Trauma and PTSD
History of PTSD diagnosis
- railway spine - 19th century
- shell shock - WWI
- concentration camp syndrome – WWII
- Vietnam War
- PTSD diagnosis first defined in DSM III in 1980
\
What do we mean by trauma?
- Dictionary → “a deeply distressing or disturbing experience.”
- DSM 5 (Criterion A): exposure to death (of others), threatened death (self/others), actual or threatened injury or sexual violence
* Includes:
* direct exposure, witnessing, or learning of a close other being harmed/exposed to trauma
* repeated exposure in course of professional duties (e.g. first responders, medics, journalists)
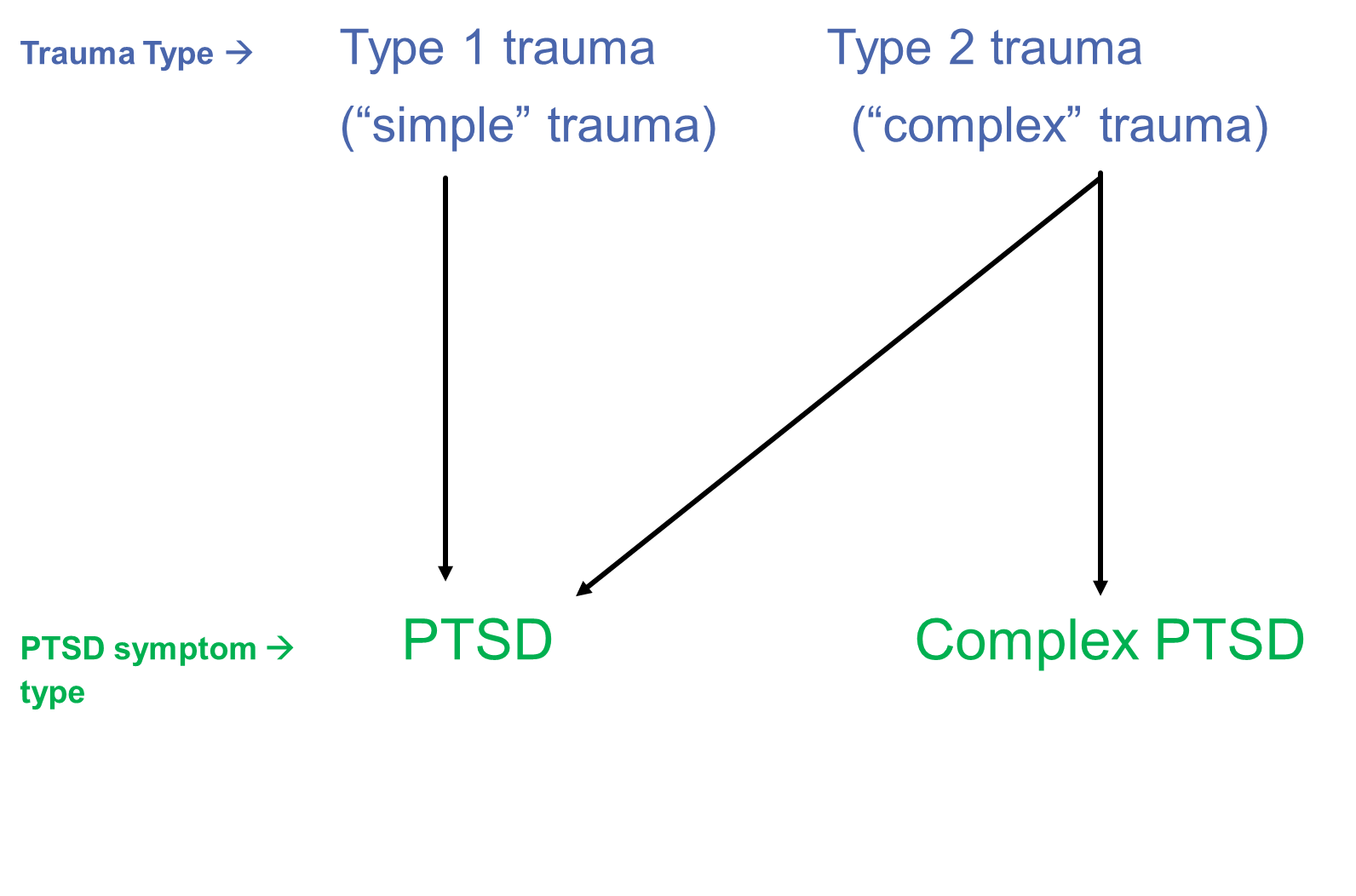
* ‘==Type I’ (‘simple’)== vs ^^‘Type II’^^ (‘complex’ trauma → the distinction between ==a discrete/isolated traumatic event== vs ^^chronic/repeated/prolonged traumatic events^^ (e.g. domestic violence, childhood sexual abuse, trafficking, torture)
* Different psychological impact of chronic trauma exposure?
*
Types of traumatic experiences
1. Natural disasters (i.e. earthquakes, tornados, volcanos) 2. Fire/explosion 3. Combat /War (as a soldier or civilian) 4. Transport accident (e.g. boats, trains, cars, planes) 5. Serious/life-threatening accident or illness 6. Physical assault/abuse (with or without weapon) 7. Sexual assault/abuse (including in childhood) 8. Torture 9. Witnessing death of others/learning of death of a loved one
- Severe human suffering
PTSD is only one possible outcome
 Responses to trauma
Responses to trauma
- Nature of the traumatic event/sequalae (both emotional (e.g. shame, guilt) but also physical (e.g. physical injuries/permanent change)
- Person’s environment/safety after the trauma
- Past experiences
- Existing coping strategies
- Personality factors
- Attributional style
- Cultural experiences/beliefs
\
Can we prevent PTSD?
- still an ongoing investigation…
- Hard to find factors that consistently predict who will be at risk of developing long-term PTSD symptoms.
- Some research suggests important factors may be: * Mental defeat (i.e. mentally giving up during the trauma- perceived loss of dignity, autonomy, sense of being human (Dunmore, Clark, & Ehlers, 1999, 2001)). * Rumination about the trauma * Pre-existing/family history of mental health difficulties * Symptom severity/Acute Stress Disorder * Peritraumatic dissociation (?risk to life/trauma severity) * Post-trauma social support
- Tetris Experiment * Risks of ‘psychological debriefing’ – not recommended in NICE guidance * ‘Watchful waiting’ is important
\
Other possible reactions after trauma
- Acute stress disorder
- Adjustment disorder
- Grief/persistent complex bereavement disorder
- Depression, anxiety, OCD…. Many different mental health problems
- No mental health problems
\
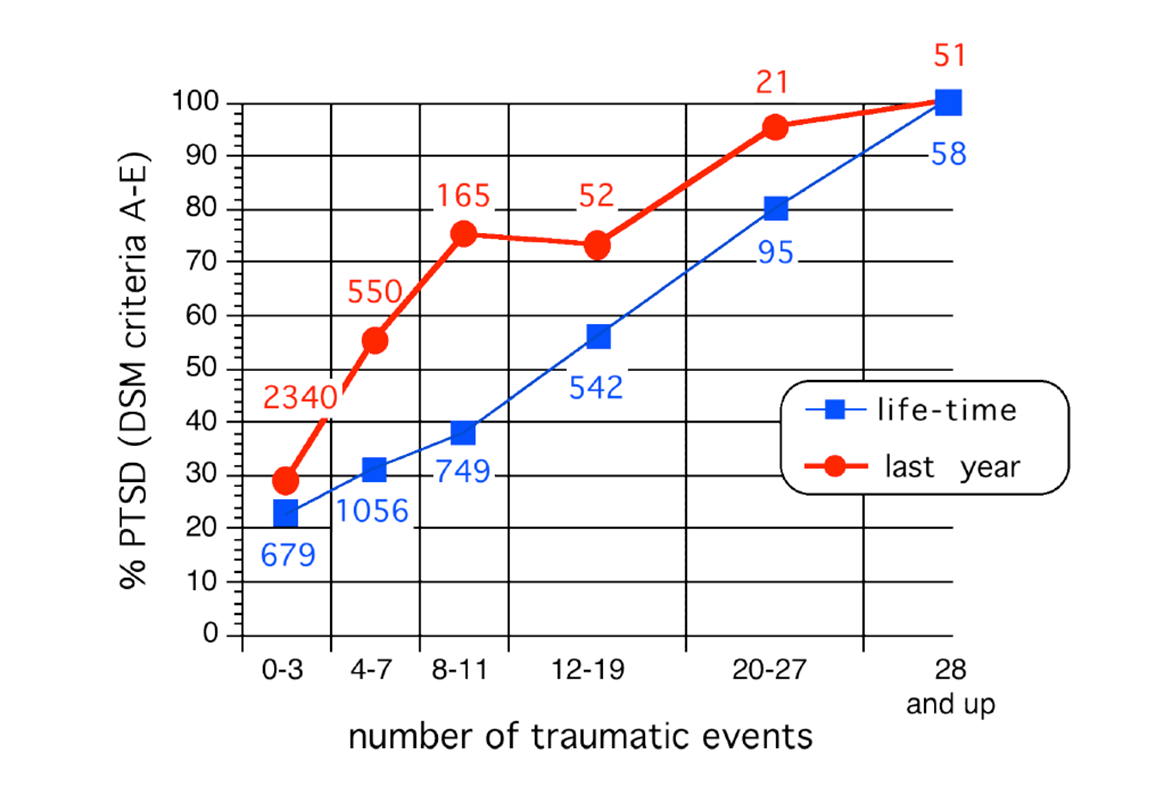
‘Building block effect’ → Schauer et al. (2003)
- With repeated exposure to trauma, the likelihood of a person having PTSD increases
- After 28+ traumatic events, almost everyone will have symptoms consistent with a diagnosis of PTSD
Post-traumatic Stress Disorder (DSM-5)
- Must have been exposed to a trauma * e.g. death (of others, threatened death (self/others), actual or threatened injury or sexual violence * Includes direct exposure, witnessing, or learning of a close other being harmed/exposed to trauma, repeated exposure in course of professional duties (e.g. first responders, medics, journalists)
- Symptoms (a month post trauma): * Re-experiencing * Avoidance * Negative alterations in cognition and mood * Alterations in arousal and reactivity * Impairment in functioning
\
Common reactions to trauma in children
1. not wanting to sleep alone 2. being afraid of things that are reminders of the trauma 3. crying and clinging (worried) 4. unusual aches and pains 5. regressive behaviours 6. aggressive play (may re-enact the event) 7. being confused about the trauma and its meaning 8. being worried and/or confused about death 9. trouble concentrating and doing school work
- worries about safety of others
- shame or guilt about what they did or didn’t do
- worry about the future “If I grow up”
- worry about how parents react to the trauma
\
Complex PTSD
- More likely after extreme, prolonged traumatic events where escape is impossible * For example, imprisonment, torture, trafficking, domestic violence, childhood abuse
- Symptomatology and impact is often different
- Not officially recognised as a diagnosis until now – ‘clinical consensus’ * Recently added to ICD-11 (2022)
Diagnostic Criteria
- Core symptoms of PTSD plus disturbances in self-organisation: * affect dysregulation: * heightened emotional reactivity * anger * recklessness * numbing * dissociation. * negative self-concept: * feeling diminished * defeated and worthless * feelings of shame * guilt or despair. * disturbances in relationships * difficulties engaging and maintaining/sustaining relationships * difficulty feeling close to others * little interest in engagement in relationships.
Cross-cultural validity of PTSD diagnosis
- Debate about the relevance of PTSD diagnosis to non-Western populations * (e.g. for refugees) (e.g. Summerfield, 2001; Patel et al., 2016)
- Good evidence cross cultural validity PTSD diagnosis * (e.g. Hinton and Lewis-Fernandez, 2011, systematic review to advise DSM-5)
- But there are some cross cultural variations in expression/presence of some symptoms, and different ideas about how to treat/recover from trauma
\
Emotional Processing Theory - Foa & Kozak (1985, 1986)
- Fear networks in memory to facilitate our escape from danger or threat
- Network contains information about: * the feared stimuli * our fear responses (e.g. physical/emotional reactions) * thoughts/meaning associated with feared stimuli * thoughts/meaning associated with our own responses
- Realistic threat > ‘normal fear’
- Fear network becomes problematic (‘abnormal fear’) when: * the information does not accurately represent the world * physical and escape/avoidance responses are triggered by harmless stimuli * harmless stimuli/responses are perceived as dangerous * fear responses interfere with daily functioning
- To reduce ‘abnormal’ fear, we need to activate the network and then provide ‘realistic’ information to replace the faulty information in the structure > Prolonged exposure therapy
\
Dual Representation Theory - Brewin, Dalgleish & Joseph (1996)
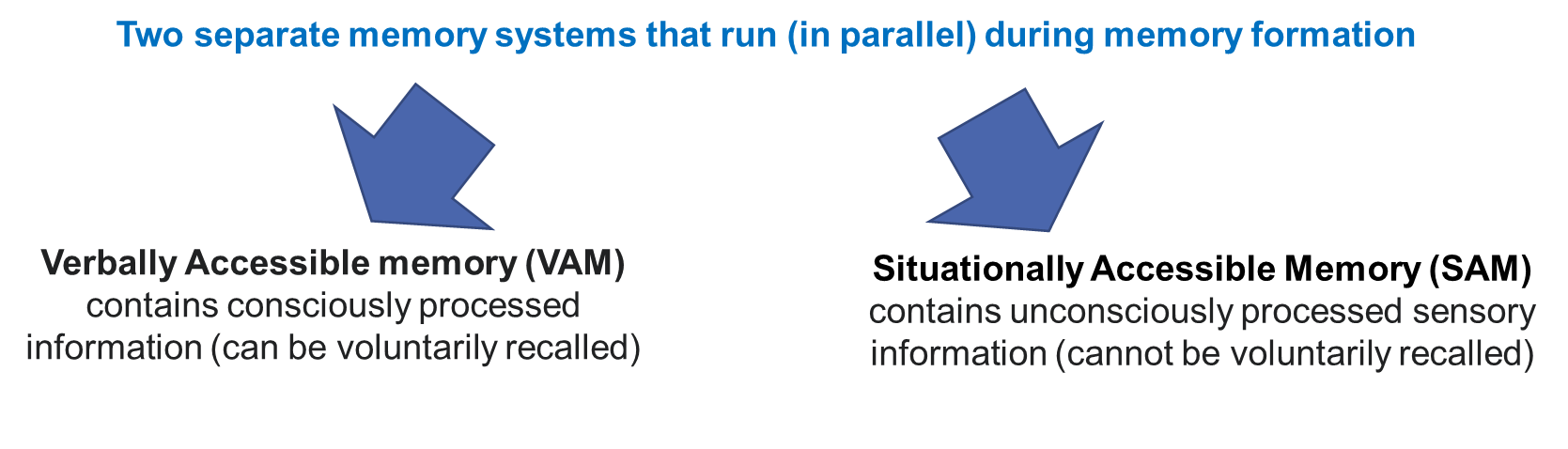
- During a trauma: * VAM system is impaired (conscious attention is focused on the threat). * SAM system captures vivid sensory information during the traumatic event
> later automatically recalled through exposure to trauma-related triggers (i.e. re-experiencing symptoms).
\
What types of treatments have good evidence for PTSD?
- Trauma-focused treatments * Trauma-focused cognitive/cognitive-behavioural therapy * EMDR (Eye movement reprocessing and desensitisation) * Narrative Exposure Therapy (NET) * Prolonged exposure
- drug treatments are NOT ‘first line’ treatments and are usually prescribed to manage symptoms (i.e. they do not necessarily tackle ‘underlying cause’ of symptoms).
\
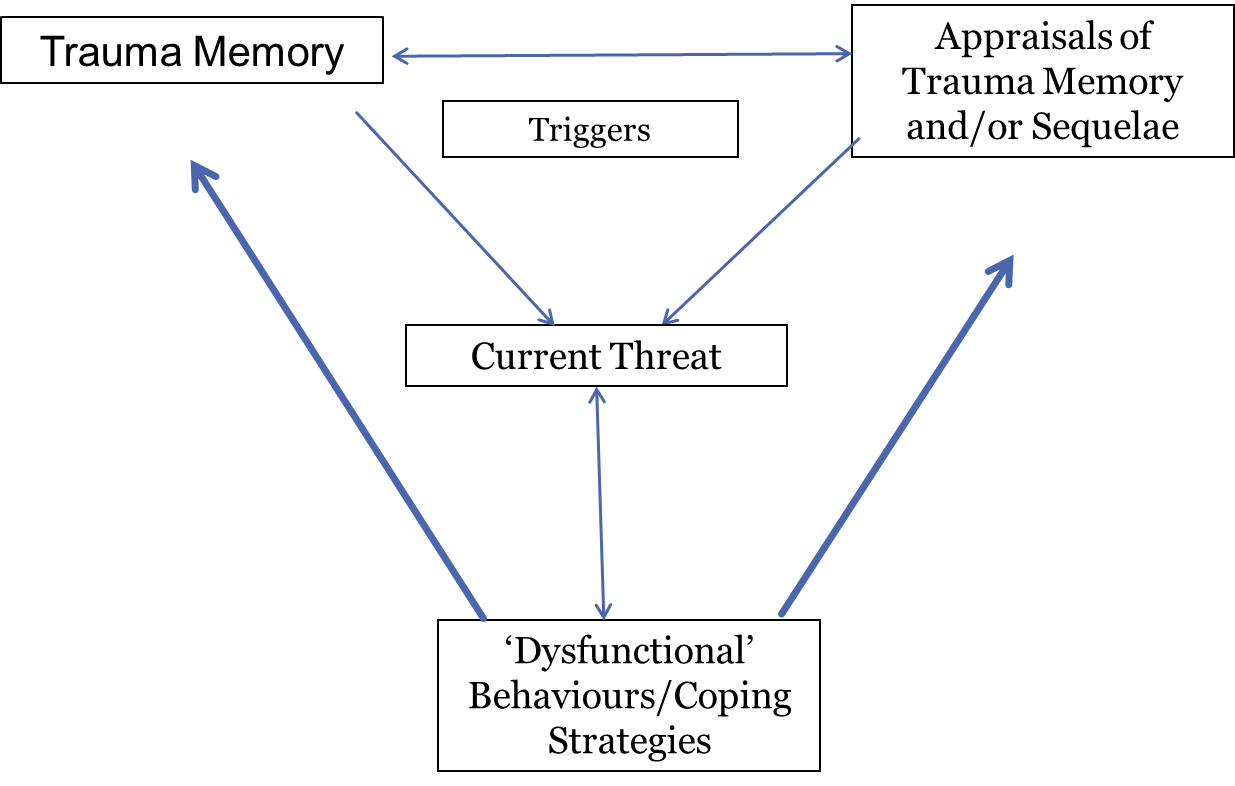
Cognitive Model of PTSD - Ehlers and Clark (2000)
 TfCT overview
TfCT overview
- Formulation/psychoeducation and introducing ‘Reclaiming Life’
- ‘Reliving’
- Identification of ‘hot spots’
- Cognitive restructuring of hotspots
- modifying negative appraisals (developing ‘updates’ for hotspots)
- Site visit
- Behavioural experiments (to drop safety-seeking behaviours/cognitive strategies)
- Stimulus discrimination
\
Other types of tf-CBT
- Cognitive Processing Therapy (CPT) * group or individual intervention, often used for survivors of sexual assault/domestic abuse. * Involves a detailed written narrative of traumatic event * Resick & Schnicke (1992)
Prolonged Exposure (PE)
- therapist supporting the client to: * engage with in vivo and imaginal exposure to trauma reminders with the goal of reducing their avoidance in relation to trauma-related stimuli * to promote ‘extinction’ of the conditioned fear response. * McLean & Foa (2011)
\
EMDR
- Client asked to recall traumatic event whilst implementing ‘bilateral stimulation’ * e.g. eye-movements; tapping, audio stimulation/tones
- Hypothesis that EMDR therapy facilitates retrieval of the traumatic memory network and enhances information processing. * Aim: new associations are made between the trauma memory and more adaptive memories or (new) information * complete information processing * new learning * reduction of emotional distress * new cognitive insights
Overview
- Assessment/history taking
- Identifying trauma(s) to work on)
- Resource building/skill development (e.g. for self-soothing and emotional regulation)
- Target memory identified and processed using EMDR therapy procedures. * client engages in ‘sets’ of bilateral stimulation whilst simultaneously holding the trauma in mind: * After repeated sets, when the client reports no distress related to the targeted memory, the client is asked to focus on a preferred positive belief * This process (of processing target memory) is repeated for all traumatic memories identified by as problematic by the client.
\
Narrative Exposure Therapy (NET)
Overview
Summary
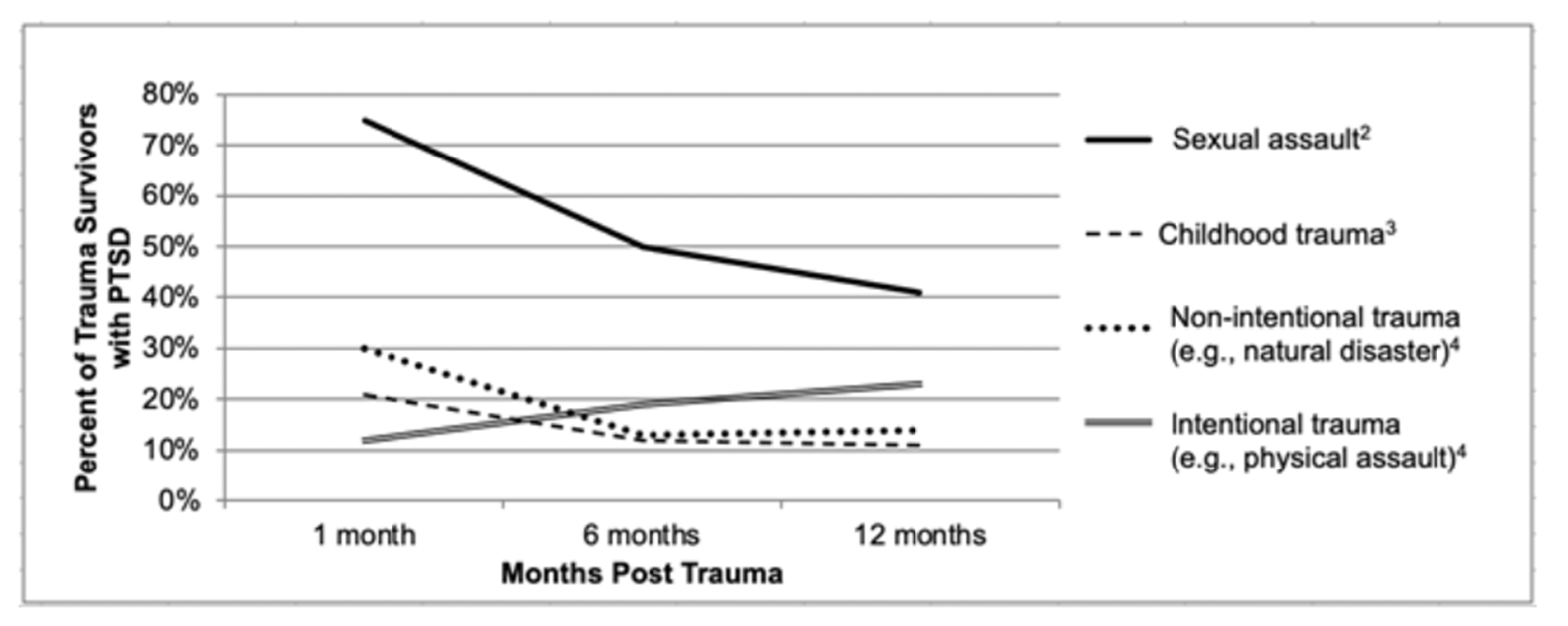
- PTSD is one potential consequence after a person experiences a traumatic event * PTSD-type symptoms are normal in the immediate aftermath of a trauma, only if symptoms persist should a diagnosis of PTSD be made * PTSD is much more likely to develop after certain types of trauma (e.g. interpersonal violence)
- Understanding trauma in its context is important
- Trauma-focused therapies are the main evidence-based treatments for PTSD at present
- Treatments should be adapted to incorporate the cultural and personal beliefs and values of the client
Criterion B: Re-experiencing Symptoms
The traumatic event is persistently re-experienced
- Need 1 or more symptom: * Recurrent, involuntary and intrusive memories of the trauma * Nightmares of the trauma * Flashbacks of the trauma (and other dissociative reactions to the trauma including complete loss of consciousness) * Intense or prolonged distress after exposure to traumatic reminders. * Marked physiologic reactivity after exposure to trauma-related stimuli
- For children: * Intrusive memories: children older than 6 may express this symptom in repetitive play. * Nightmares: Children may have frightening dreams without content related to the trauma(s). * Flashbacks: Children may re-enact the event in play
Criterion C: Avoidance Symptoms
Persistent effortful avoidance of distressing trauma-related stimuli after the event
- Need 1 or more symptom: * Avoid thoughts, feelings, conversations about the trauma * Avoid external reminders (e.g. people, places, activities, objects, situations) associated with trauma
Criterion D: Negative alterations
Negative alterations in cognitions and mood that began or worsened after the traumatic event.
- Need two or more symptoms: * Inability to recall key features of the trauma * Persistent (and distorted) negative beliefs and expectations about oneself or the world (e.g. “I am bad”; “the world is completely dangerous”) * Exaggerated blame of self or others for causing the trauma * Persistent negative trauma-related emotions (e.g. fear, horror, anger, guilt, shame) * Difficulty experiencing positive emotions (constricted affect) * Decreased interest in (pre-traumatic) significant activities * Feeling isolated/cut off/disconnected from others
Criterion E: Alterations in arousal and reactivity
Trauma-related alterations in arousal and reactivity that began or worsened after the traumatic event
- Need two or more symptoms: * Irritability or aggression * Risky or self-destructive behaviour * Hypervigilance * Exaggerated startle reaction * Difficulty concentrating * Difficulty sleeping
Criteria F + G + H
- Criterion F: * Duration of symptoms must be more than one month. (If less than diagnosis of acute stress disorder may be more appropriate)
- Criterion G: * symptom-related impairment in social, educational or occupational functioning
- Criterion H: * Disturbance is not due to medication, substance use, or other illness.
\