GI system PEDS
Vomiting
~ GI disorders, infection, food allergies, motion sickness, obstruction, increase intracranial pressure, Rx adverse effects
Gastrointestinal infection | Common pathogens include norovirus, rotavirus, Salmonella, and Escherichia coli. |
Gastroesophageal reflux disease (GERD) | The LES fails to prevent the backflow of stomach acid into the esophagus. |
Mechanical obstruction | This includes stenosis, malrotation, ileus, intussusception, and strictures. |
Food poisoning, allergies, and toxins | The immune system views some substances as a threat, triggering vomiting as a protective mechanism. |
Gastrointestinal motility disorders | Disorders like gastroparesis disrupt the expected movement of food. |
Underlying conditions | These include gastritis, appendicitis, peptic ulcers, pancreatitis, and inflammatory bowel disease (IBD). |
Medications and treatments | Chemotherapy, anesthesia, radiation therapy, antibiotics, or NSAIDs can cause nausea and vomiting. |
LES + UES relaxes while stomach, diaphragm, abdomen contract
Vomiting Center in medulla oblongata; GI tissue irritation; structural anomalies that obstruct flow → activation of SNS → increase HR, RR, close of glottis to prevent aspiration, sweating
Screening: for post-op
Determining level of nausea by using ranges of faces for younger children
Psychological factors, head injury, migraines, low or high BG, brain tumors, pregnancy, self-induced, cannabis, consumption of toxic substances
Risk factors
Poor hand hygiene, improper food preparation, on clean water = gastroenteritis
Food allergies/ intolerances, motion sickness, immunodeficiencies, sx, Rx
S/s: ~ contain food particles, bile, mucus, blood
Splitting up is mild regurgitation of food shortly after eating and common in babies
Vomit child seem sick and have more amount
if undigestive food → pyeleric stenosis
lab/dx:
Presentation, hx, duration, CBC, BMP,
assess for infection, anemia, E/I
U/A for dehydration, kidney problems, infection, pregnancy
Imaging = ultrasound, gastric emptying test, upper GI
CNS evaluation
Tx:
Prevent dehydration, relieve s/s, treat underlying cause
Bland diet,
oral rehydration (oral rehydration solution/ ORS = 1 Cup for every 10 lb) has electrolytes
Start w/ small sips of 5 ml q1-2min → gradually increases
If induced vomit, wait for 30 minutes and try again
If unable to oral rehydration → IV hydration and antiemetics
Measure w/ syringe or standardized medicine cup
Freeze solution like a popsicle
DO NOT give high sugar content like sports drinks or soda
Rely on observation and infants and young children = be aware of the compensation since they are more vulnerable to dehydration = low urine output, dark urine, sunken fontanels, lethargy, decreased tear production, dry mouth/ skin, skin color change
Talk about cleanliness, Oral Care ,hydration, feeding techniques, portion sizes, avoiding overfeeding and allergens
To treat motion sickness = provide ventilation during rides, avoid reading or playing games in car, ensure child has a view out of front window during car
Diarrhea =
Three or more liquid stools or lose consistency within 24 hour.
Acute = infections agent infiltrates wall lining (norovirus , rotavirus , C. diff [ if ABX ]), covid-19 = inflammation → decrease absorption of fluid and nutrients + increase peristalsis
most common agents: Vibrio cholerae or Escherichia coli.
Most common cause of bloody diarrhea = shigella
Can self resolve within less than 14 days
Unless bloody or mucus stool , fever , severe abd cramping or tenderness , or s/s of dehydration or sepsis → HCP
Chronic = tumor, cancer, food allergies, celiac (malabsorption of nutrients) ADR, IBD (rapid contraction of intestinal muscles)
→ weight loss , severe malnutrition , dehydration
→ detail hx , stool assessment and testing , cancer screening , allergy , Rx review
Functional diarrhea = chronic diarrhea that rules out no explanation → can continue life but will continue to have daily diarrhea
→ lead to dehydration = lethargy , Restlessness, sunken eyes , in ability to drink , skin trigger (chronic =+ malnutrition ), little urine output in 12 hours/ know what diaper in 6 hours , low LOC
Diarrhea is acidic + frequent wiping = perianal skin breakdown
Risk :
Laxatives, attending daycare, poor hand washing, <5y
Lab / dx:
Stool culture (if blood in stool or fever);
Rotavirus antigen(if outbreak)
stool occult blood = shingella, salmonella
CBC , CMP, urine specific gravity
For chronic diarrhea= extensive health hx, gastroenterologist, check for over and parasites, lactose intolerance and celiac
CBC CMP, F/E/I,
ESR, CRP = inflammation, autoimmune, cancer
Follow up w/ nutritionist
Tx= prevent dehydration and malnutrition reduce frequency and duration of episodes
Oral or IV fluid replacement,
ABX: Ciprofloxacin(shigella),
Zinc and vitamin A
No antidiarrheal (loperamide) for <2yr = worse s/s, bacterial infection, tx delay, ileus
If does not feel like drinking = offer through syringe, small amounts from spoon or small cup, older than one here can have frozen popsicles
Use those for demonstration of proper wiping and hand hygiene
Constipation
Fewer than two BM per week, or has difficulty or painful BM; Hard, dry, Lumpy, large tool → fecal impaction
fecal incontinence when: gets to full and liquid stool leaks
Poor appetite, n/v , bloating , anal fissures , rectal prolapse , UTI , megacolon
infants = three to four BM/ day
toddlers, younger children, school age , adolescence = 1-2 per day; skipping a day does not mean they are constipated unless it is difficult to pass
Excess water absorption and: causes stool to be hard and dry
Decrease peristalsis = longer Transit time
Impaired rectal sensation and coordination decreases urge to defecate
Impaired anal sphincter or intestinal muscle coordination causes problems on completing ball movement
Screen: ask about frequency consistency and appearance of stool = Bristol Stool Form Scale = hard Pebbles
Basketball blood, child routine, daycare, eating and drinking habits, physical activity, Rx
→ if chronic screen for celiac and food allergies
Risks: unclean bathrooms, stress, abuse, age, trauma, diet and routine change, genetics, transition from formula to solid foods, toilet training, and familiar surroundings, Behavior
Lab / dx:
Check stool for blood, parasites, infection
CBC, CMP, thyroid function blood test
Nutritional deficiencies, anemia, underlying
Abd x-ray, ultrasound = access to amount, degree of fecal impaction, structural anomalies
Barium enema x-ray, colonic Transit study. Anorectal manometry
MRI to check for lumbosacral spine
Tx:
Diet modification, Rx, gastroenterologist
Behavior = regular bathroom routine, (+) reinforcement(reward chart), promoting toilet posture w/ step stool, established routine
Polyethylene glycol
Adequate fluid intake |
|
Balanced diet |
|
Healthy toilet habits |
|
Physical activities |
|
Stress Management |
|
Dehydration
Infants and young children are more vulnerable: infant is 70% → 1y is 65 % → adults is 60% ; higher body surface area
More likely due to diarrhea and vomiting →F/E/I → hypovolemic shock, cell dysfunction, organ failure, metabolic acidosis (especially in diarrhea)
From not drinking enough water , poor feeding , illness , low thirst sensation , excessive sweating ,
GI infections or disorders (rotavirus/ Crohn's disease )
Dehydration type:
Isotonic = water and sodium lost together = diarrhea and vomiting; Na = 130- 145
Hypotonic= sodium loss> water loss = endocrine issues, diuretics, cystic fibrosis; Na <130
Hypertonic: water loss> sodium loss = fever; Na >145
Screening: check consciousness, breathing, color
At-the-Door Severe Dehydration Assessment
Signs of severe dehydration include:
Decreased level of consciousness = Lethargic
Breathing difficulties = In severe respiratory distress or not breathing
Skin color = Mottled, gray, or cyanotic
S/s
Weight loss, decreased tear production/ urine output, dry mucus, irritability, lethargy, sunkened fontanels/ eyes, reduced skin turgor/ capillary refill, cool mottled skin, high RR and HR → weak or absent peripheral pulses, low BP
Prolonged dehydration → decline in development and cognitive
Urine output=
0.5 to 1 mL/kg/hr if the child weighs less than 30 kg (66.1 lb)
30 mL/hour for a child over 30 kg (66.1 lb).
Lab/diagnosis:
Glucose test, u/a for infection, specific gravity, ketones
CMP, CVC, bun/cr, EKG( for E/I), x-ray for GI, ABG for acid base inbalance
Tx:
Oral rehydration,: breastfeeding, low sugar and age appropriate Foods in small amounts
Moderate dehydration: oral given at rate of 50-100mL/kg for 1st two to four hours
Severe: IV boluses of 20mL/kg 0.9% over 10-20min; bolus going to be given again if child is not stabilize
If concerns about HF or fluid overload: 10mL/kg 0.9% NS = careful w/ fluid overload and Pulmonary congestion
Encouraged to carry water bottles, frequent drinks of water throughout the day
Maintenance IV Fluid Requirements for Pediatric Clients Based on Weight
Less than 10 kilograms: 100 mL/kg/day
Less than 20 kilograms: 1,000 mL/day plus 50 mL/kg/day for each kilograms between 10 kilograms and 20 kilograms
Greater than 20 kilograms: 1,500 mL/day plus 20 mL/kg/day for each kilograms over 20 kilograms
Divide the total by 24 to determine the hourly rate.
Safety Precautions When Administering IV Fluids With Additives
Do not administer fluid boluses with potassium in the solution.
Potassium losses must also be replaced slowly to avoid hyperkalemia and cardiac arrhythmias.
Do not add potassium to IV fluids until the child has a urinary output.
Do not administer fluid boluses with dextrose/glucose in the solution unless the child is hypoglycemic and there is an order for it.
Feeding issues
Due to emotional stress, abuse, trauma, limited appetite, food selectability, fear of feeding
Structural or functional = sucking , chewing , swallowing problems
Cleft lip / palate , esophageal atresia
GI disorders = IBS, gastroenteritis, colic → abd pain, gas, bloating, constipation, vomit, diarrhea
picky eating when toddler and preschool
Sensory disorders affects our child perceives food
→ malnutrition →F/E/I, growth restriction, developmental delays, disruption of organ
Underlying dysfunction can lead to feeding issues.
Medical dysfunction: Cardiorespiratory issues during oral feeding may involve aspiration, aspiration pneumonia, dysphagia, or reflux.
Nutritional dysfunction: This is malnutrition due to nutrient deficiency, possibly due to decreased dietary diversity or requiring oral supplements to sustain nutrition or hydration.
Feeding skills: This can include the need for texture modification of food or liquids. Modified feeding positions, equipment, or strategies may also be needed.
Psychosocial: This includes avoidance behaviors at mealtime and may be related to inappropriate parent management, bonding, or interaction during feeding time.
Risk factors:
Selective food preferences , premature , adverse early feeding experiences , poor feeding environment , lack of Parental knowledge or time , lack of availability of foods or access to healthcare , poor feeding practices (lack of bonding , forceful feed , pressure to eat , restriction of certain foods , using Foods as reward)
Screening: observation, hx, development, growth chart, prenatal ultrasounds or genetic testing if congenital
Feeding assessment questionnaires = appetite, meal patterns, orofacial problems, and/or the parent’s perceptions.
S/s
arc back or stiffen and fuss while eating,
Coughing, choking, congestion, gagging, drooling, gurgling, harness, spitting up, long time to eat, falling asleep while eating, dehydration, malnutrition, aspiration pneumonia, (-) thoughts about eating
Lab/diagnosis
stool, blood work, barium swallow study or endoscopy to see swallowing
Celiac disease screening if multiplication
Iron or lead testing if pika
Dysphasia assessments by speech therapist using video fluoroscope swallow study or Fiber Optic endoscopic evaluation
Tx:
Dietitians, speech therapy for swallow safety, social work, Mental Health, Occupational Therapy(helps w/ eating and trying new foods),
Teach parents model behaviors, , (+) reinforcements, clear expectation and boundaries, consistent eating routines
Failure to thrive FTT
Patients weight for their age is less than 5%, or weight decrease by two major percentiles
Malnutrition , poor muscle tone , appearance , dry or pale skin , brittle hair and nails ,
~ have health condition , oral motor dysfunction , heart murmur
If neglect = poor hygiene , diaper rash , lack of eye contact , loss of hunger Drive , stiffness while being held , lack of crying to express hunger
Protein or energy deficiency , risk for infection
Cerebral palsy + trisomy 21 = diff growth chart
Underlying problems, socioeconomic issues, insufficient calorie intake, increase metabolic demands, malabsorption
Poor parental bonding , poverty , lack of food , food selectability , neglect or abuse , mental health , SUD, inadequate parental knowledge of proper nutrition
From structural anomalies, neurological disorders( decrease appetite), on the crime system not releasing enough growth hormone, chronic pancreatitis, cystic fibrosis( decrease enzymes = malabsorption)
Most common inadequate nutrition , behavioral disorders
Organic = celiac , GI infections , food intolerance , GI reflex , gastroenteritis
Growth hormone deficiency , hypothyroidism , IUGR
Screen monitoring the growth charts and parameters, consistent decline, detailed feeding hx
Lab / dx:
CBC for anemia or infection/ CMP E/I, liver and renal function
Check iron and vitamin D
Stool sample = malabsorption, inflammation, infection
Imaging for anatomical anomalies or skeletal conditions
Tx:
Education, support, Behavior, dietitians, nutrition counseling, calories supplementary, caring for underlying disorder
Check for clean water access, and exposure for infections : H pylori, giardiasis
~ require supplementation
Age | Average Weight Range | Caloric Intake Requirements |
|---|---|---|
Newborns | 3.2 to 4.1 kg (7 to 9 lb) | 100 kcal/kg/day |
Infants and toddlers (1 to 3 years) | 10 to 15.9 kg (22 to 35 lb) | 80 kcal/kg/day |
Preschoolers and (4 to 5 years) | 13.6 to 22.7 kg (30 to 50 lb) | 70 kcal/kg/day |
Young school-age (6 to 8 years) | 18.1 to 41.7 kg (40 to 92 lb) | 60 to 65 kcal/kg/day |
Older school-age and adolescents (9+ years) | 27.2 to 81.6 kg (60 to 180 lb) | 35 to 45 kcal/kg/day |
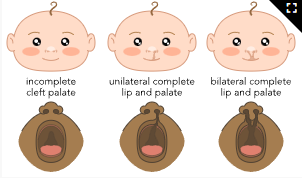
Cleft lip / palate
Cleft lip = Gap in upper lip that can range from small Notch to larger opening day extends through the lip into the nose
Palate = opening in the palate
Lip = Occurs during 4 to 7 weeks of gestation
Upper lip has Vermilion border, Cupid's bow, philtrum
incomplete Fusion of the frontal nasal promises and maxillary prominences = unilateral or bilateral
Microform cleft lip = mild separation
incomplete cleft lip = visible upper lip but does not involve the floor of the nostril
Complete cleft lip = full separation and includes floor of the nostril + pallet and gums
Cleft lip and palate: separation of upper lip and palate + bones and changes shape of the nose
Pallet = 6 to7 weeks of gestation = can involve soft or hard palate
Screening:
During prenatal ultrasounds or genetic testing, check during newborn assessment
Due to bmp4 gene mutation, exposure to infections or toxins during pregnancy or other genetic syndromes
Smoking cigarettes, SUD, folic acid deficiency, DM, Rx (topiramate, valproic acid, phenytoin, steroids, isotretinoin(for acne))
The first trimester of pregnancy is very important since the lip and palate develop during that period.
Lip and nose development occurs between weeks 3 and 6 of gestation.
The palate develops between weeks 4 and 12 of gestation.
Since the structures develop independently of each other and early in the gestational period, gestational maternal exposure to hazards can cause the development of either or both of these conditions.
Lab / dx
Inspection or palpate w/ glove finger but can be detected until later in life → speech therapist for feeding assessment + Imaging
S/s: feeding, latching, sucking, swallowing difficulties → drooling
Ear infections and earring loss, Dental crowding , gum disease
Tx:
cheiloplasty (reconstruct upper lip) within 1st months (cleft lip)
Palatoplasty: around 6 to 12 months
Feeling specialist and lactation Consultants, ENT specialist ( ~ ear and eustachian tube problems)
Dental Care, Orthodontic Care to realign teeth, speech and language specialists
Modified feeding methods w/ special bottles / nipple/tubes/ pacifiers; spoon feeding ; using syringe
Avoid manipulation or touching cleft lip unless for cleaning or medical procedures
→ gently clean cleft lip or palate w/ sterile saline
oral prosthetics until sx
Social worker will help to pay the sx
Appendicitis
Inflammation of vermiform appendix
Due to blockage of lumen of the appendix = ohard stool, lymphoid hyperplasia, foreign body → traps bacteria, thrombosis, necrosis, perforation → peritonitis
→ decrease blood supplies → localized abscess and Frank peritonitis
Fecalith(hard, Stone like Mass made up of hardened fecal material), appendicolith (classified deposits and harder than masses) lymphoid hyperplasia. E coli, steptococcus, bacteroids, pseudomonas
Risk:
10- 19, male, prior abd sx, infection, family hx, cystic fibrosis
S/s:
Abd pain = diffused vague pain around umbilicus → lower right side of abdomen = Mcburney's point
From diffuse to localize, pain worsens w/ movements; guarding and protected inflame appendix
Loss of appetite, n/v, constipation, fever
Rebound tenderness in RLQ (increase pain during palpation), RLQ pain from LLQ
Auscultation 1st then palpation
Sudden cessation of pain = perforation → start getting ill peritonitis develops
After 48 Hours of s/s, risk of perforation increases
Indications of a Ruptured Appendix
Sudden onset of tachycardia or fever
Severe abdominal pain that is unrelieved by medication or nonpharmacological pain control methods
Rigid, board-like abdomen
lab/dx:
WBC, immature cells, CBC, CMP, CRP,
U/a to rule out other conditions, Imaging tests to look for free fluid, enlarged appendix diameter, thickness of appendices wall, abscess/ CT scan = goldeb
Tx: appendectomy within hours; laparoscopic sx or open sx if appendix abruptured
ABX administered before sx and after sx (cefoxitin) , pain management
No heat to abdomen, pull legs to the chest, deep breathing or distraction, avoid strenous activity
Can be confused by PID if sexually active female
Surgical site instructions, avoid heavy lifting for 4-6 weeks
GERD
weak or underdevelopment LES, → prolonged or severe GER and cause irritation and inflammation
screening: Gastrointestinal and Gastroesophageal Reflux (GIGER) scale or Infant Gastroesophageal Reflux Questionnaire-Revised (I-GERQ-R),
overfeeding, diet consisting a lot of greasy or highly acidic food, health condition, weaken muscle tone, poorly developed or weak esophageal sphincter
(citrus, caffeine, chocolate peppermint, spicy or fried food, soda) or vigorous activities.
risk:
genetic, family hx, premature, hx of esophageal atresia repair obesity, CF, asthma, cerebral palsy, second hand smoking
poverty, lack stim, physical punishment, parental mental health, SUD
s/s:
heartburn, regurgitation, spit up/vomit after eating. nausea, noncardiac chest pain, swallowing problems, decreased appetite, sore throat, hoarseness, dental issues, halitosis, poor weight, FTT
infants cry excessively and arch their backs; resp distress, chronic coughrs
aspiration= , wheezing, stridor, apnea, apparent- life-threatening event / ALTE (sudden, alarming change in behavior, such as choking, temporary cessation of breathing, color change, or marked limpness.)
arch back = sandifer syndrome
tx:
Subjective: verbalized by the parents or client or related to behavior
Heartburn/burning, noncardiac chest pain
Regurgitation/spit-up/vomiting
Hematemesis
Poor appetite or refusing food
Recurrent inconsolable crying or irritability
Hoarseness, sore throat, trouble swallowing
Chronic cough, wheezing, ALTE
Sleep disturbances
Objective: observed or measured by health care providers
Esophagitis, esophageal stricture
Recurrent desaturation
Aspiration pneumonia
Laryngitis
Recurrent otitis media
Unexpected posturing/Sandifer syndrome
FTT/weight loss
Dental erosions or halitosis
→ esophagitis, esophageal erosions/ strictues, feeding difficulties
sleep disturbance, pain, frustration,
affect speech and language development
lab/dx:
upper GI XR , 24hr ph intraesophageal study = measures amount of reflux, upper GI endoscopy involves biopsy, detects esophagitis + strictures
pH probe = inserted to nose through esophageous = measure activity -
tx:
keep pt upright after feeding, smaller and more frequent feedings, avoid trigger foods/ overeating.
PPI *omeprazole / histamine antagonist (famotidine)
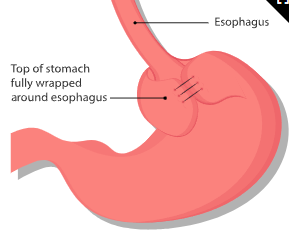
sx intervention = gastrostomy, Nissen fundoplication
prop themselves while sleeping, elavate using wedge under their mattress, reduce weight
4yr < chewing gum
30 degree angle for 30 mins or place on their backs to sleep, remove bedding and soft objects, not prop feeding
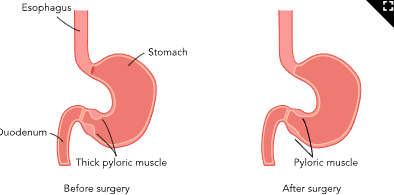
pyloric stenosis
narrowing of pylorus → projectile vomiting → dehydration/ weight loss
due to hyperplasia (inc mass), hypertrophy (inc size), pyloric valve dysfunction, stenosi,s thickening of pyloric muscle layers = infantile hypertrophic pyloric stenosis (IHPS)
more in family hx, erythromycin and maternal smoking
premature, firstborn, young parents <20yr, low maternal education, 2-8 weeks old. Maternal smoking during pregnancy, bottle-feeding
s/s;
healthy at birth → projectile vomit (non bilious, intermittent, worse after eating )
constant hunger, poor weight gain, abd distension, persitaltic waves, palpable olive shaped mass in RUQ, change in BM
lab/dx:
CMP, ABG metabolic alkalosis,
US (gold for imaging) = check pyloric wall thickening/ length, or signs that gastic is not emptying
tx:
IV hydration
pyloromyotomy: muscular wall incision = made above navel, tight pyloric muscle is repaired,
post op is expect to experience vomiting for several days due to swelling in pyloric muscle → clear liquids by 24hrs → regular feedings within 2-3days → discharge = tummy time
know difference between spit up and vomiting
GI Bleed
ligament of Treitz
upper are proximal, lower are distal
reflex and ulcers cause erosion to lining = exposing blood vessels
inflammatory diseases = ulcer, sores, bleeding,
Meckel’s divertculum (congenital outpouching) = acid secretion
portal HTN = esophageal varices
NSAIDs = clotting dysfunction
indomethacin( inhibit prostaglandin + fetal GI lining), ASA, cephalothin ( alter GI bacteria), phenobarbital ( affect blood clot)
upper GI: peptic ulcers, GERD, esophagitis, gastritis, foreign injection, post op complications, Mallory-Weiss tears (occur in mucous membrane in lower part of esophagus or upper part of stomach)
lower GI: infectious colitis, Meckel’s diverticullum, ischemic colitis, IBS, fissures, constipation that causes anal tears, poisoning, sexual abuse, rectal varices, food intolerances
foods that give bloody stool appearance : abx, red candy, chocolate, iron, floavored drink, gelatin, bismuth containing Rx
risk: NSAID, coagulation disorder, GI infection (H. pylori/ shigella), sx, abd radiation, IBS, food allergy, colitis, liver disease, intestinal polyops, vascular malformations
Common Causes of Upper and Lower GI Bleeds by Age Group
Age Group | Upper GI | Lower GI |
|---|---|---|
Neonate |
|
|
Infants 1 month to 1 year |
|
|
1 to 2 years |
|
|
Children over 2 |
|
|
screening: assess abd pain, vomit, change in bowel habits, hemodynamic instability (resting tachycardia orthostatic hypotension)
s/s:
hematemesis, melena (strong odor due to enzymes and bacteria digesting Hgb) in upper Gi
hematochezia (bright red) = lower GI
high HR, low BP, abd pain, anemia, dizzy, paleness, dehydration
can cause stress gastritis w/ premature birth, intubation, mechanical vent, neonatal stress
lab:
check stool and blood for pathogen = INR(0.8-1.2), Hgb/Hct, PTT, lactate (3-7 arterial / 5-20 venous), LFT
structural = XR, CT, US, MRI, barium, endoscopy, nuclear scintigraphy (uses radioactive, angiography, Meckel scan
Endoscopy Types Depend on the Suspected Area of Bleeding
An esophagogastroduodenoscopy (EGD) = upper GI bleeding.
A colonoscopy = lower GI bleeding.
A capsule endoscopy = small intestine as the capsule passes through the body.
tx: hydration/ volume support
acute bleed = blood transfusion, intensive care, RX (pantoprazole esomeprazole = suppress acid secretion)
endoscopy + sx to control bleed
Toddlers and preschoolers may only require information right before the procedure.
School-age children younger than 7 should most likely be told the day of the procedure.
Older children may be told days or weeks in advance.
decrease risk of accidental toxic ingestion: secure cabinets, properly dispose medication, no 2nd hand smoke, no contaminated water
IBS
chronic that affects large intestine → functional abd pain disorders (FADP) = when diff body process leads to GI issue → diahrrea, constipation,
from low neuro communication in gut/brain axis → altered motility, visceral hypersensitivity, gut biome, immune, and CNS process
NOT UC, CHRONS, COLLITIS, it does NOT have inflammation/ tissue damage
from strong emotions, abd pain from inc motility = intense and spasmodic “ push/ pull” contraction = intermitten abd pain w/ constipation and diahrrea
high rate of allodynia
IBS-C: Constipation
IBS-D: Diarrhea
IBS-M: Mixed (constipation and diarrhea)
IBS-U: Unsubtyped (combination of IBS manifestations where the pattern does not fit the criteria for other subtypes)
high risk if both parents have disorder, lactose, GI infection, emotional stressm altered gut bio, vitamin D deficiency, abuse, underlying mental health conditions
high fat/ low fiber, food intolerance (lactose, sorbitol, fructose, or gluten)
s/s: recurrent abd pain → diffused unrelated to appetite or activity.
alternating bouts of diahrrea/ constipation, bowel urgency, malaise, nausea, dizzy, anorexia, swell/ bloat, gas, mucous in stool
lab/dx:
comprehensive medical history, physical examination, s/s
pain w/ 1 day per week for 3 months
WBC, low Hgb, CRP,
fecal calprotectin = leel of inflammation in GI
stool sample, fecal pancreatic elastase for pancreas insufficiency
u/a for UTI, lactose breath if intolerance
XR or US = visualize internal organs
endoscopy = gather tissue sample
tx:
lifestyle modifications, dietary changes:
avoid trigger foods: large meals, fatty foods, lactose (when applicable), caffeine, and artificial sweeteners.
low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAP);
inc fiber (controversial due to causing bloat + gas but help if constipation),
hydration
check labelss
pain management, psych
Rx:
antispasmodic = dicyclomine (anticholinergic) = abd pain/ cramp
antidiarrheals = loperamide
laxatives
peppermint for spasms, abx if bacteria, probiotics,
antidepress/ antipsychotic, CBT for coping, manage stress, (-) though management
gut-directed hypnotherapy or biofeedback
for stress: distraction, guided imagery, relaxation techniques, and breathing techniques.
regulate sensory system w/ playing with tactile materials, water play, or movement-based activities
Inflammatory Bowel Disease
chronic inflammation = disruption in epithelial lining = allows bacteria and certain food proteins into layer → immune response and inflammation
Ulcerative collitis (UC) = mucosal and submucosal inner lining of rectum/ colon
→ diarrhea w/ blood or mucous or pus, abd pain, rectal bleed, bowel urgency, fatigue, weightloss, anemia
→ more blood
Crohns = small and large intestine (entire)
→ patchy pattern → abd pain, diarrhea (w/ or w/o blood), weight loss, fatigue, low nutrition
→ fistulas, anal fissures, abscesses
→ more pain
both include: joint pain and swell, skin rash, eye inflammation, liver disroder, mouth ulcers
IBS Manifestations | Manifestations of Both IBS & IBD | IBD Manifestations |
|---|---|---|
|
|
|
Primary differentiation:
| Primary differentiation:
|
→ can lead to hemorrhage, strictures, toxic megacolon, osteoporosis, anemia, gallstones, deep vein thrombosis, infections, sclerosing cholangitis (progressive scarring and narrowing of the bile ducts → cirrosis), liver failure, and increased risk of colon cancer.
GH resistance
screen:
genetic screen (first degree relative) w/ s/s
inc w/ altered gut, infection, Rx (abx, NSAID, hormonal birth control, isotretinoin), smoke,, high diet in refined sugars and low in fruits/ veggies
lab/dx:
CBC< ESR, albumin level, LFT,
genetic test, anti-Saccharomyces-cerevisiae antibodies (ASCA) = negative (0-20 units)
stool sample = fecal occult blood test (FOBT) fecal calprotectin, stool culture
imaging = endoscopy (colonoscopy, flexible sigmoidoscopy, capsule endoscopy, or balloon-assisted enteroscopy)
tx:
Rx: aminoacylates (mesalamine), corticosteroids, immunosuppress (methotrexate), biologic response modifiers ( etanercept)
enteral nutrition to induce remission = formulated liquids, eliminate trigger
lifestyle modifications: regular exercise, stress management techniques, and smoking cessation, diet
supportive care: psychosocial support, counseling, and educational resources
sx:
colectomy,
proctocolectomy with ileal pouch-anal anastomosis (IPAA) → entire colon and rectum removed and pouched placed in small intestine
Fecal microbiota transplantation
14-18 yr = Rx responsibility
Celiac
wheat include durum, einkorn, emmer, Khorasan wheat, and spelt, bread, pasta, and cereal
~even rice, corn, quinoa, and oats
When in doubt about a restaurant dish, ask how the menu item is prepared. Restaurant dishes can easily be contaminated with ingredients containing gluten.
Gluten can also be found in seasoning, broths, syrups, and other foods that may seem unlikely. Some common examples include the following.
Candy
Chips
Cookies
Croutons
Processed meats
French fries (if the facility does not use a dedicated gluten-free fryer)
Gravy
Sauces
Tomato paste
Imitation foods
Seasoned rice
Condiments
Soups
Soy sauce
Vegetables covered in sauce
body cannot digest gliadin ( glycoprotein in gluten) → excess glutamine = autoimmune → inflammation + digestive enzyme = flattens or atrophies wili and brush border, decrease SA for nutrient and mineral absorption
→ severe diarrhea → weight loss, FTT, protein deficiency, Ca/ vit D low, muscle wasting, ascites, abd distention, dental m osteoporosis, steatorrhea
if untx: autoimmune disorders, neurological disorders, pancreatic insufficiency, colitis, Sjogren’s syndrome, skin conditions, lactose intolerance, short stature, diabetes mellitus, multiple sclerosis (MS), anemia, infertility, osteoporosis, migraine, heart disease, and intestinal cancers.
actively
screen:
celiac diseas, family hx, autoimmune, Down syndrome, DM T1, early introduction to protein solids
serological tissue for transglutaminase antibodies (tTG-IgA) = consume gluten to avoid false negative
mutation:HLA-DQA1 and HLA-DQB1 genes → leukocyte antigen (HLA) complex helps diif own proteins w/ other proteins
s/s:
s/s in 2-4 m after colic foods and grain is introduced → 9-12m = FTT
extremely watery diarrhea, foul-smelling stool constipation, abd pain, fatigue, h/a, painful skin rashes
and distention, irritability, anorexia, muscle waste, anemia, vit deficiency
non-classic = migraines, chronic fatigue, joint pain, rashes
lab/dx:
transglutaminase antibody (tTG-IgA) <20 EU and genetic markers
biopsy of intestines = definitive dx
tx:
lifelong, strict, gluten-free= restore damage to intestines by 2 yrs
replace w/ grains, like rice, corn, soy, chickpea, arrowroot, tapioca starch, flax, and quinoa
and incorporate nutrient-rich foods, like fruits, vegetables, fish, and gluten-free meats.
actively participate in meal plan and grocery shop, food prep
hand hygyene+ cross contamination (wet or sticky supplies will have more ) = creating gluten-free play zones, cleaning play surfaces, and ensuring children wash their hands
gluten-free options at restaurants and communicate their needs to restaurant staff.
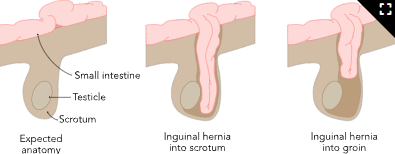
Hernias
organ protrudes through weak spot in and wall → visible bulge or swelling → bowel incarceration or bowel strangulation, ischemia
ingual: undescended testes, genitourinary and chromosomal anomalies, or unilateral ingual hernia
umbilical: autosomal trisomies (21/18), endocrine (hypothyroid), dysmorphic syndromes (Beckwith-Wiedemann syndrome (asymmetric growth) or Marfan syndrome
rare is congenital diaphragmatic hernia (CDH) = !!! from severe resp distress
tachypnea, labored breathing, cyanosis, nasal flaring, retractions, difficulty maintaining oxygen saturation, and a sunken or scaphoid appearance of the abdomen.
diminished or absent breath sounds on the unaffected side.
→ GERD , resp problems, musculoskeletal deformities and neurodevelopmental impairments.
due to increased abdominal pressure, coughing or constipation, and connective tissue disorders, CF
premature birth, low birth weight, and parental or sibling history of a hernia, certain intestinal anomalies of the esophagus or diaphragm
screen:
physcial examination, prenatal US
s/s:
more visible crying, straining, coughing, or passing stool
discomfort, pain, aching, a distended abdomen, vomiting, fussiness, fever, or redness near the hernia site.
ingual: males into scrotum / females: labia majora
umbilical: painless and vary w/ size → more prominent when child strain
Bowel incarceration
Increased pain or discomfort at the hernia site
Swelling or bulging that becomes firm and does not reduce
Redness or discoloration of the hernia area
Vomiting or nausea
Bowel strangulation
Severe pain and tenderness at the hernia site
Sudden increase in the size of the hernia
Discoloration of the hernia area, such as darkening or bluish discoloration
Firmness and rigidity of the hernia mass
Abdominal distention or bloating
Vomiting, especially if it is bilious (greenish-yellow in color)
Fever or manifestations of infection
These manifestations require immediate, emergency medical attentio
lab/dx:
physical s/s → imaging
CDH by prenatal US → CXR + MRI visualize of abd organs in chest cavity to evaluate lungs → ECG
tx:
CDH → intubation, ventilation, suction, umbilical artery catheter, extracorporeal membrane oxygenation (ECMO)
umbilical hernias resolve by 2-4yrs → sx or s/s
ingual = reduce externally or sx
if bowel incarceration or strangulation will require sx
how to reduce it for parents
proper bdy mechanics while lifting, healthy diet to avoid constipation
use words like “bump” or “bulge”/
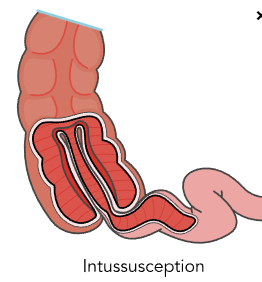
intussusception
common cause of bowel obstruction in 3m - 6yr also after infection
intestine telescopes to it self, usually in small intestine around ileocecal valve → peristalsis propels bowel → edema + obstruction → ischemia / necrosis → hemorrhage, venous engorgement, sloughing iof → mucus and blood in stool → obstruction, bowel strangulation, infection, necrosis, perforation, shock, and peritonitis
from infections, enlarged lymph nodes in intestine, altered motility, anatominal, Meckel’s diverticulum, polyps, CF, celiac, bowel sx,
s/s:
abrupt and severe pain in healthy child,
~ cry/ scream inconsolably and draw knees up to chest → green vomiting of bile or fecal material
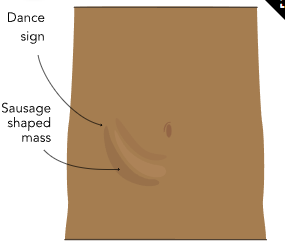
abd distended, red, jelly-like stool, sausage-shaped mass in the upper right quadrant or mid-upper abdomen, Dance sign ( absence of palpable vicesa when examining RLQ) = retraction of cecum away from iliac fossa
→ sepsis/ shock = lethargy; pale, sweaty skin; tachycardia; shallow respirations; fever (or a low temperature in infants); and a decrease in blood pressure
reuccurs within 24hr
lab/dx: hx w/ XR, US (preferred)
contrast enema dx +tx since uses hydrostatic pressure from air moves bowel back (w/ those who have ED)
tx:
1st: barium, water-soluble, or air-contrast enema (hydrostatic reduction).
hydrostatic: is placed in rectum and backwashes into ileum
sx if reduction still shows, sepsis/ shock/ peritonitis, s/s for more than 24hrs (fatal if more than 2-5 days)
manual reduction by milking through bowel → if unsuccessful, or bowel strangulation = sx will remove affected bowel segment
ED
anorexia nervosa (AN),
bulimia nervosa (BN),
binge eating disorder (BED).
pica,
rumination disorders: regurgitate and rechew digested food
avoidant or restrictive food intake disorders (ARFID): avoidance to certain foods
from neurotransmittion disruption = dopamine, serotonin, norepinephrine from hypothalamus and corticolimbic, frontostriatal systems
→ impairs: reward processing, emotional regulation, appetite control, and the dopamine pathway → distorted body perception, fear of weight gain, maladative food choices, altered appetite, struggle finding pleasure, rigid eating and exercise behaviors
→ malabsorption, malnutrition, impaired GI motility, delayed gastric emptying, and slow digestive transit time + vomit or laxative = heart arrhythmias
screening in yearly check ups in 9-18yrs w/ questions:
Tell us about a time when you were at your lowest and highest weight. What age were you at this time? What was your height during this time?
Are there body areas that cause you stress?
How often do you think about your body, appearance, or food during the day? Do these thoughts distract you from daily life?
Do you feel stress or anxiety when you do not have time to exercise?
Do you use laxatives, diuretics, diet pills, or caffeine?
Is there a family history of eating disorders?
Do any of your family members have mental health conditions, such as anxiety, depression, or obsessive-compulsive disorder?
Have you and your family been experiencing any stressful events?
Is school challenging for you?
Have you experienced any bullying?
Do you smoke cigarettes, chew tobacco, vape, drink alcohol, or take illicit drugs?
Do you have any feelings of depression or hopelessness?
by mental health disorders (including anxiety in childhood), negative early feeding experiences, adolescence, cultural ideas about beauty, adverse childhood events, perfectionism, and negative self-image
s/s:
eating habits/ food rituals, preoccupation w/ food and calories, restrictive eacting patterns, distorted body image
for males =leanness, weight control, athletic build, and muscularity. w/ purging, muscle build supplement, depression, SUD
→ esophagitis and gastric ulcers, GERD, heartburn, damage to the esophageal lining, and problems with digestion and absorption, all while leading to bloating, constipation, and electrolyte imbalances.
Low body weight, weight loss, or failure to make expected weight gain
Heart arrhythmias, dizziness, and fainting
Drastic weight change (weight fluctuations or rapid weight gain may cue binge eating or BN)
Malnutrition, fatigue, muscle weakness
Amenorrhea = delay puberty and problems w/ fertility
small tests, low testosterone →erectyle dysfunction + reduced sperm count
Decreased body temperature or low resting blood pressure (BP) or resting heart rate (HR) (energy restriction)
Unexpected orthostatic vital signs (systolic BP drop greater than 20 mm Hg, a diastolic BP drop greater than 10 mm Hg, or tachycardia)
Bone thinning
Anemia
Brittle hair and nails
Jaundice
Esophageal mucosal damage from self-induced vomiting
Manifestations and Traits of Eating Disorders
Type | Traits |
|---|---|
Anorexia nervosa |
|
Bulimia nervosa |
|
Binge-eating disorder |
|
Avoidant/restrictive food intake disorder (ARFID) |
|
Other specified feeding or eating disorders | Examples of eating disorders that do not completely align with the criteria for the other eating disorders above include:
|
lab/dx:
CBC. CMP, kidney + liver, vit, mineral, U/A, ESR, testing for celiac
Hormone levels (gonadotropin, estradiol, prolactin, testosterone, cortisol, thyroid)
Testing stool for parasites
Electrocardiogram (ECG) (with orthostasis or bradycardia)
Bone density tests
Imaging of the brain or GI tract
Pregnancy test for females
tx:
healthy eating patterns w/ healthy growth,
tx plan w/ replenishing nutrition, CBT, FBT, support groups,
or hospitalization → HEADSS = home, education, activities, dru/sex, suicidality/depression
disclose illnes for dentist , topical fluoride Rx for enimal erosion