Rectal Drug Delivery I
Circulation Route
Inferior (bottom) → systemic circulation
Middle → systemic circulation
Superior (top) → portal circulation
Physiological Factors
Fluid Quantity
Mucus Properties
Rectum Contents
Circulation Route
Physicochemical Factors
Water/Vehicle Solubility (Ionization)
water → drug concentration
vehicle → drug release & type
Surface Properties
Hydrophilic + Lipophilic → good
Lipophilic + Lipophilic → bad (remains within the base)
Particle Size → affects sedimentation (big >150) and (small >50)
Drug Concentration
Higher Conc → More Drug → Higher agglomeration rate → reduced absorption
agglomeration → collection/gathering of disparate elements/particles into a single cluster/mass
Molecular Size
Dosage Forms:
Suppositories: Solid dosage forms designed for rectal insertion, melt, soften or dissolve to exert systemic or localized effects
Cylindrical (easier for insertion) → 4 cm, both or one end tapered
Weight (adult: 2g & 1g)
Suspensions or Emulsions
Enemas: injections of fluid (solution/suspension) into rectum AND colon.
micro (1-20 ml)
macro (> 50 ml)
Use Cases:
Unable to use the Oral Route
GI Disorders
N/V
Postoperative → cannot consume by mouth due to inability or unconscious)
Pediatrics and/or Geriatrics (Child or Elderly)
Seizures
Mentally Unstable → lead to suicide (choking) or other cases.
Drug Unsuitable for Oral Administration
Gi S.E (e.g. diclofenac)
Unstable in GIT pH
Enzyme Degradation
First Pass Elimination
Taste Bad
Local Effect Desirable
stay in rectal cavity
constipation
hemorrhoids
anal fissure
Advantages:
Accommodates relatively large dosage volume
Safe and Convenient ROA
Minimize Drug Dilution
Less degradative enzymes → more gets in the blood
Easy Discontinuation
Partially Bypass FP
Disadvantage
Not widely accepted
Absorption Rate dependent on presence of feces
Difficult to Administer
Formulation of Suppositories
vehicles
active ingredients (drug)
excipients (additives)
Requirements
non-toxic/non-irritation → bowel movement can occur due to irritation of mucous membrane → diarrhea
compatibility of drug → ensure no interactions that can cause adverse effects
physically and chemically stable during storage before expiry date → efficacy is maintained
melting range → melt in insertion or dissolve in rectal fluid
small enough to allow solidification after preparation
big enough for industrial scale → easy to manufacture consistently
Volume contraction → allow for easy removal w/o breaking from the mold
Viscosity → thick enough to have good flow into mold (even/consistent distribution and dosing per suppository) → low sedimentation rate → gradual drug release and able to spread evenly over mucosal surface for absorption
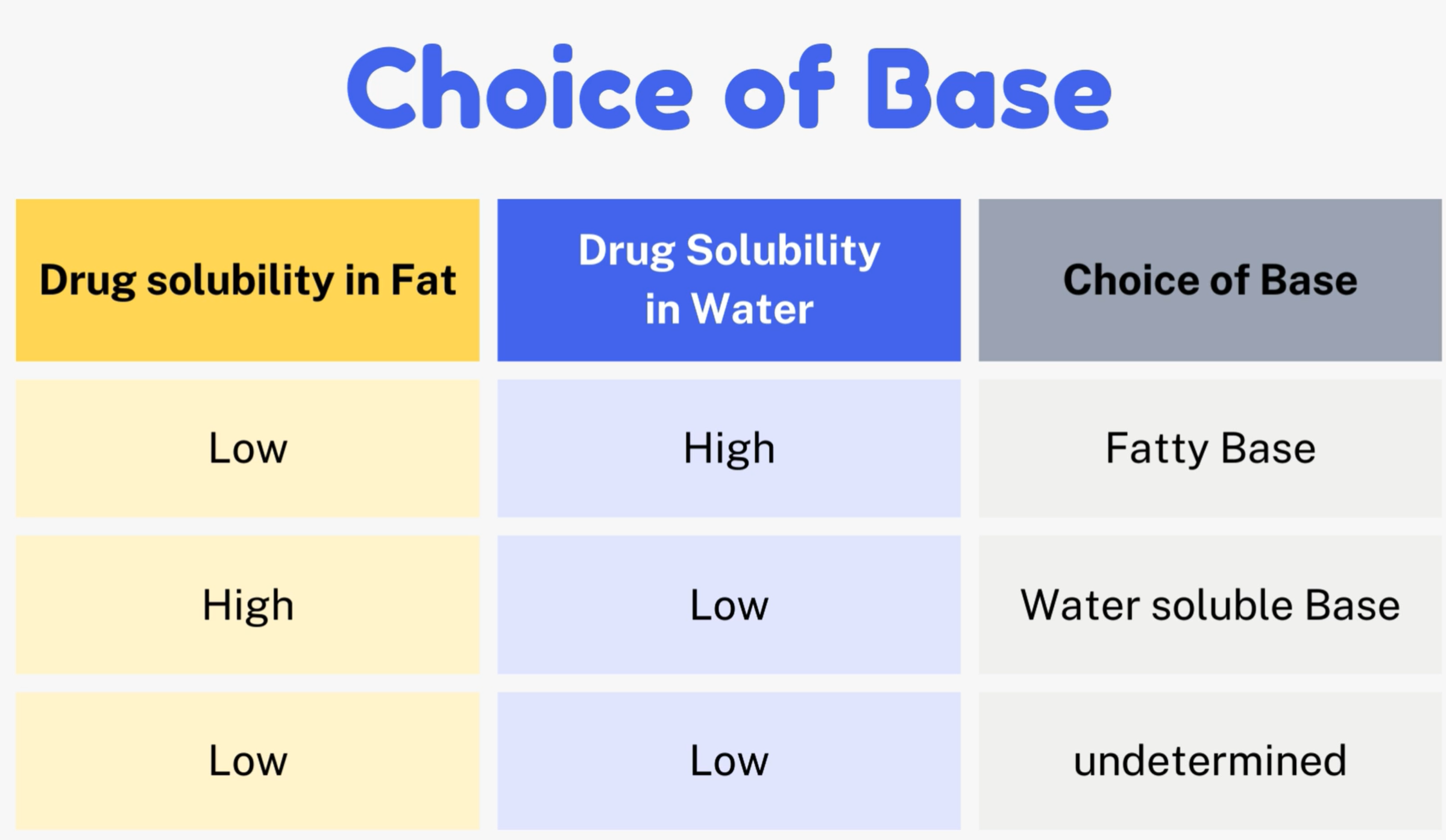
Bases
fatty
cocoa butter (smell like chocolate, yellowish-white, non-irritant, melting point (30-35 degrees) → keep in the fridge.
Disadvantage: Polymorphism (overheating → structural change and unstable) → new melting point (25-30 degree) — melts too early at room temperature
solution: increase melting point (e.g. beeswax) or decrease melting point (phenols)
Synthetic Triglycerides: hydrogenated fatty acids of vegetable oils (e.g. coconut oil) → more expensive & melting point varies based on its combination with other drugs
Advantage: does not experience polymorphism.
water-soluble
Glycerinated Gelatin → translucent yellow tint, hygroscopic (water content), dissolves slower (prolonged release) → administered by dipping in water first (difficult to administer dry) → store in cool, dry place/in containers.
Disadvantage: more prone of bacterial/microbial growth
Solution: Add preservatives for longer shelf-life and prevent growth.
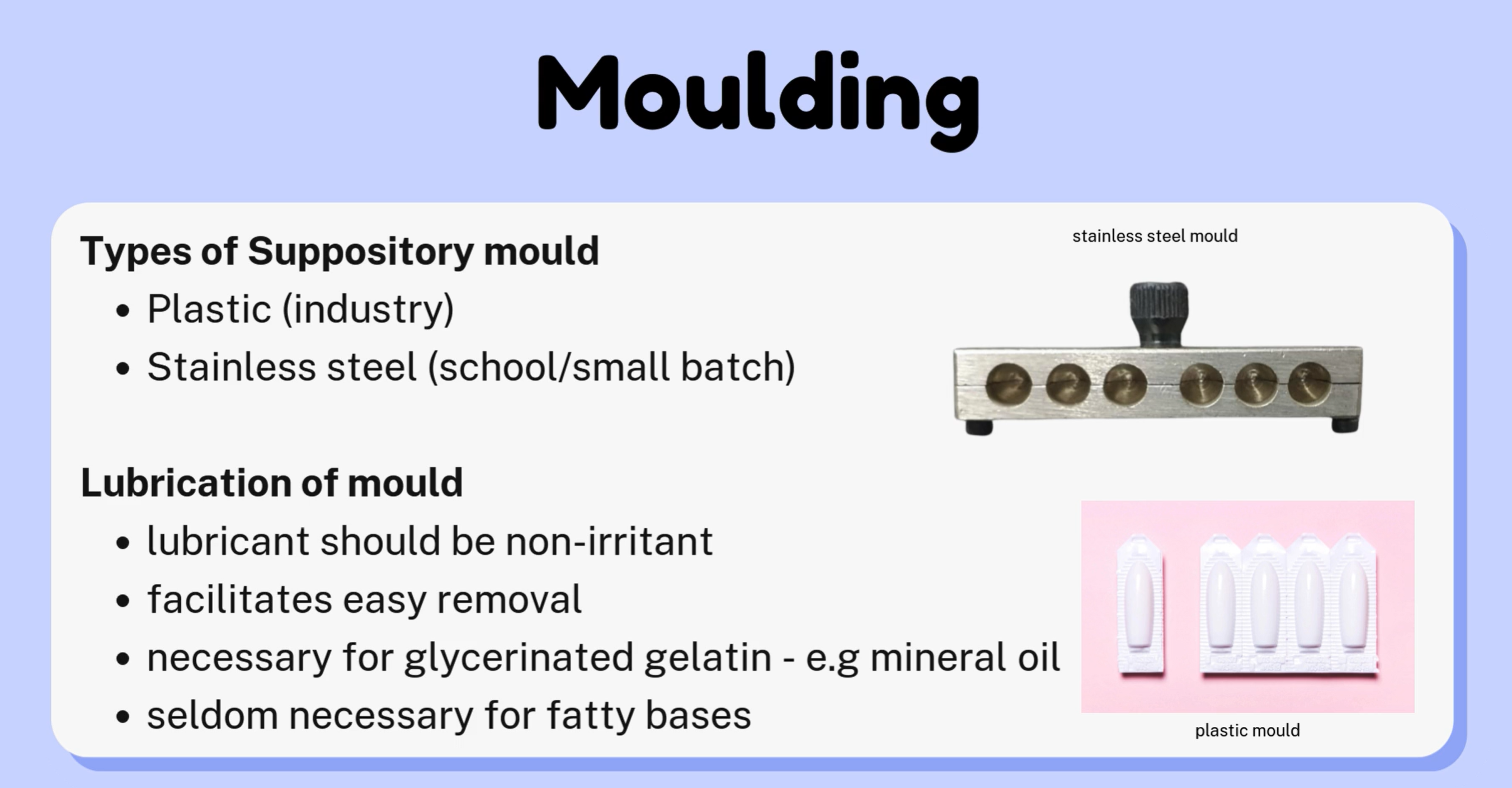
Must be lubricated before placing into the mold (sticky) → e.g. mineral oil
PEG polymers → translucent white, chemically stable, non-irritant, combined with others, doesn’t melt at body temp, dissolve slower
can vary in solubility and chemical properties when combined with other excipients.
Fatty → melts in the rectum for drug release + PEG polymers.
W.S.B → dissolve in the rectal mucus/fluid for drug release.
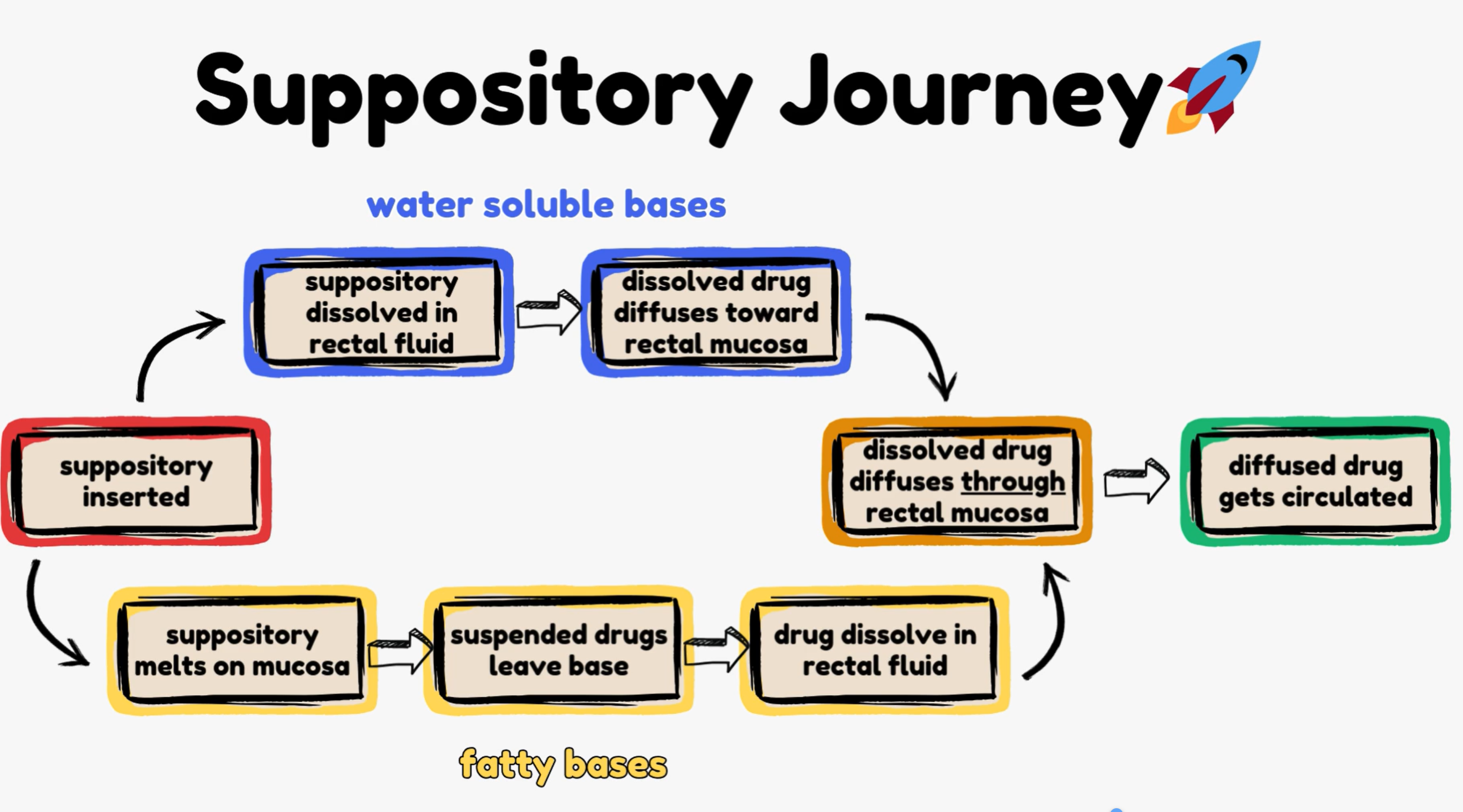
opposite compared to other concepts → because main goal of making suppositories is for the drug to be suspended in the suppository and not dissolved within in.
Common Excipients used
Surfactants → mainly surface-active agents → reduce surface tension
Thickeners → increase viscosity → gel-like system to prolong release → transit time (longer)
Melting Point Altering Agents → phenol
s (decreased), beeswax (increased)
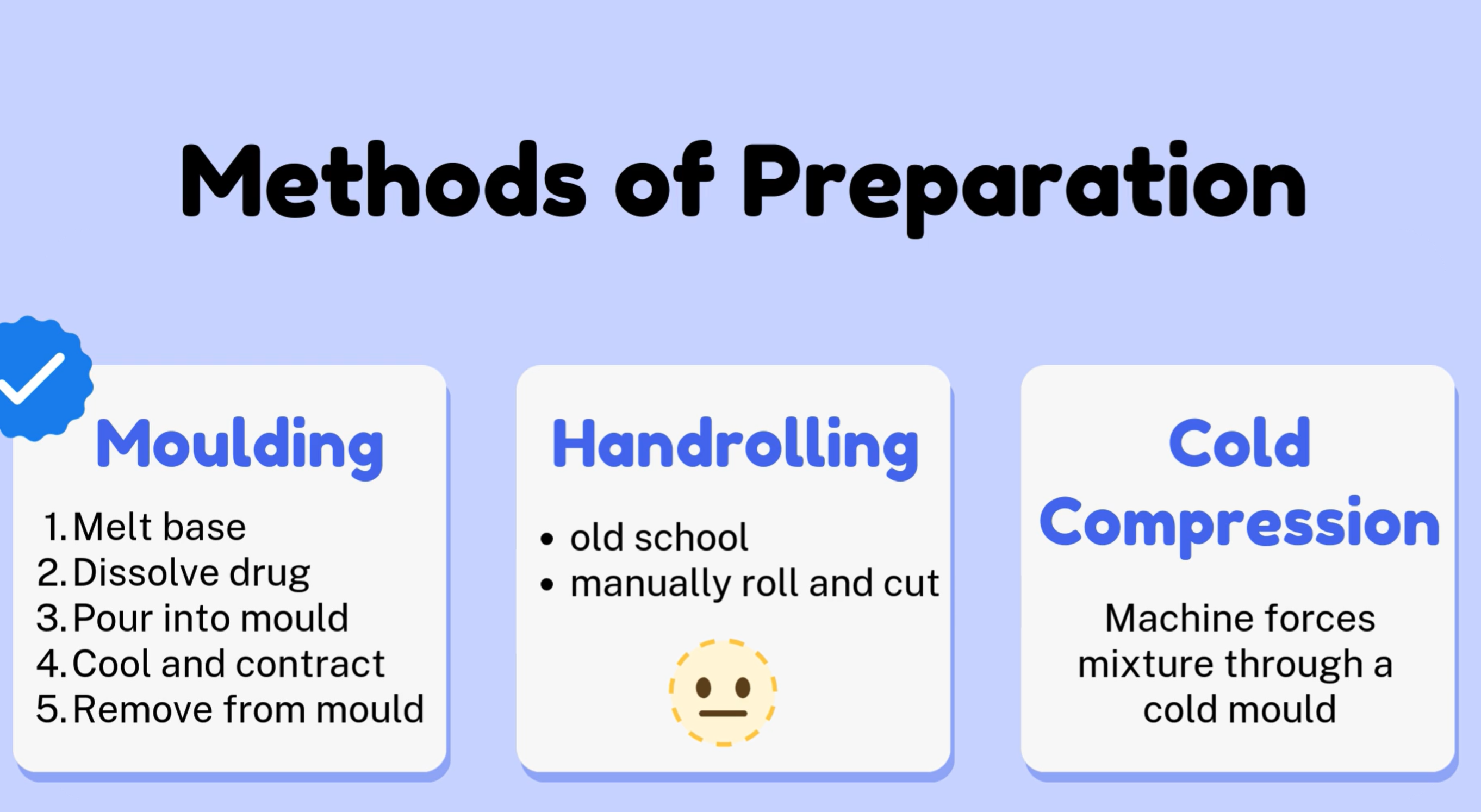
Methods to Make Suppositories