Pathology of Pulmonary Neoplasia (Pathology of Lung Cancers)
lung cancer deaths are expected to increase more than 1.8 times over the next 20 years
In the UK lung cancer is very slowly decreasing particularly in the male population
Lung cancer aetiology: Tobacco (main)
-abestos
-environmental radon
-air pollution and urban environment
-other occupational exposure: chromates, hydrocarbons, nickel
-other radiation
pulmonary fibrosis
>85% lung cancer attributable to TOBACCO
females may be more susceptible
per cigarette more susceptible and the way they smoke
RISK related to consumption - inhalation and pack years
NO safe smoking threshold
the more you smoke the greater your risk, risk reduces with abstinence but only slowly
the damage persists in patients lungs for very long (persisting genomic damage)
60 recognised carcinogens in tobacco smoke (different for each companies)
Tobacco smoke effects:
epithelial effects
multi-hit theory of carcinogenesis
-12 genetic alterations in cells to cause a tumour
host activation of pro-carcinogens
→inherited polymorphs predispose
-metabolism of pro-carcinogens
-nicotine addiction
some patients who smoke tobacco can get a lung cancer that is not usually caused by tobacco smoke
-main point is tobacco damages genetically
KRAS, BRAF and MET mutations may act as addictive oncogenic drivers but are associated with smoking
EGFR, HER2 mutations and various fusion genes are addictive drivers and are NOT associated with smoking
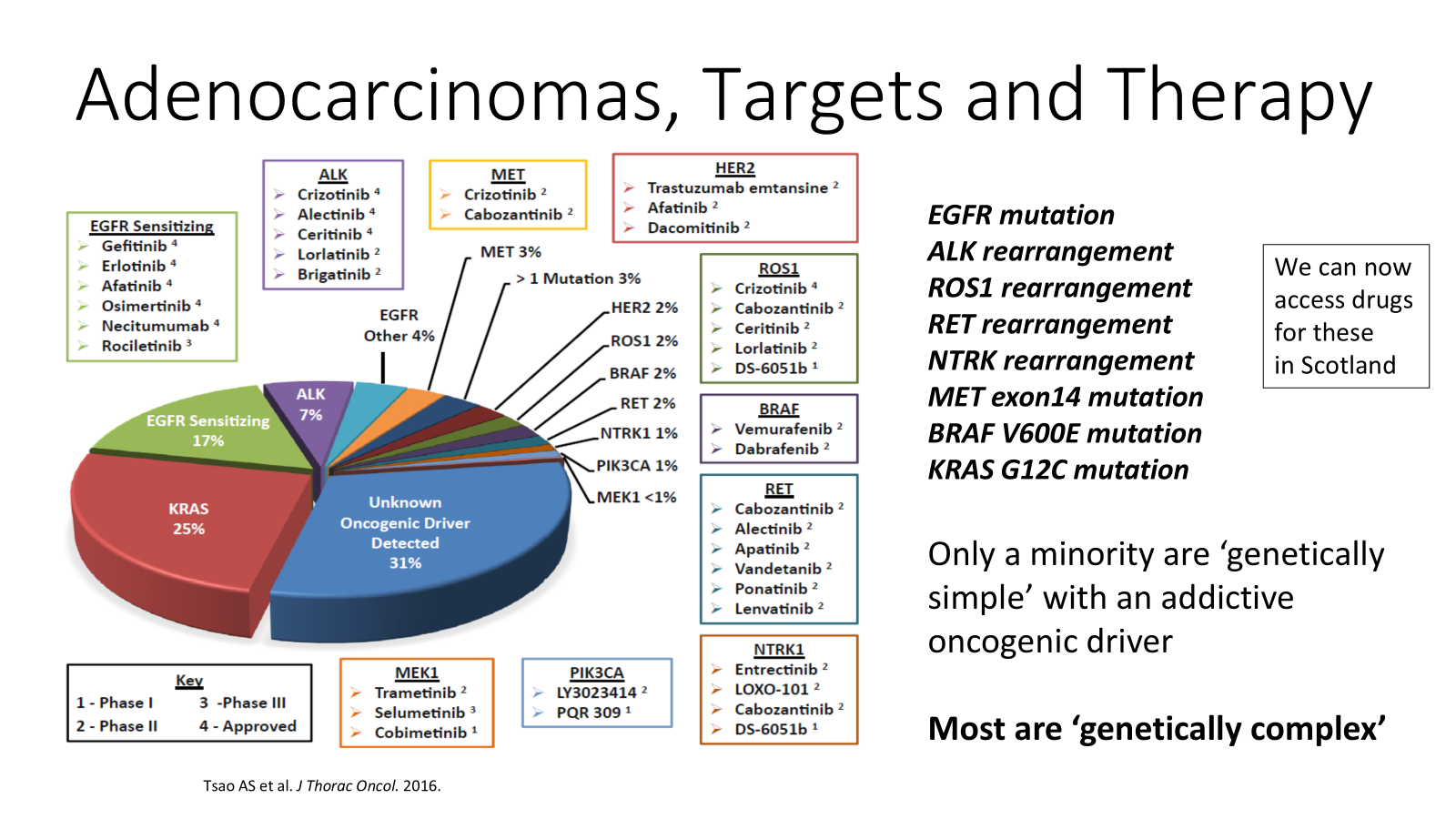
drugs to give patients to target addictive oncodrivers
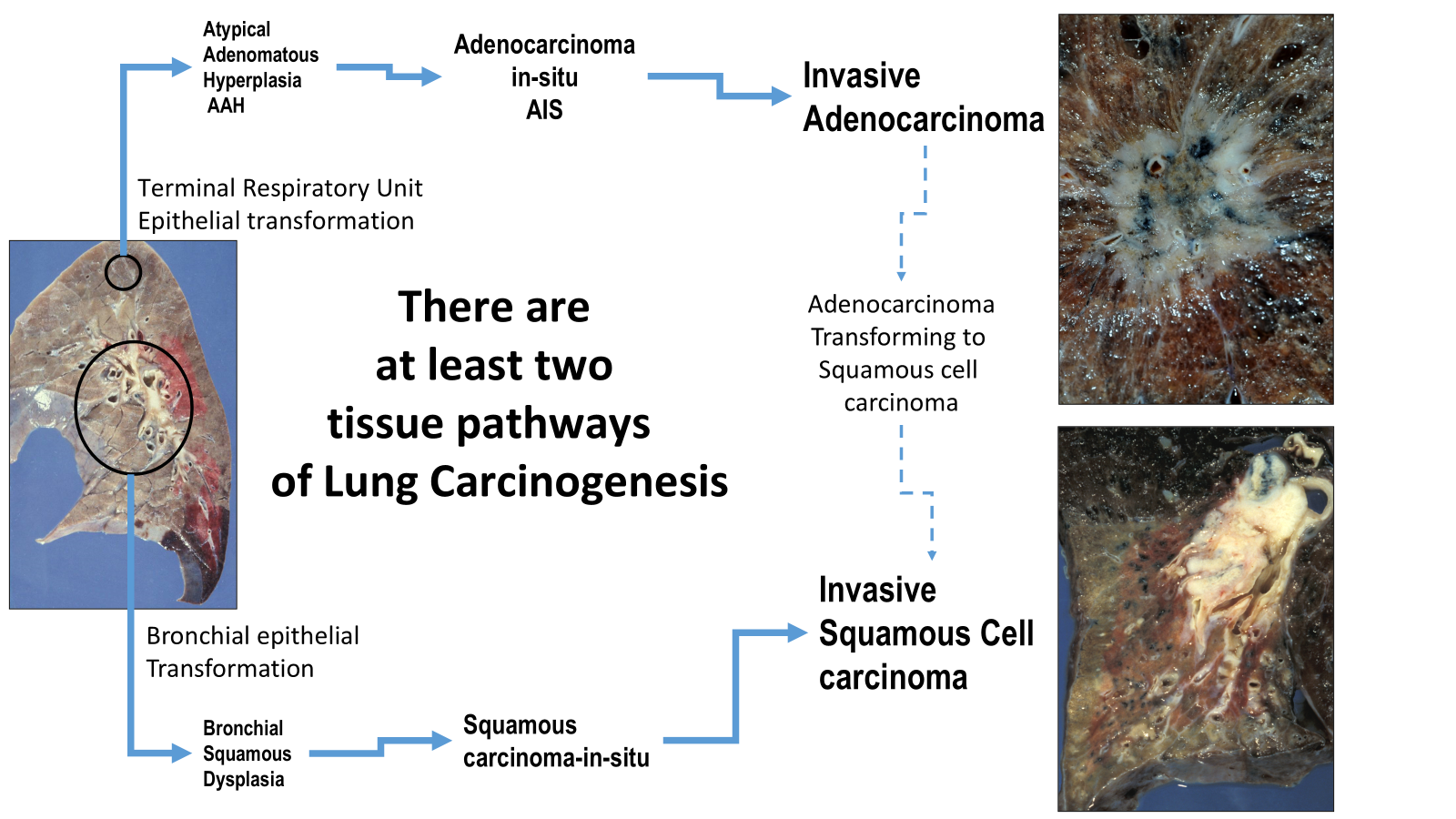
-this is to do with adenocarcinomas of the lung
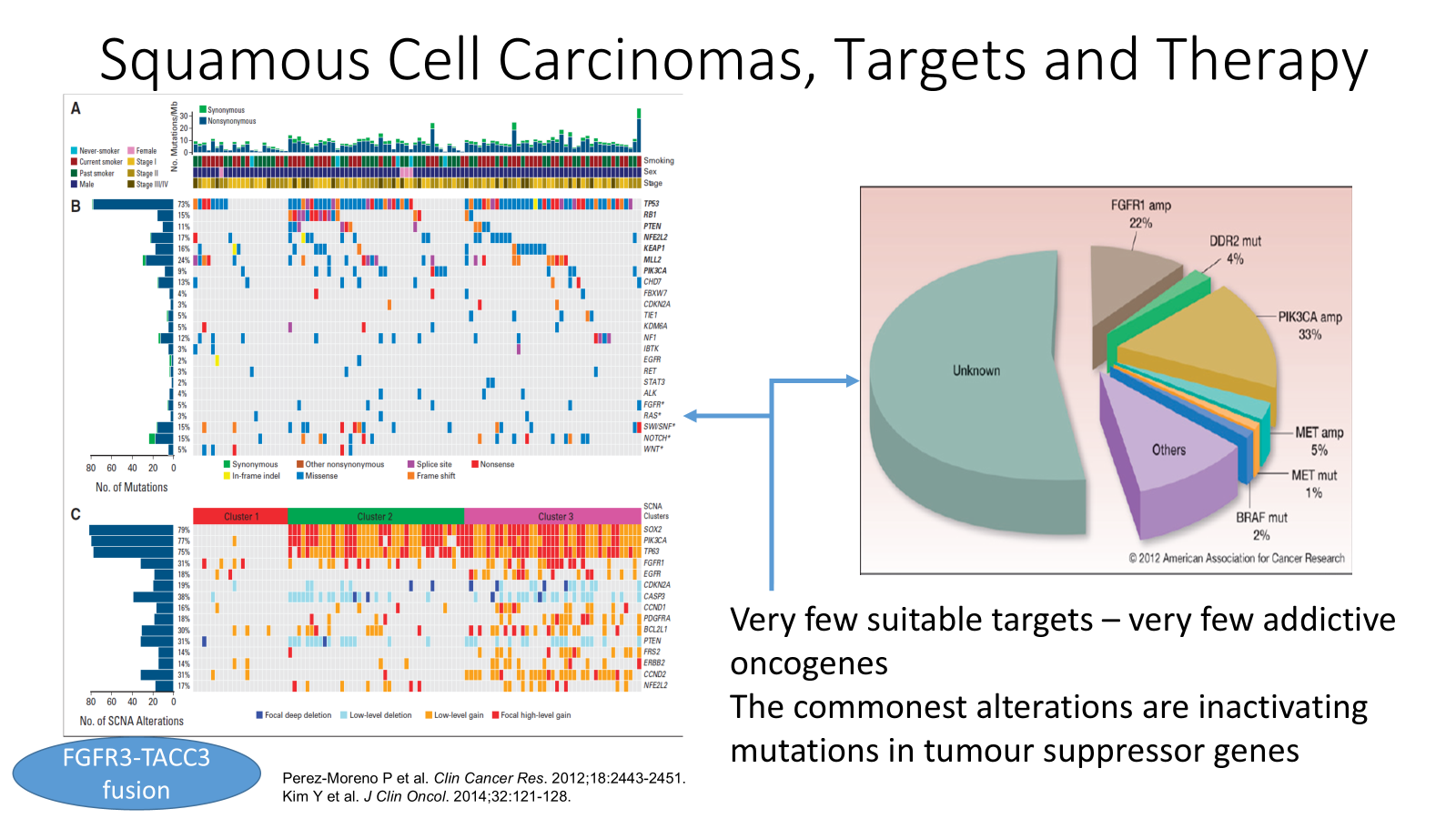
squamous cell carcinomas don’t have good oncodrivers for these because most of these are very genetically variable?
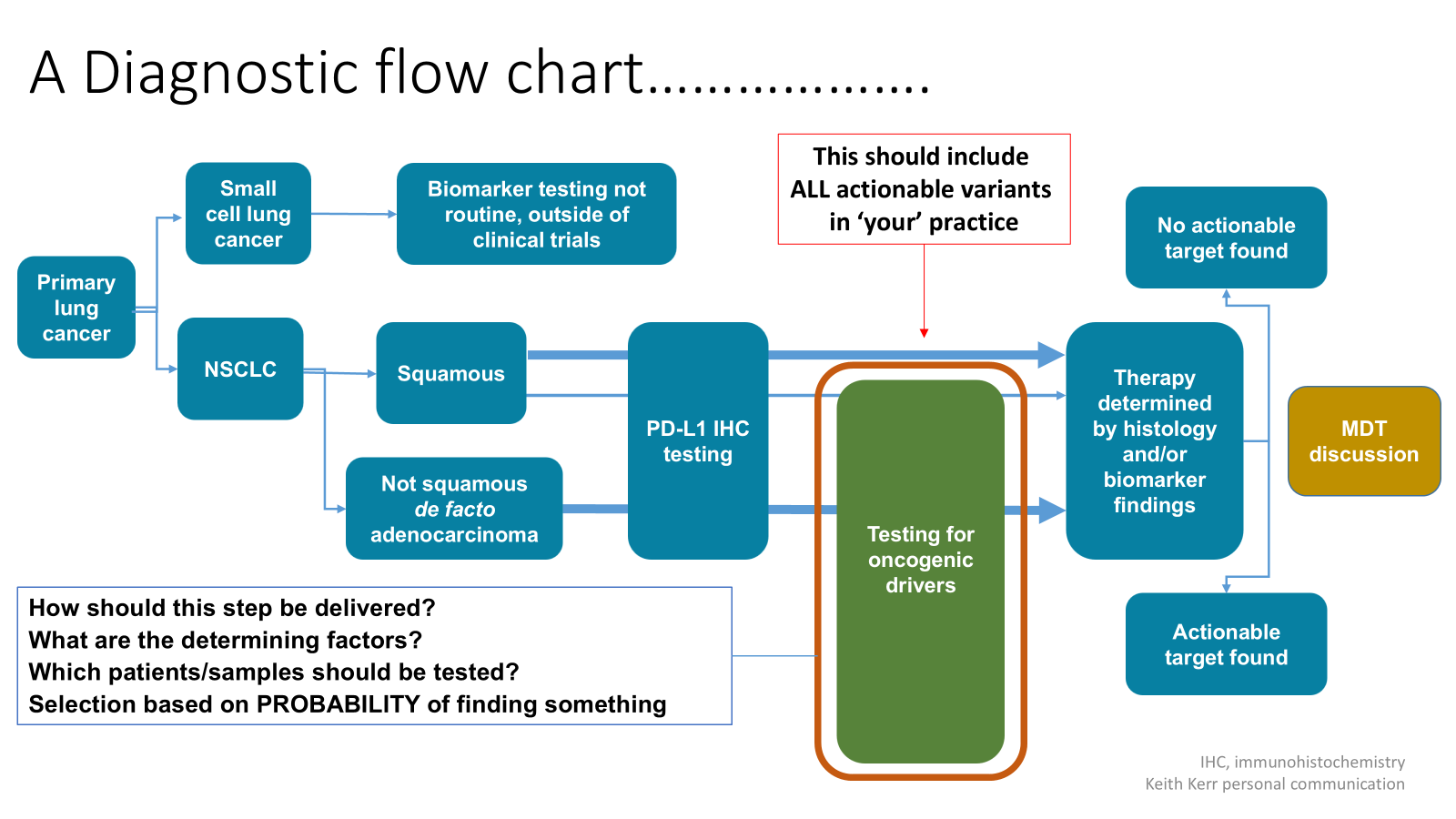
small cell carcinoma gets different chemotherapy to the other carcinomas:
-adenocarcinoma, squamous cell carcinoma, large cell carcinoma and others
You can get other tumours of the lung (metastatic disease of the lung)
Primary lung cancer
grows slowly and silently before found
presents LATE in its natural history
symptomatic lung cancer is fatal
if tumour cough fast enough can be chopped out and a larger one too if not spread to anywhere else
coughing up blood always needs to be investigated
left eyelid drooped, patient won’t sweat on left side of face etc
i.e horner’s syndrome- has lung cancer
super vena cava obstruction, risk of cerebral oedema
Lymph node metastases: -intrapulmonary nodes (N1), extrapulmonary intrathoracic nodes (N2, N3) and
Extrathoracic nodes (M1)
non metastatic paraneoplastic effects of lung cancers
skeletal: -clubbing, hypertrophic pulmonary osteoarthropathy (HPOA)
pain in wrists and ankles because of distal periosteal inflammation
endocrine: –ACTH, SIADH, (small cell) PTH (squamous)
small cell carcinoma much more aggressive disease compared to adenocarcinoma
prognosis factors in lung cancer: -stage of disease
-classification i.e type of disease
-markers/oncogenes/gene expression profiles
T= size of tumour
N= status of lymph nodes in various places
M= presence or absence of metastases
finding and using biomarker-selected therapy options in lung cancer allows them to live longer
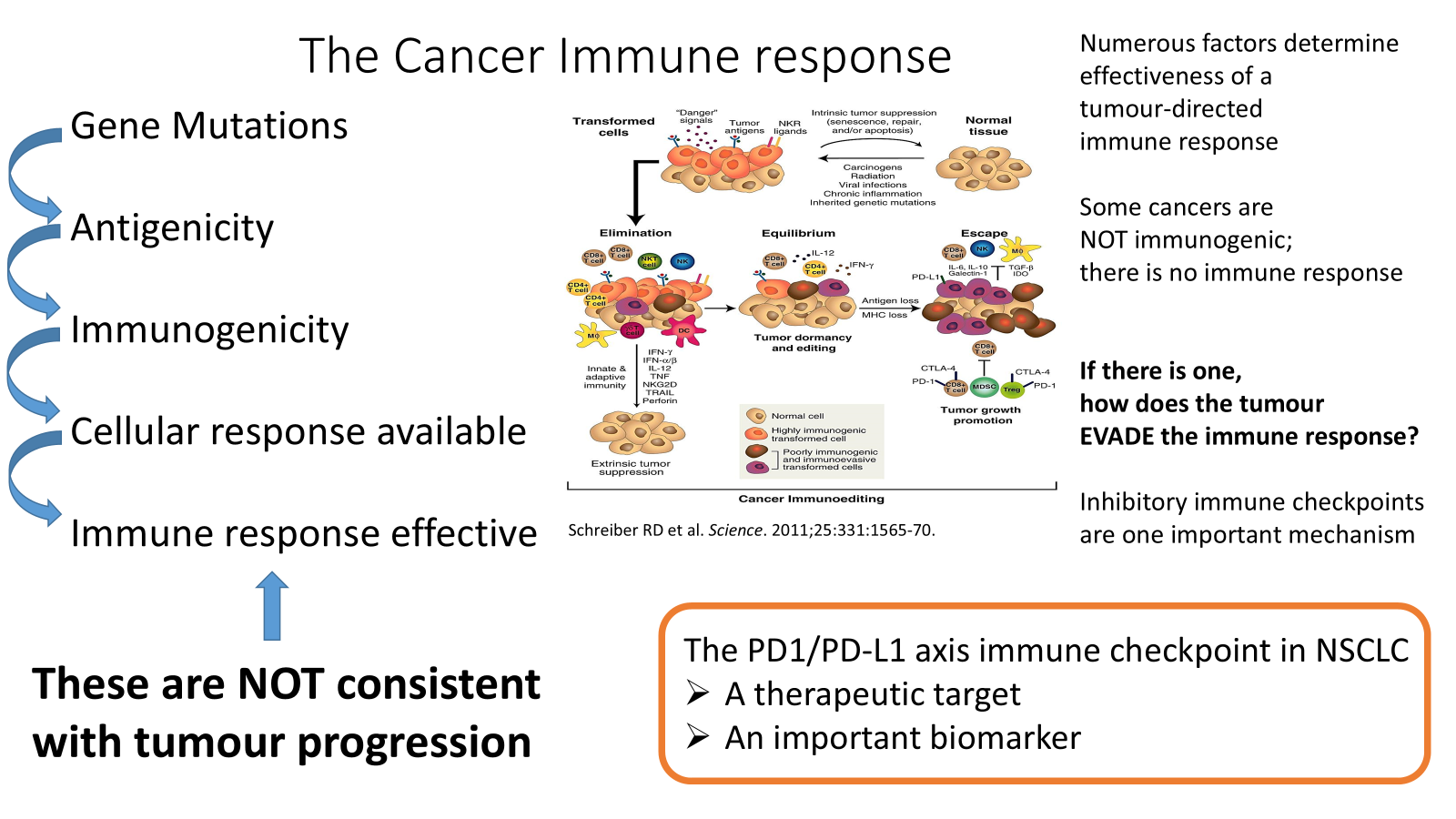
switch off mechanisms get hijacked by tumours to evade the immune system
antibody drug conjugates-effective way of delivering chemotherapy
depends if specific protein expressed on surface of cell