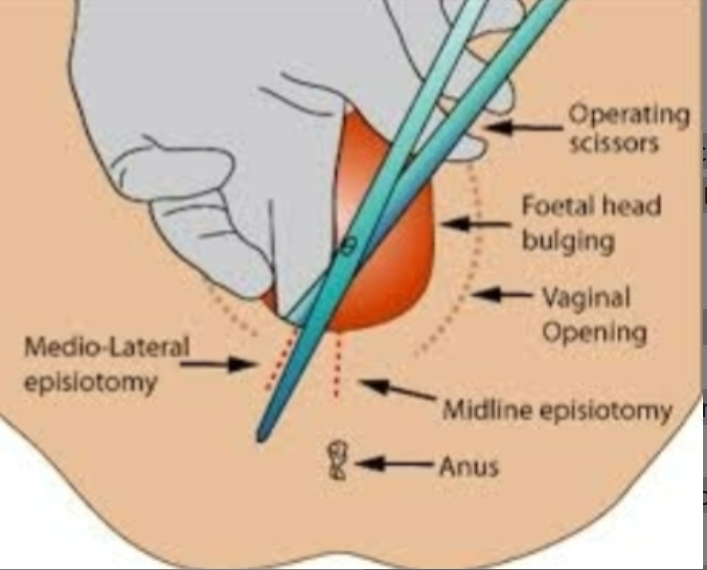
episiotomy
cut vagina
needed sometimes for LGA babies
retained placenta fragments
uterine inversion
uterus not shrinking down
coagulation disorders
hematomas of the vulva, vagina, or subperitoneal areas
hematomas causes back pain
Shoulder dystocia- risk, treatment, post-delivery assessment of newborn
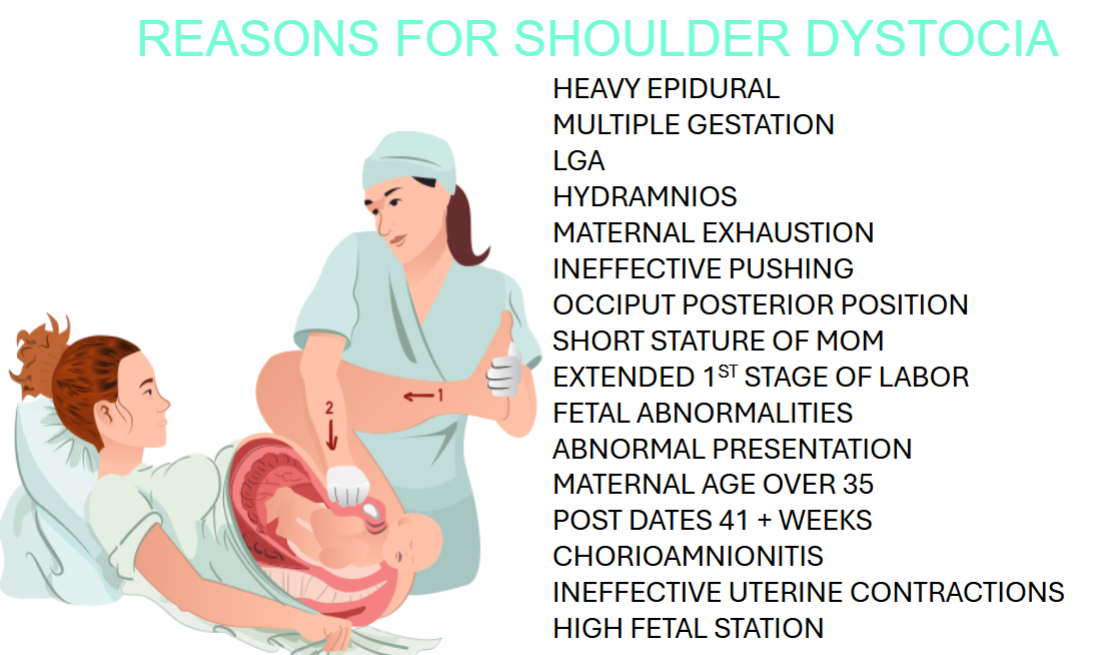
TREATMENT
mcroberts position: lower head, hyperextend leg back, put fundal pressure w/ their fist on the opposite side
suprapubic pressure to dislodge the shoulder
heavy anesthesia → legs are too numb
multiple gestation = (twins or triplets)
post delivery assessments
Newborn:
Assess arm movement & Moro reflex → brachial plexus injury (Erb’s palsy)
Check for clavicle/humerus fracture
Monitor respiratory status & Apgar (hypoxia)
Look for bruising/trauma
Mother:
Assess for postpartum hemorrhage (fundus, lochia, VS)
Check perineal lacerations (3rd/4th degree)
Monitor urinary retention.
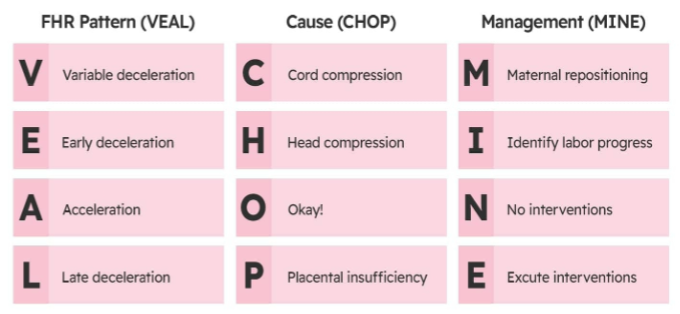
VEAL CHOP MINE
Nursing care immediate post partum, stage 4
recovery: between placenta delivery until mother’s stabilization
1.5-2 hrs in L&D, then go up to mother and baby department
most critical time: post partum —> first two hrs
monitor VS (signs of shock) every 15 mins for an hr, and then every 30 mins for another hr
check fundus — make sure that it is firm and at the umbilicus, immediately after the baby comes out
everyday it goes down finger reth
if i push down there should be a little trickle of blood
if it is a gush of blood —> something is wrong, could be a little placenta
check for post partum hemorrhage — most critical
post partum care
large pads
mesh undies
OTC pain relivers
motrin 800mg + tylenol 600mg
perineal numbing spray
nursing pads
stool softener
perineal squeeze bottle nursing bra
nipple cream
witch hazel pads
Lochia normal vs abnormal, fundal check
1st stage of lochia (aka Rubra)
<5 days
flows like a heavy period. some clotting is normal
dark or bright red blood
mild, period-like cramping
2nd stage of lochia (aka serosa)
3-10 days or 4-12
moderate flow with little to no clots
pinkish brown discharge that’s less bloody and more watery
3rd stage of lochia (aka alba)
5 days to 6 wks or 12 days to 6 wks
yellowish white discharge with little or no blood
light flow or spotting
no clots
Education to new moms about infant care, feedings, diapers, what is normal and what is not
education to new moms
happens within 1 wk old
gains about 2/3 of an ounce every day
suckles, burps, and has first bowel movement
eats 8-12 times a day of breastfeeding; every 2-3 hrs w/ formula
sleeps for 16-18 hrs a day
focuses briefly on a parent’s face when held
6-8 wet diapers a day
Labor- dilation, effacement, station, fetal position
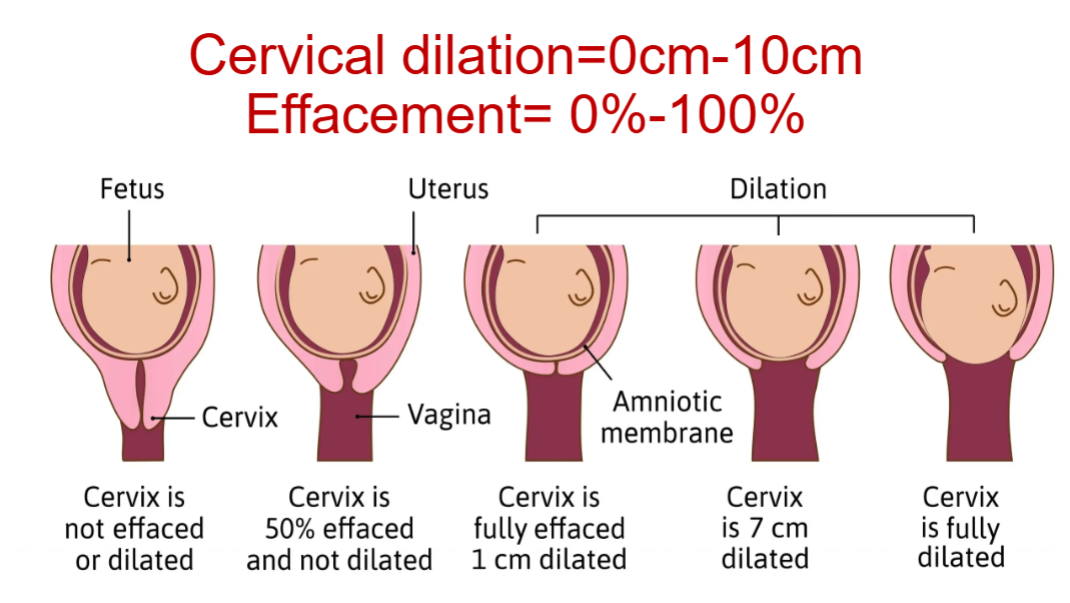
Dilation
cervical dilation = 0cm - 10cm
cervix only opens with good strong CONSISTENT contractions
411: TELL ALL PATIENTS
Contractions 4 minutes apart, lasting 1 minute for 1 hour
CANNOT WALK OR TALK THROUGH CONTRACTIONS (tell every pregnant person)
if you can walk or talk you’re not in labor
10cm = completely dilated
Effacement - thinning & shortening of the cervix
effacement = 0-100%
MUST efface first before dilate (or happen at the same time)
cannot dilate before effacement because the cervix needs to thin out in order to stretch sufficiently for the baby to pass through the birth canal.
you WILL NOT dilate if you are not effaced
FTP (failure to progress) - when their dilation is not dilating adequately within the expected timeframe, often leading to the need for intervention or alternative birthing methods
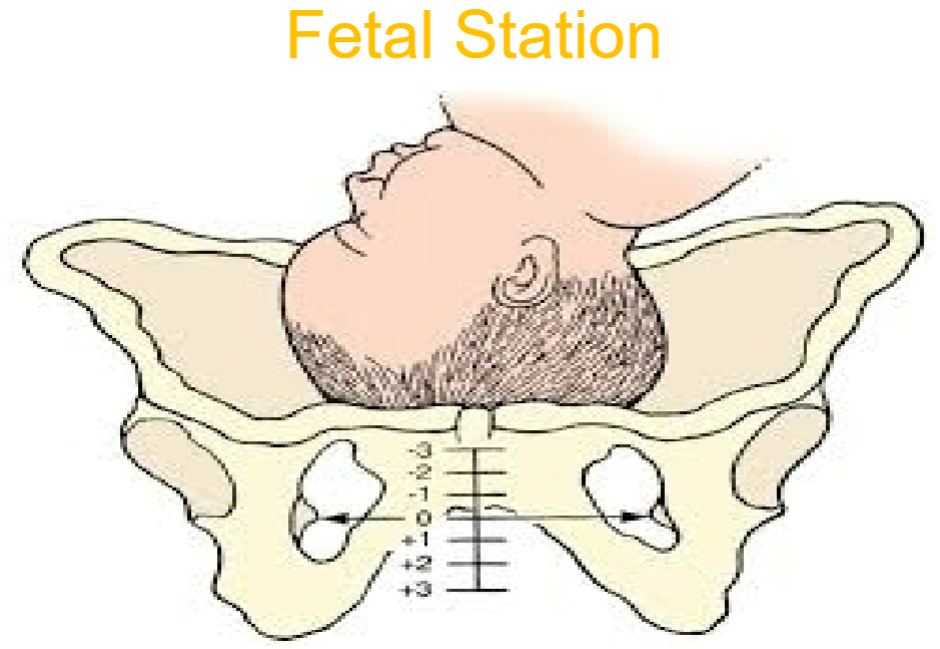
Station
want baby to be in plus stations
put finger in, feel for bone in left or right, then find baby (if baby is in negative it is OOP (out of pelvis?)
as you dilate the baby moves down & goes towards the plus
when the baby drops down into the pluses that is LIGHTNING
feel where the head is in relation to the bones on the left and right bones (aka false pelvis)
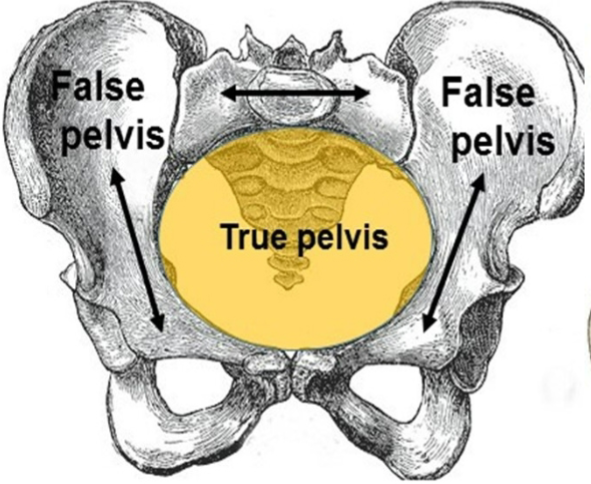
+3 station is also known as crowning of the baby
if baby is super high in station (in the negatives) then the nurse tells the mother, I will give you an hour to push, if the baby does not make progress (FTP), might need to do a C-section because the baby might not come out of vaginal birth
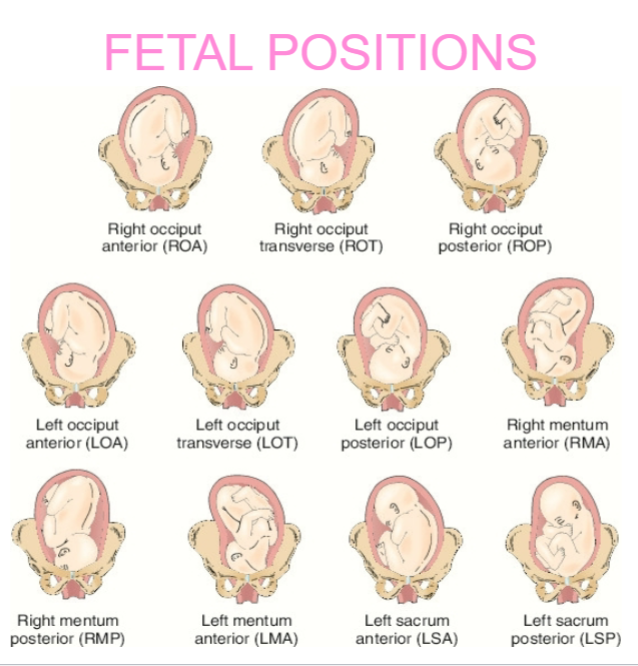
Fetal positions
Occiput - HEAD (means head)
Mentum - CHIN
ex: right mentum posterior (RMP) (chin is facing right towards back)
When back is in pain have mother on all fours leaning forward to relieve pressure on spine
left sacrum anterior & left sacrum posterior are breeched babies (don’t deliver)
Flexed position - proper position of baby: head tucked into chest, arms & legs curled in
optimal fetal positions: ROA and LOA
QBL, EBL Vaginal/c/s, meds, measure
QBL (quantitative blood loss)
helps determine if you have enough autologous blood (your own blood) to return to patient
avoid unnecessary allogenic blood transfusions
^ allogenic blood transfusions increase risk of infection
Possible issues with allogenic blood transfusions:
transfusion-associated circulatory overload (TACO)
transfusion-related acute lung injury (TRALI)
Accurate QBL measurements improve patient outcomes
EBL (estimated blood loss)
inaccurate way of determining blood loss
can cause unnecessary transfusions & transfuse more blood than needed
exposes patient to risk of allogenic blood transfusions
Average blood loss:
vaginal delivery: 500mL (or 500 cc)
C-section: 800 - 1000 mL ( or cc)
anything more than 1000 cc is HEMORRHAGE
Medications for hemorrhage
oxytocin (Pitocin) - 20 units IV
FIRST CHOICE
methergine (Methylergonovine) - 0.2mg IM
SECOND CHOICE
hemabate (Carboprost) - 250mcg IM
THIRD CHOICE
Cytotec (Misoprostol) - 800mcg rectally
FOURTH CHOICE
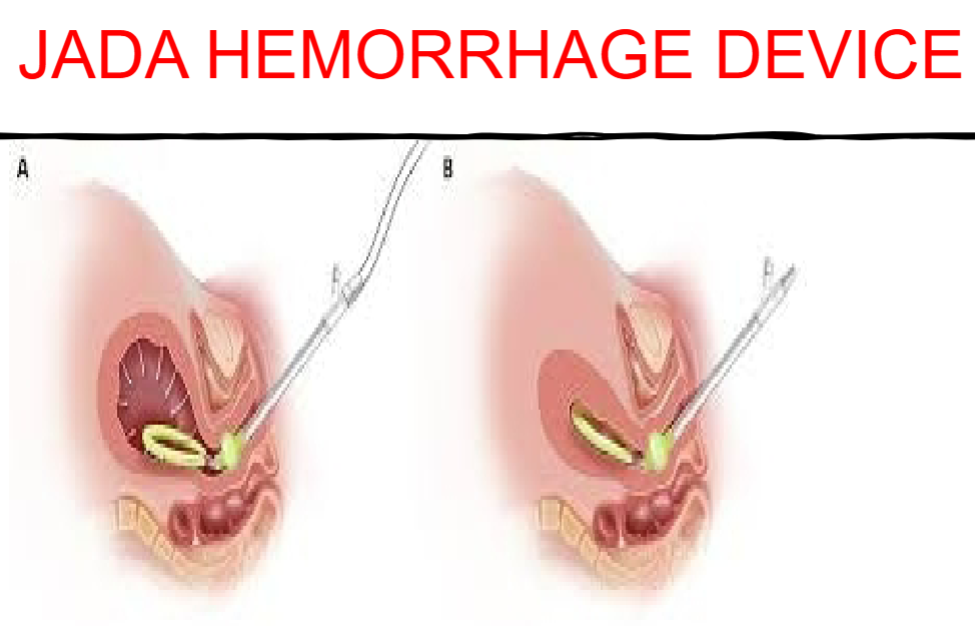
Jada
FIFTH CHOICE
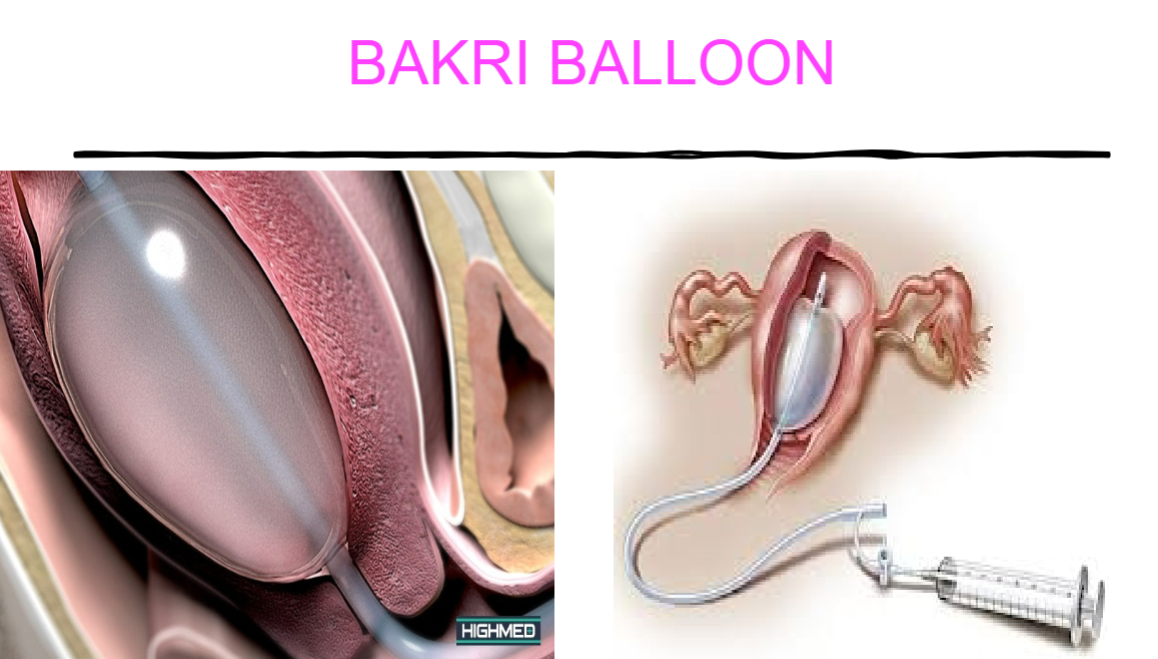
Bakkri Balloon
SIXTH CHOICE
Measuring of blood loss
weigh everything the mother has bled onto
Bottle feeding
hold the baby in a semi-upright position
support the head
breaks every 20-30 secs
let them burp
encourage mouth to open rather than forcing it
horizontal position of the bottle

Normal newborn skin assessment
vernix caseosa- formed during the last trimester
lanugo - formed 16-20 wks, functions as an anchor to hold vernix caseosa on the skin
mottling
harlequin sign
port wine stain
milia- forms when dead skin gets trapped under skin
toxic erythema
mongolian spot
salmon patch/ stork bite
hemangioma
At risk newborns, ie prolonged ROM, diabetics
typically occur at or soon after birth
problems or conditions experienced by the birthing parent during their pregnancy or at birth
possibly no identifiable cause for the disorder
conditions:
neonatal asphyxia - newborn does not receive enough oxygen during the first moments of life, potentially leading to serious complications or even death.
transient tachypnea of the newborn - a temporary condition often characterized by rapid breathing, typically occurring in infants shortly after birth, which usually resolves within a few days.
respiratory distress syndrome - a condition in which the lungs are unable to provide adequate oxygen to the body, often seen in premature infants due to insufficient surfactant, leading to difficulty in breathing and requiring medical intervention.
meconium aspiration - occurs when a newborn inhales a mixture of meconium and amniotic fluid into the lungs during or before delivery, potentially causing lung obstruction and inflammation.
persistent pulmonary HTN of the newborn - newborn's blood pressure in the lungs remains elevated, preventing adequate blood flow and oxygenation
bronchopulmonary dysplasia - a chronic lung disease commonly affecting premature infants, characterized by inflammation and scarring in the lungs, often resulting from mechanical ventilation or oxygen treatment.
retinopathy of prematurity - a potentially blinding condition that affects premature infants, resulting from abnormal blood vessel development in the retina, which can lead to scarring and retinal detachment.
peri-intraventricular hemorrhage - a condition where bleeding occurs in the brain's ventricular system, primarily affecting premature infants, and can lead to neurological complications.
necrotizing enterocolitis - inflammation and destruction of the intestinal wall
birth trauma
hyperbilirubinemia
newborn infections
infants of diabetic pts - may be at increased risk for respiratory distress, hypoglycemia, and congenital abnormalities
nec necrotizing fasciitis: flesh-eating disease, is a rare but life-threatening bacterial infection that destroys soft tissue
can spread quickly and lead to organ failure
Precipitous delivery, complications
rapid birth w/in 3 wks of intense contractions
complications: postpartum hemorrhage
severe vaginal/perineal lacerations
uterine rupture