EMSF110 - Trauma Exam
**CHAPTER 31 - CHEST & ABDOMINAL TRAUMA**
CHEST INJURIES
blunt trauma: most common injury, can fracture ribs/sternum/costal cartilages
compression: develop from severe blunt trauma, disrupts normal chest motion
penetration: bullets/knives/metal or glass pieces/rods/pipes/etc.
flail chest: occurs when blunt trauma creates a fracture of 2+ ribs in two or more places, reduces lung expansion
paradoxical motion: movement of ribs in a flail segment that is opposite the direction of movement of the rest of the chest cavity
pneumothorax: air in the pleural cavity
tension pneumothorax: begins to affect the unaffected lung or the heart because air cannot escape (if created from an occlusive dressing, burp it)
- tracheal deviation: trachea moves away from affected lung
hemothorax: chest cavity fills with blood
hemopneumothorax: chest cavity fills with blood & air
- jugular veins may be flat due to volume loss
traumatic asphyxia: sudden compression of the chest forces blood out of the organs and ruptures blood vessels
- neck/face are darker color than rest of body
- possible bulging eyes/JVD/broken blood vessels in face
cardiac tamponade: occurs when blood entes the pericardial sac
- signs: JVD, muffled heart tones, narrowing BP
aortic dissection: marked by tearing pain (in chest, back, stomach, etc.)
commotio cordis: uncommon, caused by trauma to the chest at time when heart is vulnerable → V fib
- Tx: CPR + defibrillation
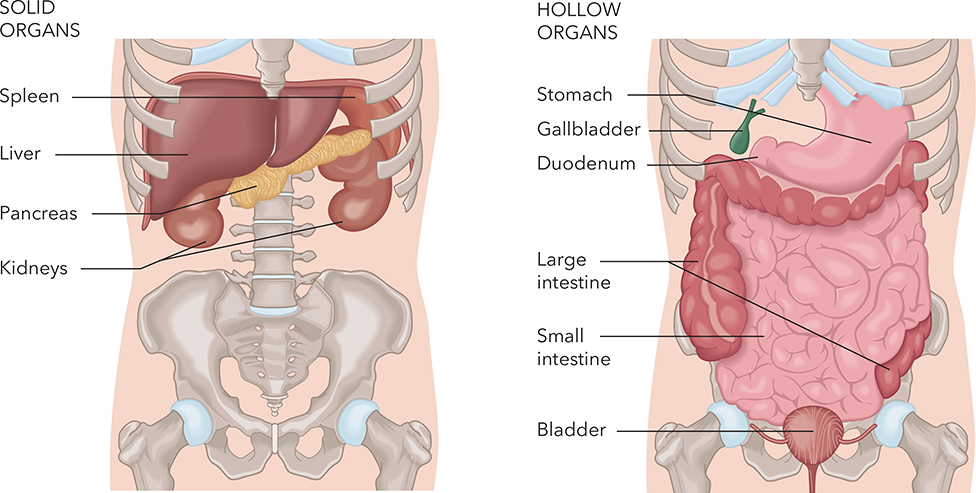
ABDOMINAL INJURIES
- evisceration: organs protruding through a wound opening
- place pt on back with knees flexed to chest
- apply saline-moistened sterile dressing over wound site & cover with occlusive dressing
- compartment syndrome: severe swelling & bleeding within an extremity
- signs: sensation of internal pressure, may feel hard on palpations, reduced CMS
SIX Ps OF ASSESSMENT
Pain/tenderness
Palor
Paresthesia (pins & needles)
Pulses (diminished or absent)
Paralysis
Pressure
***can attempt to realign a PULSELESS extremity once in the field
SPLINTING
- rigid splint
- formable splint
- traction splint: used for mid-femur injuries ONLY
CHAPTER 33 - TRAUMA TO THE HEAD, NECK & SPINE
SKULL/BRAIN INJURIES
- coup injury: occurs @ site of injury
- contrecoup injury: occurs opposite the site of injury
- hematomas:
- subdural: between brain & dura
- epidural: between dura & skull
- intracerebral: inside brain
- decorticate posturing (hands/feet towards core) or decerebrate posturing (hands/feet away from core)
signs: visible skull bone fragments or brain tissue, Battle sign, pupils unequal/nonreactive to light, depressions/deformities/swelling of skull, altered mental status, “racoon eyes”, Cushing reflex, projectile vomiting, ringing of ears, etc.
***ICP (intracranial pressure)
NECK INJURIES
- stop bleeding
- prevent embolus
SPINE INJURIES
***look for loss of bowel/bladder control
***high priority (physiologic findings): altered mental status, abnormally slow or rapid resp rate, cool/pale/clammy
***high priority (anatomical findings): amputation above wrist, pelvic or chest instability, 2+ long bone injuries, etc.
remember ABCs, golden hour, limit on-scene time, request ALS & rapid transport
COLD EXPOSURE
- hypothermia: can be increased by alcohol ingestion, underlying illness, major trauma, etc.
- infants/children and older adults are most prone to hypothermia
- signs: shivering, numbness, stiff/rigid posture, drowsiness, rapid HR and resp rate, LOC, cool/red/pale/cyanotic skin
- extreme: no detectable vital signs, HR 10 bpm, very cold to touch
passive rewarming: cover pt, remove wet clothing
active rewarming: apply external heat source
- frostnip (early/superficial): remove from cover & cover
- frostbite (late/deep): oxygenate and cover affected area !DO NOT RUB OR MASSAGE!
HEAT EXPOSURE
- hyperthermia: any heat not needed for temperature maintenance
- heat cramps/exhaustion: moist/pale/normal or cool skin, usually occurs @ beginning of summer
- Tx: remove from environment, lay in supine position, apply moist towels over cramped muscles
- heat stroke: temperature-regulating mechanism fails, marked by stoppage of sweating
- Sx: hot skin (may be dry or moist), altered mental status, LOC, rapid/shallow breathing, N/V, dilated pupils, temp 104+, potential seizures, no muscle cramps
- Tx: apply cool packs, remove clothing, administer high-concentration O2
WATER-RELATED
- drowning: experiencing respiratory impairment from submersion/immersion in liquid; triggers spasm of larynx; final attempt at breath allows water to enter lungs
- arterial gas embolism: bubbles in the bloodstream due to diver holding breath upon resurfacing
- air embolism: stroke-like symptoms
- decompression sickness: caused by rapid surfacing after deep, prolonged dive (takes 1-48 hours to appear)
HIGH-ALTITUDE ILLNESS
- acute mountain sickness: Tx may consist of anything from rest & rehydration to supplemental O2 & immediate descent
- high-altitude cerebral edema (HACE): severe form of acute mountain sickness, often takes 2-3 hours to appear
- high-altitude pulmonary edema (HAPE): severe form of acute mountain sickness, results in respiratory failure/arrest
BITES & STINGS
***all spiders are venomous
- treat for shock
- contact medical direction
- remove stinger or venom sac