2. Infectious Conjunctivitis
Conjunctivitis
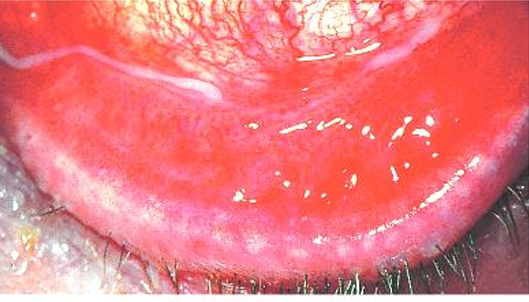
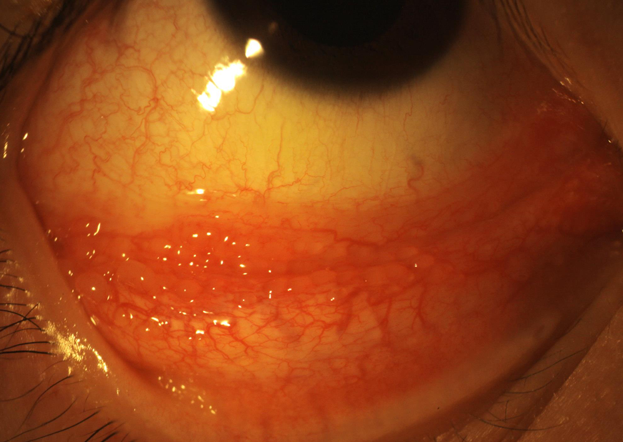
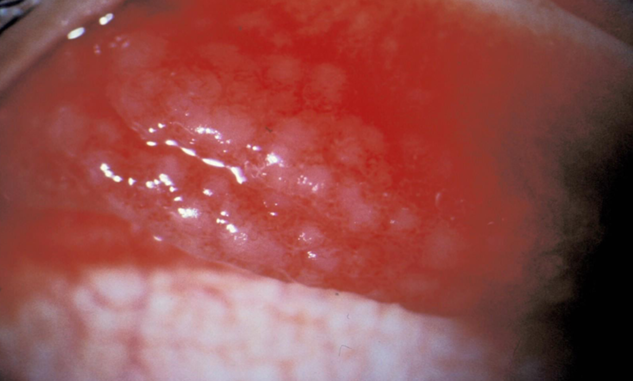
Bacterial Conjunctivitis
Rapid onset (usually unilateral).
Tearing, irritation, grittiness, foreign body (FB) sensation.
Vascular engorgement: beefy red appearance that fades towards the limbus (not fully true - can be diffuse) .
Thick mucopurulent discharge, leading to crusted and oedematous lids.
Fellow eye involvement typically occurs within 2-3 days.
Possible mild corneal involvement, such as superficial punctate keratitis (SPK) or peripheral infiltrates.
Common Organisms:
Staph aureus
Staph epidermis
Other gram-positive cocci like Strep pneumoniae
Moraxella
Hemophilus influenzae

Management
Usually a self-limiting disease, resolving in 10-14 days with natural tears and mucous.
Topical broad-spectrum antibiotics can expedite resolution in 1-3 days.
Lid and eye cleaning are important.
Highly contagious, requiring simple hygiene precautions to prevent transmission.
Chloromycetin 0.5% (Chlorsig, chloramphenicol) (S3) - Bacteriostatic
Days 1 & 2: every 2 hours (q2h) - 1 drop
Review in 48 hours
Days 3-7: every 6 hours (q6h) - 1 drop, 4 times a day
Do not patch the eye
Alternative: Soframycin (Framycetin) 0.5%, 2 drops every 1-2 hours, then 2-3 drops every 8 hours (q8h).
Chronic Bacterial Conjunctivitis
Often associated with underlying lid disease.
Manage the underlying lid disease.
If non-responsive or with persistent recurrence, consider lid cultures.
Chlamydia
Caused by Chlamydia trachomatis (often called the "silent disease").
Sexually transmitted disease (STD) affecting the urethra in males and the cervix in females.
Manifestations in the conjunctiva:
Ophthalmia neonatorum (conjunctivitis in newborns)
Adult inclusion conjunctivitis
Trachoma
Notifiable disease due to its public health significance.
Ophthalmia Neonatorum
Conjunctivitis occurring in the first 4 weeks of life.
Typically secondary to chlamydia, gonococcus, or other bacteria acquired during birth; rarely due to Herpes simplex.
Prophylaxis involves erythromycin ointment.
Rare but serious emergency:
Gonococcus can lead to corneal perforation.
Chlamydia can lead to pneumonia.
Herpes can lead to encephalitis.
Characterized by the absence of follicles.
Variable postpartum onset:
Chlamydia: 5-14 days
Gonococcal: 1-2 days
Longer for HSV and other bacteria.
Neonatal Chlamydial Conjunctivitis Treatment
May be associated with otitis, rhinitis, and pneumonitis.
Presents between 5 and 19 days after birth.
Manifests as mucopurulent papillary conjunctivitis.
Treatment includes topical tetracycline and oral erythromycin + referral

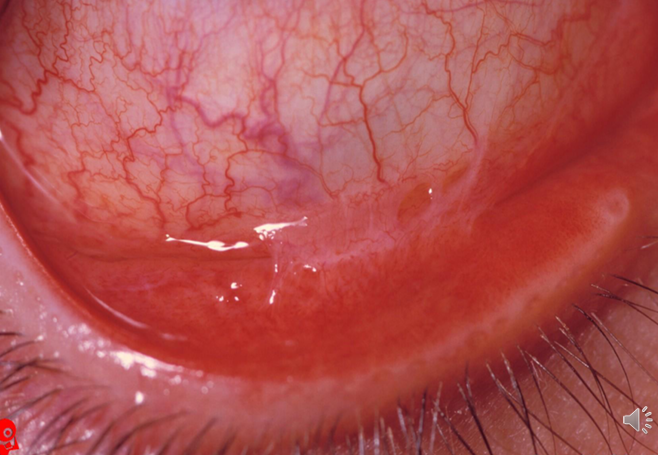
Adult Inclusion Conjunctivitis
Sexually transmitted disease (STD).
Patients are generally young and sexually active.
Approximately 50% or more also have pelvic inflammatory disease (potentially asymptomatic).
Affects the cervix in females and the urethra in males.
About 1 in 300 individuals with genital chlamydia will develop conjunctivitis.
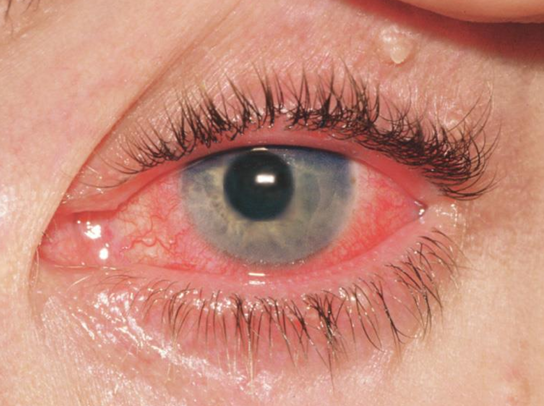
Symptoms:
Maybe unilateral or bilateral.
Red, irritated eye.
Watery to mucopurulent discharge.
Possible slight lid oedema.
Preauricular lymphadenopathy - tender swelling near earlobe
Palpebral conjunctiva initially shows a papillary reaction, followed by the development of large follicles, mostly in the inferior fornix but also possibly on the upper tarsal surface.
Keratitis is possible around week 2, with subepithelial infiltrates, marginal infiltrates, and superior limbal pannus.
Can become chronic, lasting for months.
Management
Referral to an STD clinic for investigations (as it is a notifiable disease).
Topical and systemic therapy:
Tetracycline ointment.
Oral azithromycin (1000mg single dose).
Doxycycline (100mg every 12 hours for 7-10 days).
Erythromycin (250-500mg every 6 hours for 3 weeks).
Case study - 23 yr old male
myope
good vision in each eye with rx
red irritable eyes
discharge evident on waking
duration three months
no pain or photophobia
\Diagnosis: adult inclusion conjunctivitis
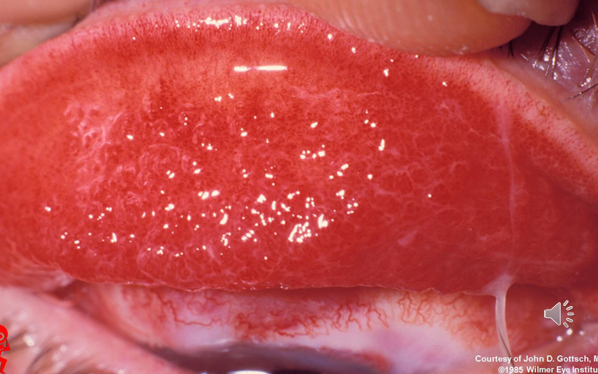
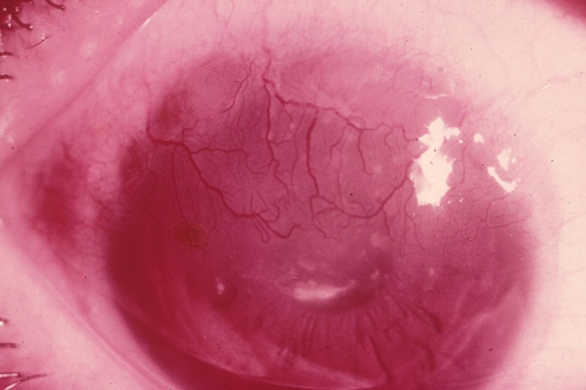
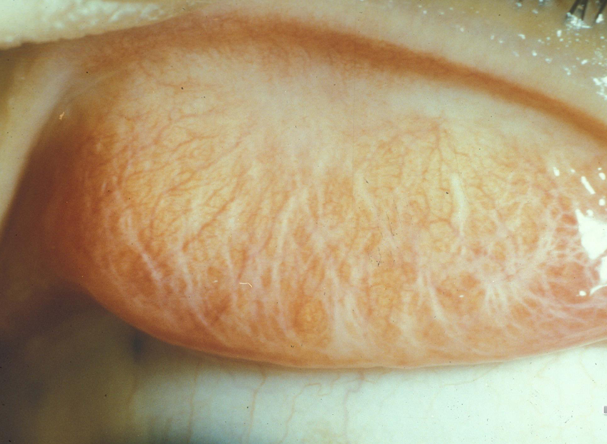
Trachoma
First presentation: mild, mucopurulent, self-limiting conjunctivitis.
caused by chlamydia
Chronic inflammation; leads to chronic follicular conjunctivitis, papillary hypertrophy (especially on the upper tarsal conjunctiva), pannus, and epithelial keratitis.
Repeated infections result in:
Scarring and cicatrization of the cornea, conjunctiva, and eyelids (entropion and trichiasis).
Linked to poor hygiene conditions, including sanitation issues, crowded living, and livestock proximity.
Flies serve as a major vector in the cycle of transmission.
Leading cause of preventable blindness worldwide.
WHO estimates: don’t need to memorise
146 million with active disease
10 million with trichiasis
6 million blind
Treatment
Single oral dose of azithromycin.
Hygiene improvement (clean water, fly reduction).
Control of trichiasis.
SAFE Strategy (WHO)
Surgical management of trachomatous trichiasis.
Antibiotics.
Face washing to interrupt trachoma transmission.
Environment change (water, fly control, sanitation, managing cattle and crowding).
Prevalent in Africa, the Middle East, Latin America, Central and Southeast Asia.
Australia was the only developed country to still have endemic blinding trachoma.
Trachoma in Australia:
Primarily affects remote and very remote indigenous communities in the Northern Territory, South Australia, and Western Australia.
The National Trachoma Management Program was initiated in 2006 in Australia to enhance trachoma control, health promotion, and environmental improvement initiatives.
Viral Keratoconjunctivitis
Adenovirus
Molluscum contagiosum
Adenovirus
Ranges from mild to severe ocular involvement:
Follicular conjunctivitis
Pharyngoconjunctival fever
Epidemic keratoconjunctivitis (EKC)
Incubation period around 5-12 days
Clinical illness for about 5-15 days
practitioner hygiene to avoid spread - incredibly contagious. If someone in practice is suspected to have it - ensure proper cleaning of clinic (thorough).
Virus killed by alcohol
Follicular Conjunctivitis
Mildest form of adenovirus
Unilateral initially (spread to other 1-2 days)
Bilateral approx 60% cases
Watery discharge
Conjunctival hyperaemia
Mild to moderate burning sensation
Follicular response
Lymph node involvement
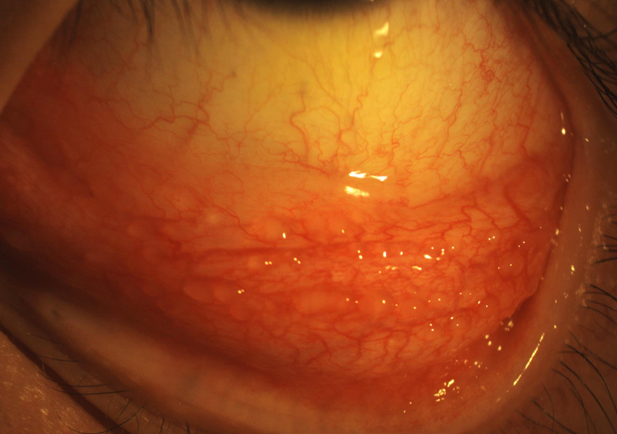
EKC: Epidemic Keratoconjunctivitis
Severe and highly contagious - disinfect slitlamps, tonometers, droppers etc.
Usually not associated with systemic symptoms, but may be low-grade fever with lymph involvement
Usually 7-21 day course
EKC Disease Course
First few days - hyperaemic palpebral conj with fine papillae
Develops into: ~ 1 week
Follicular conjunctivitis in the lower fornix in the first week, later may involve the tarsal surface
Watery discharge, hyperemia, chemosis
Preauricular lymphadenopathy
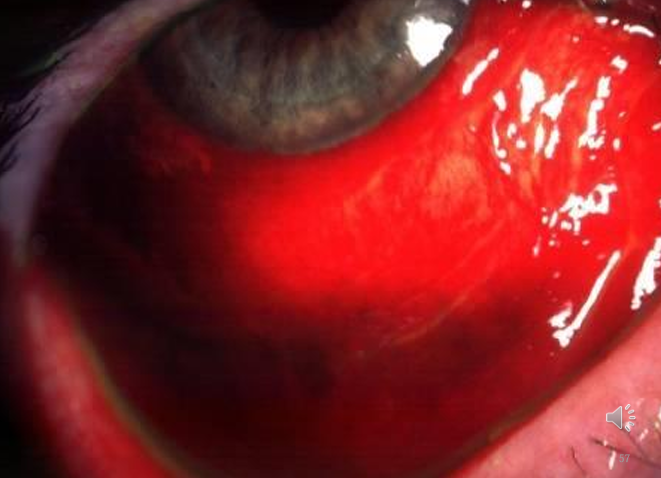
Subconj haemorrhage, lid oedema
Membranes (1/3 cases) - can cause conjunctival scarring and symblepharon
Corneal involvement:
Diffuse, fine, superficial keratitis (1st week)
Focal, elevated, staining epithelial lesions (FB sensation) (days 6-13)
Sub-epithelial opacities develop (day 14)
Epithelial changes may last 4-6 weeks
Subepithelial changes may last weeks - months - years
Pharyngoconjunctival Fever
Generally associated with adenovirus 3 and 7
Pharyngitis, follicular conjunctivitis and fever (URTI)
Preauricular adenopathy (90% cases)
Usually self-limiting over 5 - 14 days
Follicular conjunctivitis, scant watery discharge, conj hyperaemia.
often bilateral (systemic)
EKC and PCF Management
Treatment is primarily supportive
Usually resolves in 2 weeks
Cool compresses and lubricants
Antiviral drugs found ineffective
Topical antibiotics only reduce the risk of secondary infection - not necessary
Review in 5 days
No CL wear until 1 week after corneal signs disappear
Topical steroids WITH CAUTION (ophthalmologist?) - if vision is affected
Topical steroids inhibit or reduce the appearance of subepithelial infiltrates.
Infection control
EKC and PCF Management Infection Control: minimise outbreaks
Hand hygiene between patients; accessible to all staff in the practice.
Clean all equipment surfaces between cases with neutral detergent.
Staff instructed that patients with red eyes should not undergo preliminary examination procedures until the clinician has been consulted.
Single-dose vials of diagnostic drops to be used and discarded.
Tonometry - consider disposable tonometer prisms; disinfect reusable prisms with isopropyl alcohol swabs and air dry between patients; decontaminate at the end of a clinic session by soaking for 10 minutes in 0.05% sodium hypochlorite solution, then rinse and store dry (NSW Department of Health, June 2006).
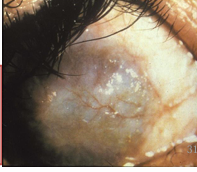
Molluscum Contagiosum
Oncogenic virus (pox virus)
Characteristic nodule on lid margin:
Single or multiple
AIDS patients - multiple lesions
Characteristics
Small pale waxy umbilicated nodule - passes toxins into the conjunctiva
May be distant from lid margin
Mild mucoid discharge
Conjunctival follicular response on side of lesion
Epithelial keratitis and even pannus in long-standing cases

Molluscum Contagiosum Treatment
Refer for destruction of lid lesion:
excision
cryotherapy
cauterization
Benign Folliculosis
Common in children
Follicles in the inferior cul-de-sac without any other signs or symptoms of conjunctivitis
Disappear with age
can be bilateral
no treatment required