Wk9: Child Psychopathology
Introduction
Learning Objectives
Develop understanding of challenges in identifying psychopathology in youth, considering developmental context.
Learn about the epidemiology of mental health problems across childhood.
Understand aspects of classification of childhood disorders.
Discuss etiology for common childhood difficulties not covered in other lectures.
Explore the developmental psychopathology framework for understanding developmental challenges in young people.
Scenario: A Sensitive, Loner Daughter
A mother is concerned about her daughter who has strange ideas.
The daughter believes she can cause car wrecks by raising her hand.
She gets angry when the weather doesn't stop raining.
She fears a "crab creature" will grab her leg if it hangs off the bed.
Question: Might this young person have a mental health disorder?
What information is needed to assess the situation?
The Importance of Age:
Age is a critical factor in determining developmental appropriateness.
Such behaviors might be developmentally appropriate at age four or five due to developing imagination.
Concerns would increase if the behavior persists into upper primary school (10-12 years).
In a teen, such behavior could indicate psychosis or delusional thinking.
Considering Context
Behaviors like crying when separated from a caregiver, having tantrums, not being able to read, swearing, or wetting the bed have developmental contexts.
These behaviors might be typical at certain ages but abnormal at others.
Case Study: Jack, a Six-Year-Old
Jack's parents disagree on whether he needs a psychologist.
Jack is not sleeping in his own bed, refuses birthday parties without parents, and has tantrums when going to school.
One parent thinks Jack is just shy and will outgrow it; the other is concerned.
Questions to Consider:
Why are these behaviors occurring from Jack's point of view?
Consider bullying at school as a possible factor.
Explore conflicting parental views and parenting styles.
Assess Jack's temperament and its impact on his relationships.
Understand Jack's physiological state and markers related to his experiences.
Determine the timeframe of the behaviors and any coinciding events (e.g., school start, family issues).
Consider the historical context, such as the impact of COVID.
Evaluate the frequency and context of tantrums (only at school or more widespread?).
Assess Jack's learning abilities and potential intellectual disabilities.
Investigate separation anxiety related to school context.
Consider Jack's developmental age and milestones to assess potential delays.
Determining "Abnormality"
Consider the frequency and intensity of cognitions, physiological signs, behaviours, and emotions.
Assess deviation from norms for a child's age.
Evaluate behavior appropriateness in developmental, family, and cultural contexts.
Consider historical factors like COVID.
Assess the impact on the child's functioning.
Epidemiological Considerations
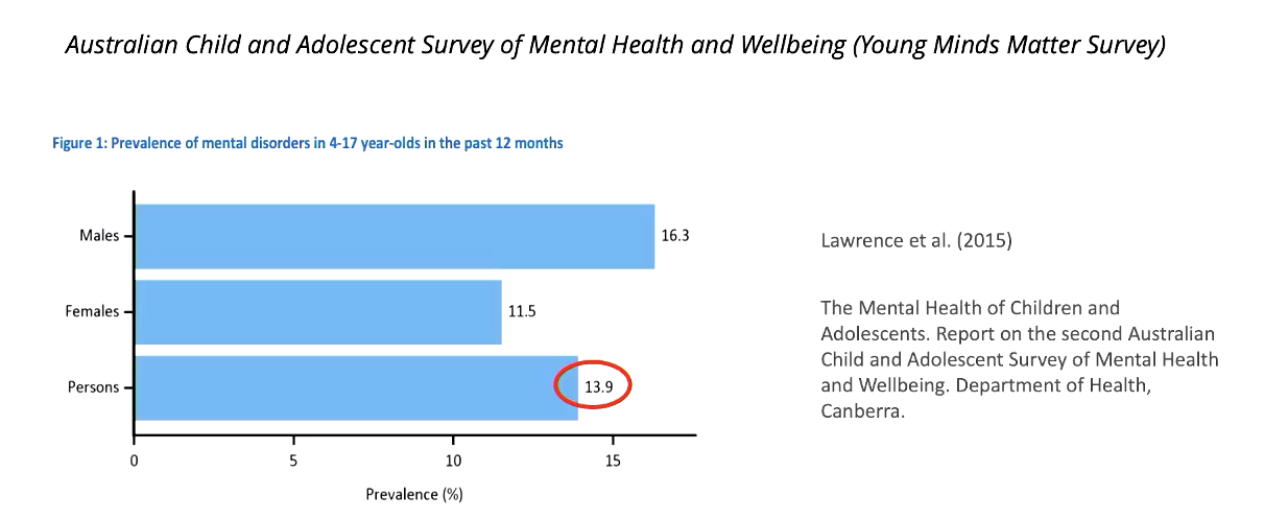
Mental health difficulties are common in youth.
The 2015 Young Minds Matter survey indicated that 14% of surveyed individuals experienced a mental health disorder in the past 12 months.
Lifetime prevalence suggests that around 20% of individuals will experience a psychological disorder during childhood.
Peak time for mental health difficulties: 40% of those aged 16-24 had mental health disorder symptoms in the past 12 months.
Many more young people have distress and impairment even without meeting diagnostic criteria.
Types of Difficulties Seen
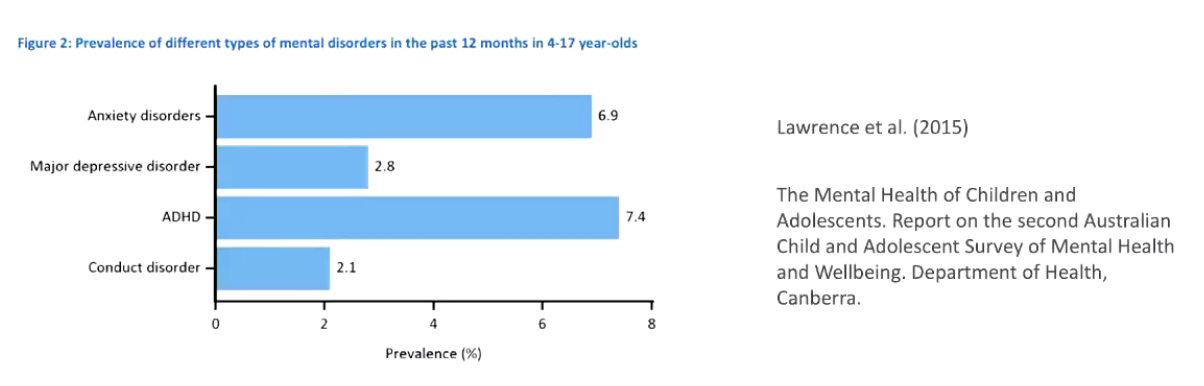
Anxiety disorders and ADHD are particularly prevalent.
Higher prevalence in specific groups, such as First Nations youth and LGBTQ+ individuals, rural groups.
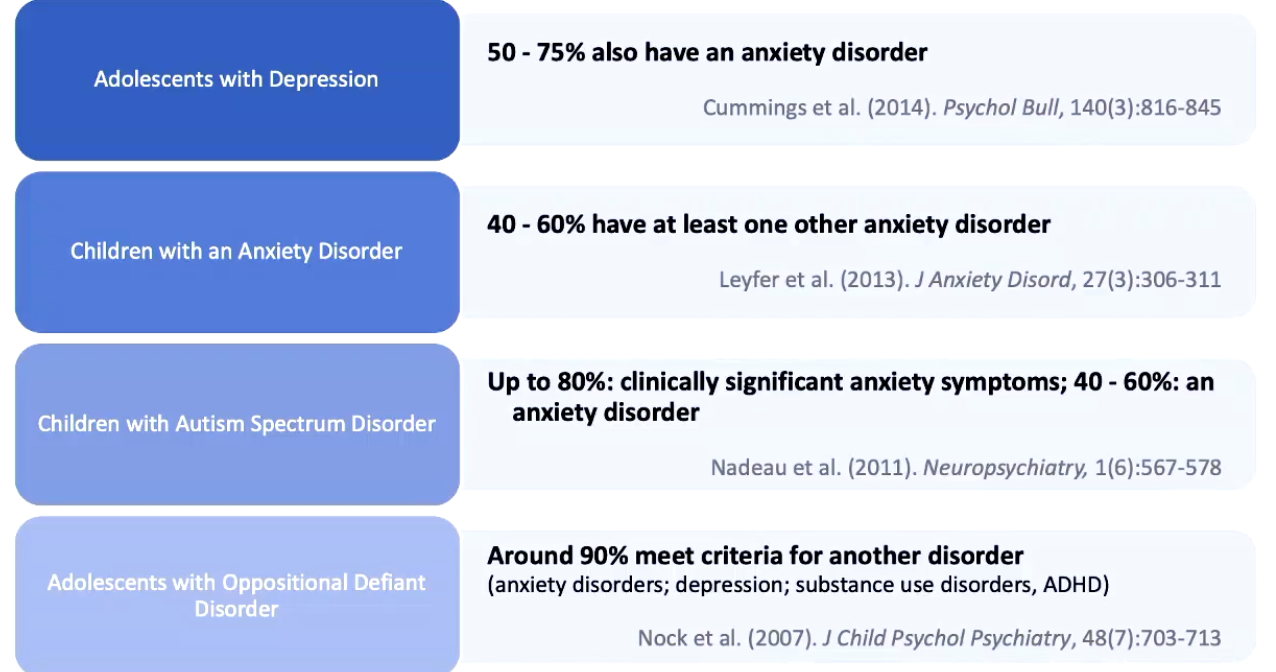
Comorbidity
Comorbidity is common, with about 40% of children diagnosed with one mental health disorder having another.
Examples include adolescents with depression also having anxiety disorders.
Children with ASD often have clinically significant anxiety symptoms.
Adolescents with oppositional defiant disorder frequently meet criteria for other disorders like anxiety, depression, substance use, and ADHD.
Reasons for High Comorbidity
Shared underlying etiology such as underlying brain differences.
Challenges in drawing categorical boundaries around disorders.
Overlapping symptoms.
Challenges associated with one disorder becoming risk factors for another (e.g., social anxiety leading to social withdrawal and depression).
Prevalence Trends
Overall, prevalence is greater in adolescents than younger children, except for ADHD and oppositional defiant disorder, which are more prevalent in younger children.
Depression, anxiety, and eating disorders are more prevalent in girls.
ODD, ADHD, ASD, and SLD occur more frequently in boys.
Interactions Between Sex and Age
Pre-adolescent boys and girls are equally likely to present with depression; in adolescent samples, depression, anxiety PTSD and eating disorders is more prevalent in girls.
Hypothesized Mechanisms for These Differences
Psychosocial stressors.
Pubertal changes.
Hormonal mechanisms.
Increase in Prevalence Over Time
Depression in adolescents has increased over a ten-year window.
Anxiety disorders have increased by 51% between 2004 and 2017.
There has been a marked increase in autism prevalence.
Explanations for Increasing Prevalence
Increase in awareness and understanding, facilitated by social media.
Decrease in stigma.
Changes in diagnostic criteria.
Increased prevalence of risk factors.
Access to Services
Despite high prevalence, relatively few young people access services.
Around half of young people in a population survey accessed mental health services for their difficulties in the past twelve months.
Reasons for Lack of Access
Stigma.
Availability and accessibility of services.
Dependence on parental awareness and willingness to access services.
Risk of under-identifying difficulties due to throwaway lines.
Importance of Understanding Child and Adolescent Mental Health Disorders
Associated with distress and impairment for young people.
Most adults with mental health disorders had their first onset in childhood.
About half of adults with mental health disorders had difficulties before age 14; 75% by age 24.
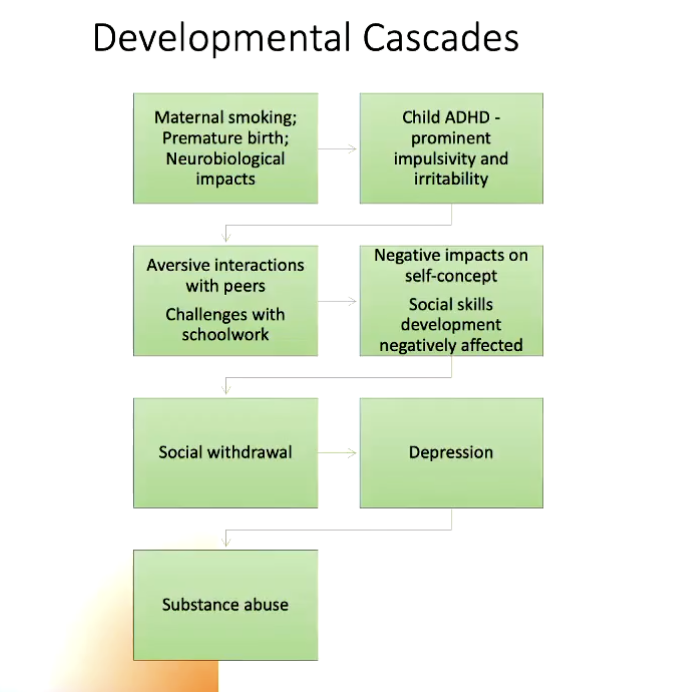
Mental health difficulties in childhood can have cascading effects on development.
Key Documents for Further Reference
Black Dog Institute resources.
National Children's Mental Health and Well-being Strategy.
Categorical Approaches to Classification in Childhood
Various classification systems exist.
DC-0-5: diagnostic classification system specifically for infants and toddlers.
DSM-five: commonly used in Australia, can be used for children under five.
ICD-11: similar to DSM, but with some specific differences.
Developmental Sensitivity of DSM-Five
Not particularly developmentally sensitive.
Criteria for diagnosing mental health challenges in youth are similar to those for adults.
Some disorders have developmental specifiers (e.g., mood presenting as irritable instead of low for depression).
PTSD is an exception where the DSM is more developmentally sensitive.
Some disorders are noted as most likely to manifest during childhood, such as neurodevelopmental disorders.
Neurodevelopmental Disorders
Group of disorders with onset in childhood, though not always diagnosed early.
Deficits in motor skills, communication skills, social cognitive abilities, impacting functioning across different domains.
High degree of heritability.
More common in boys.
Typically multifactorial, with rare singular causes.
High levels of comorbidity between these disorders.
Categories of Neurodevelopmental Disorders
Intellectual disability.
Autism.
ADHD.
Other neurodevelopmental disorders:
Communication disorders.
Motor disorders.
Specific learning disorder.
Diagnostic Criteria: Intellectual Disability
Deficits in intellectual functions (reasoning, problem-solving, planning).
Deficits in adaptive functioning, leading to failure to meet developmental and sociocultural standards.
Difficulties evident in the developmental period.
Various specifiers related to severity.
Prevalence and Etiology of Intellectual Disability
Prevalence: 1% to 3% of the population.
More common in males.
Many known causes, but also many unknown causes.
More etiology known for severe and profound cases.
About 30% to 40% of people with autism have comorbid intellectual disability.
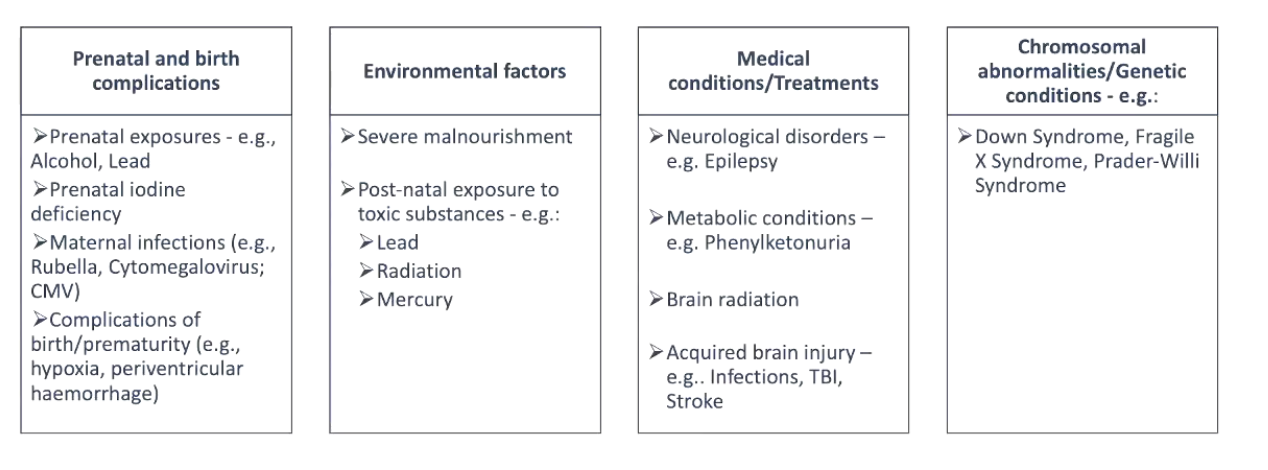
Risk Factors Associated with Intellectual Disability
Prenatal factors (genetic syndromes, chromosomal abnormalities).
Birth or prenatal complications.
Medical conditions.
Diagnostic Criteria: Autism
Persistent deficits in social communication and social interaction.
Social communication involving pragmatic language. “How easy is it to adjust language depending on person, small talk etc.”
Non verbal and verbal aspects of communication - gesture and facial expression.
Restricted, repetitive patterns of behavior, interests, or activities.
Stereotyped or cliched examples around eye contact.
Symptoms present in the early developmental period, but may not become fully manifest until demands exceed capacities.
Prevalence of Autism
Increasing prevalence.
More prevalent in males than in females.
Ongoing discussion around recognition of autism in women and girls.
Consideration in Women and Girls
Why there are differences in presentation of symptoms, and why they are often diagnosed later in life.
Restrictive and repetitive behaviors being more socially appropriate.
The phenomenon of masking.
Comorbidities of anxiety in girls.
Diagnostic Trajectory
Can the signs be spotted in preschool and toddlerhood?
Joint attention.
Early language.
Repetitive behaviors.
Important Note: Concerns around therapies promoting children mimicking neurotypical rather than being themselves.
Spectrum Considerations of ASD
Why do we conceptualize autism as a spectrum versus anxiety or depression?
There is heterogeneity of presentations, because when it was originally conceptualized, there was a recognition.
Additional Questions about Functional classifications
High functioning and low functioning is a really good question and it's a hard one to answer,
Neurodevelopmental disorders have medical condition that is, like, related to their brain and neuroscience,. So, how would you, like, differentiate the two?, And, like, is it, like, if one got some kind of brain injuries or brain disorder, can they still be considered as having neurodevelopmental disorder?.
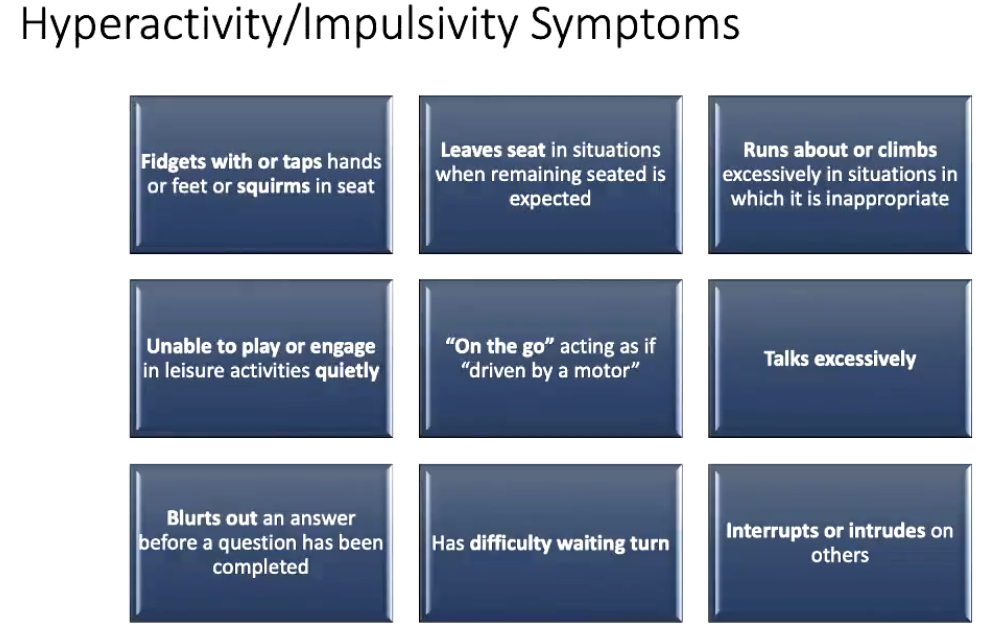
Diagnostic Criteria: ADHD
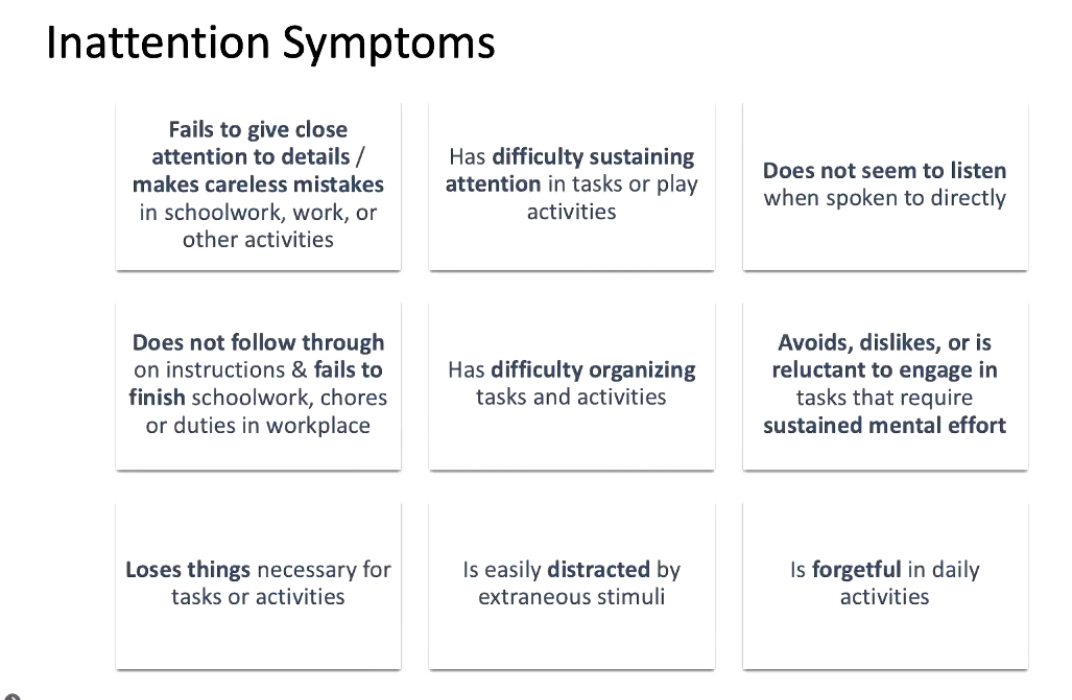
Persistent pattern of inattention and or hyperactivity impulsivity that interferes with functioning or development.
Various symptoms for inattention and hyperactivity impulsivity; at least six symptoms required in either category (five for 17 year olds and up).
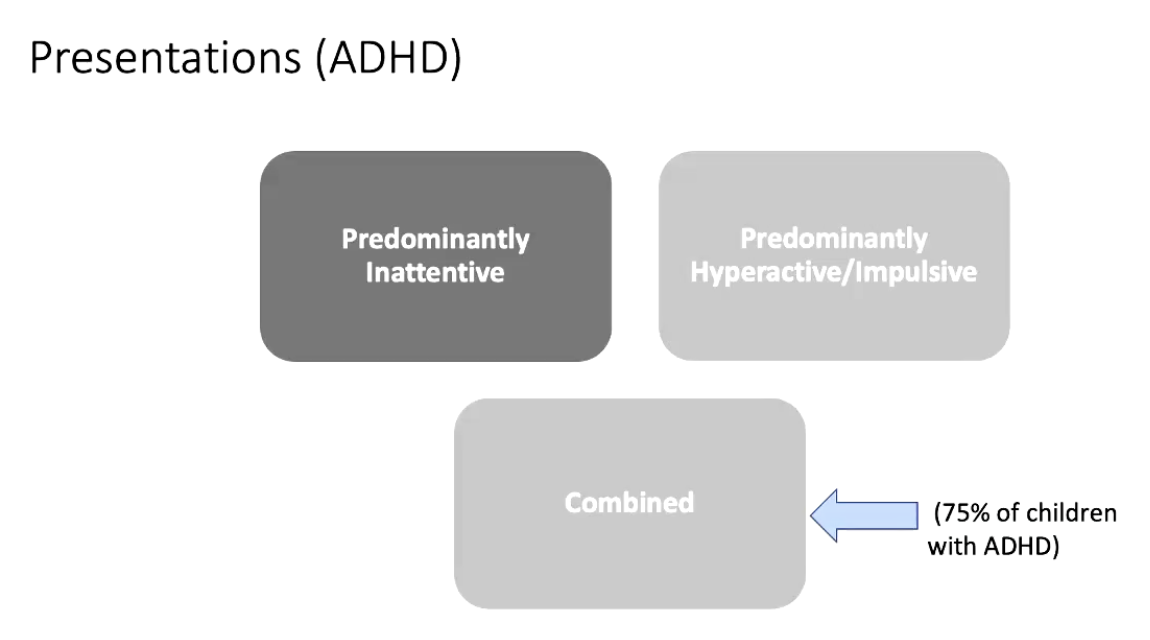
Diagnoses can be made as predominantly inattentive, predominantly hyperactive impulsive, or combined type ADHD.
Prevalence of ADHD
Prevalence: 5% to 7% in childhood.
More common in boys for combined and hyperactive subtypes.
Boys and girls are equally likely to have inattentive type ADHD.
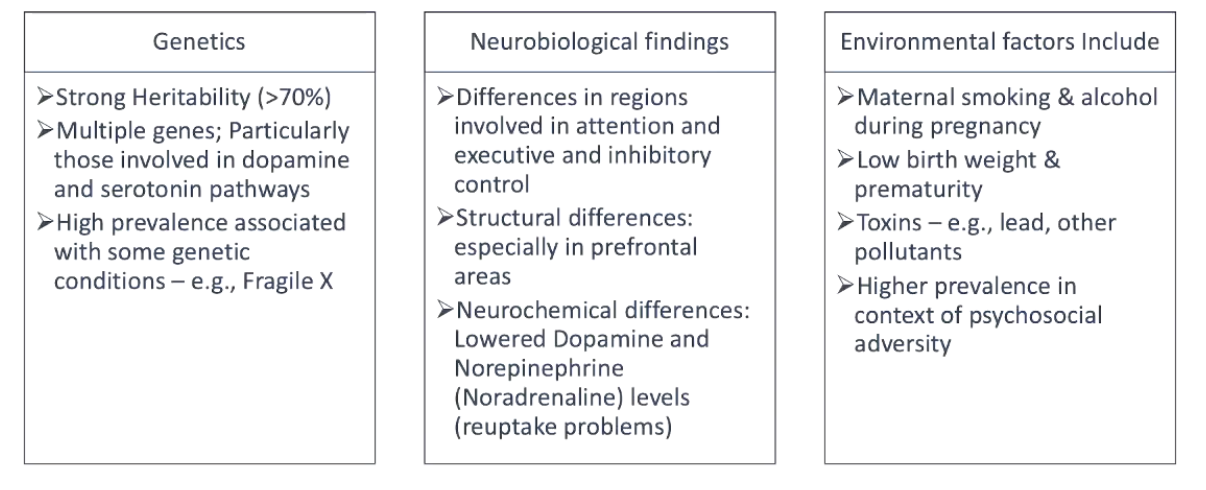
Risk Factors for ADHD
Genetic and neurobiological findings.
Environmental factors related to the in utero environment.
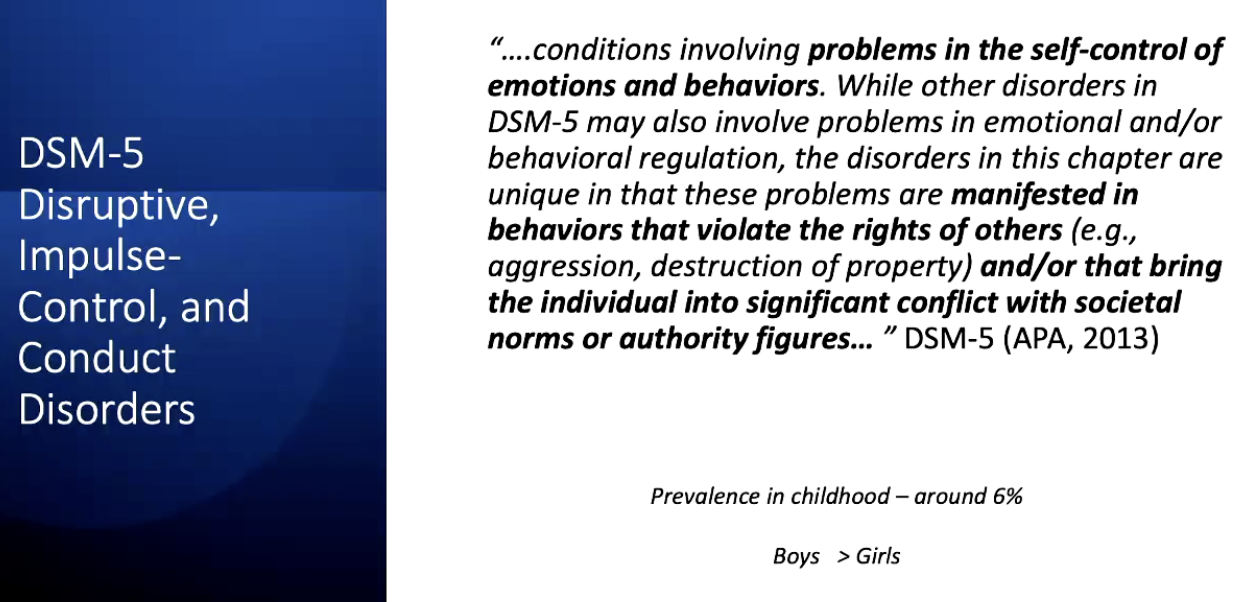
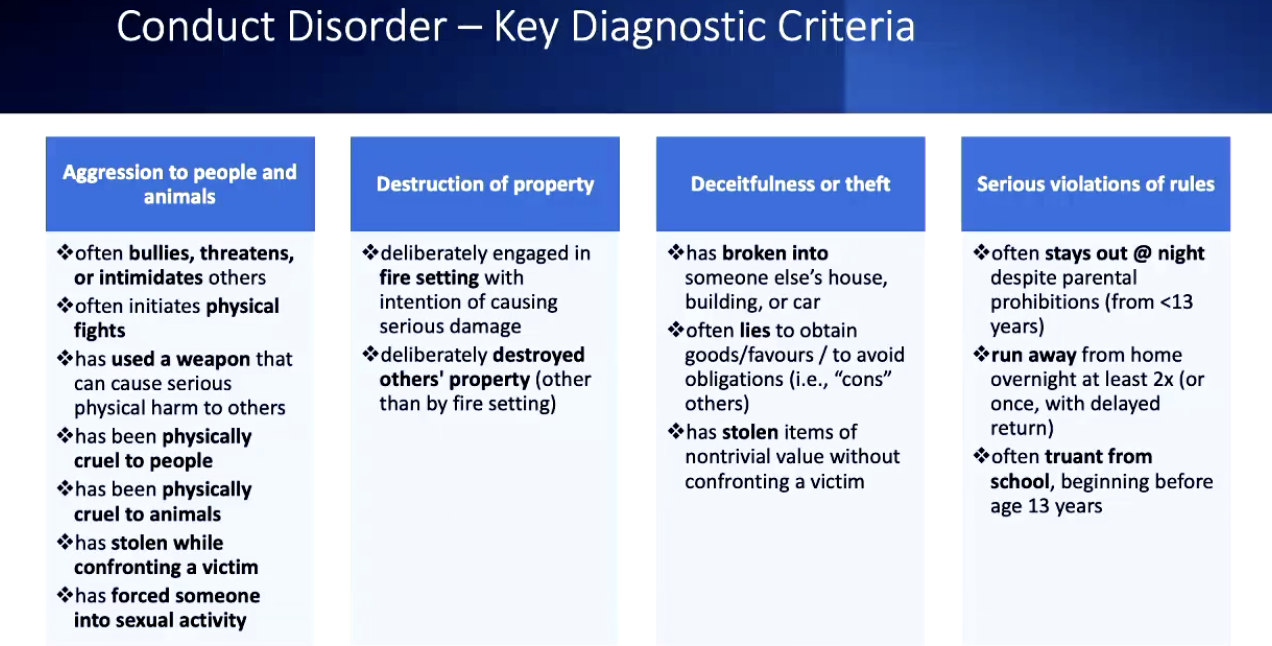
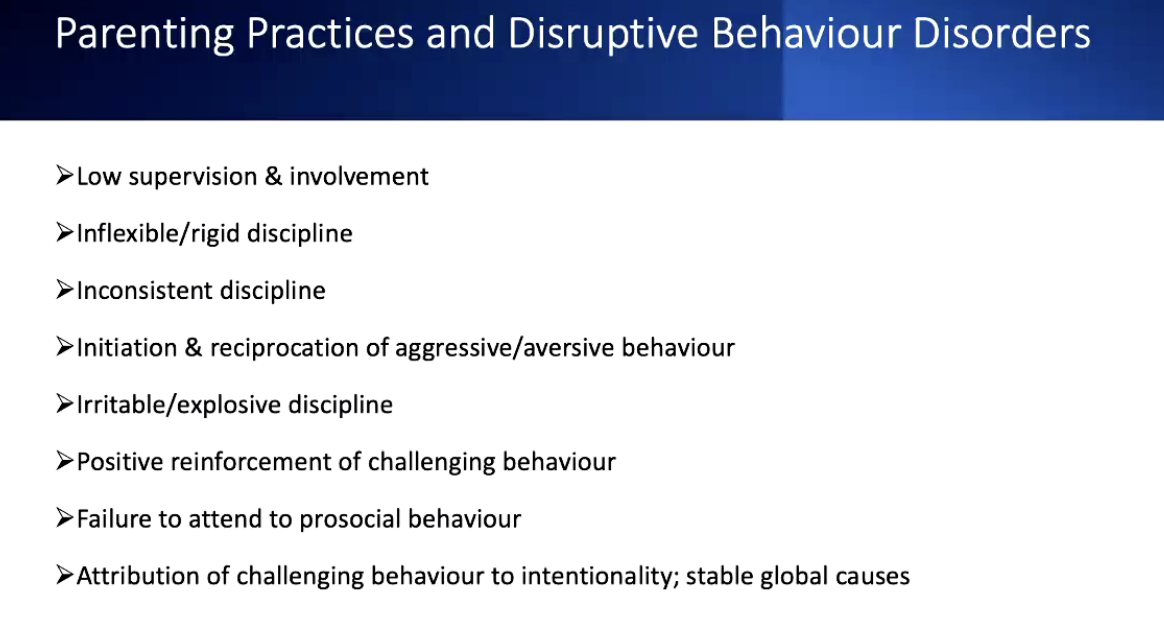
Disruptive, Impulse- Control and Conduct Disorders
Developmental Continuities and Discontinuities:
We may see:
-Developmentally transient problems
-Homotypic continuity (contiuation of the same disorder/symptom of the same disorder/symptom profile from childhood to adulthood)
-Heterotypic continuity (manifestation of psychopathology changes across development)
Developmental factors can impact on clarity on re diagnosis:
-younger children can struggle to reflect/describe internal experiences
-looking for behaivoural indicators, relying on other’s reports
-parent-child concordance poor (especially for internalisinh)
-establishing distress and impairment
-high levels of comorbity
-wide range of what is typical for any age
-heterogeneity of presentations within and across developmetnal stages
THE DEVELOPMENTAL PSYCHOPATHOLOGY FRAMEWORK:
A broad intergrative, cross-disorder approach to studying the developmental processes and pathways that lead to adaptive and maladpative bhehaivour across lifespan.
Key principles:
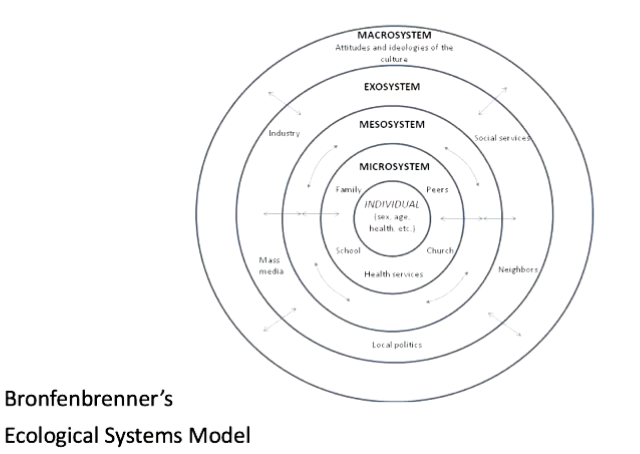
-Systems principles
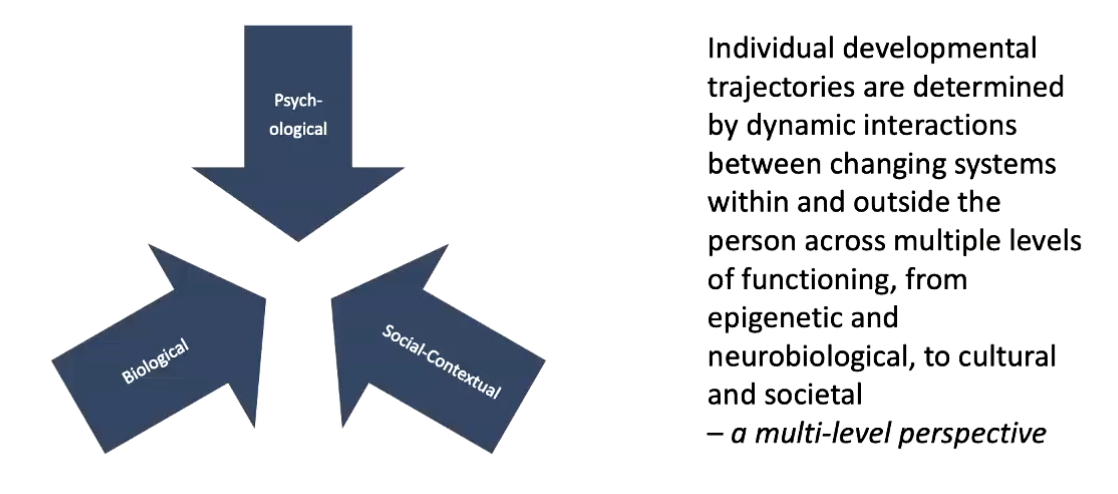
-Multiple- Levels principles
-Normative principles
-Developmental pathways
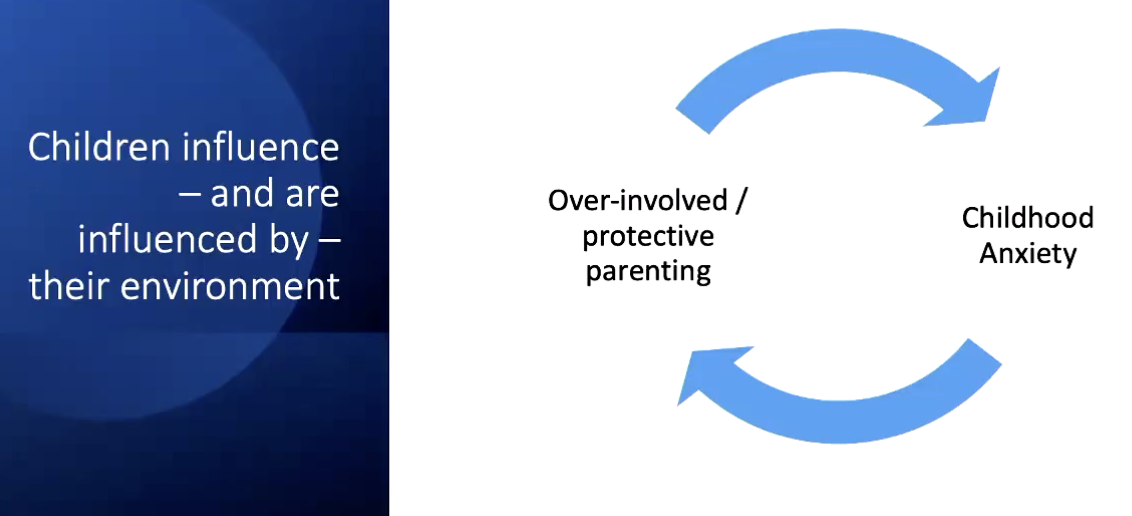
Systems principle: Children are embeded within systemic contexts
Multiple Levels Principles
Normative principle
Understanding psychopathology in a developing person requires an understanding of normative development.
Developmental Tasks
Prenatal period → Infancy/Toddlerhood
Physical growth
Brain development
Establishing an attachment to one or more specific caregivers
Differentation of self from environment
Acquiring functional language
Learning to walk
Preschool → Middleschool
Seperation from caregivers
Regulating emotions and behaivours
Acquiring academic skills
Developing peer relationships
Rule-goverened behaivour
Adolescence
Establishing autonomy from parents
Consolidating close peer relationships
Preperaing for job/career/further education
Exploring & developing various aspects of idenitty
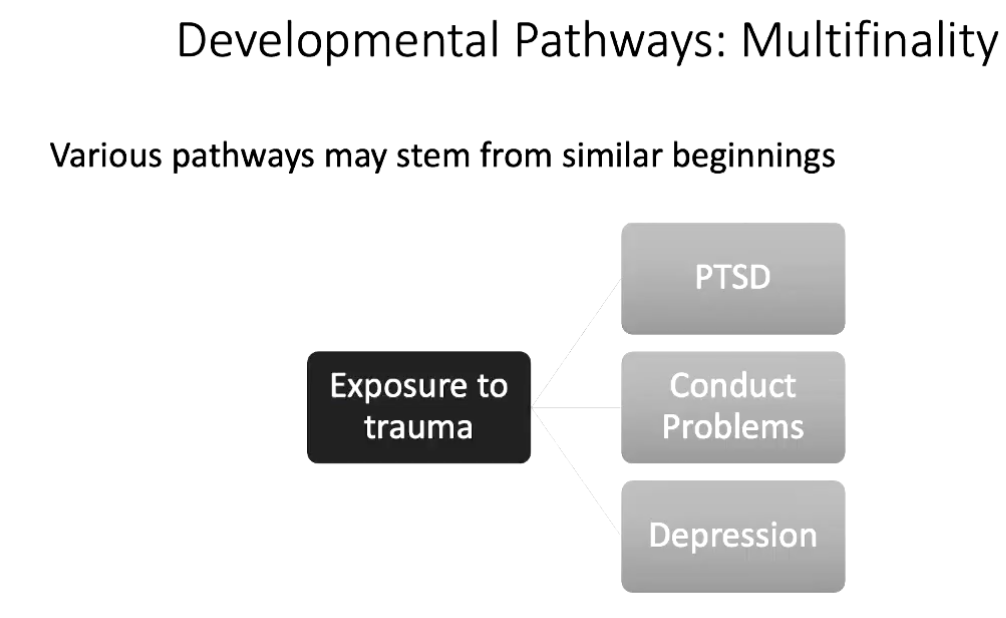
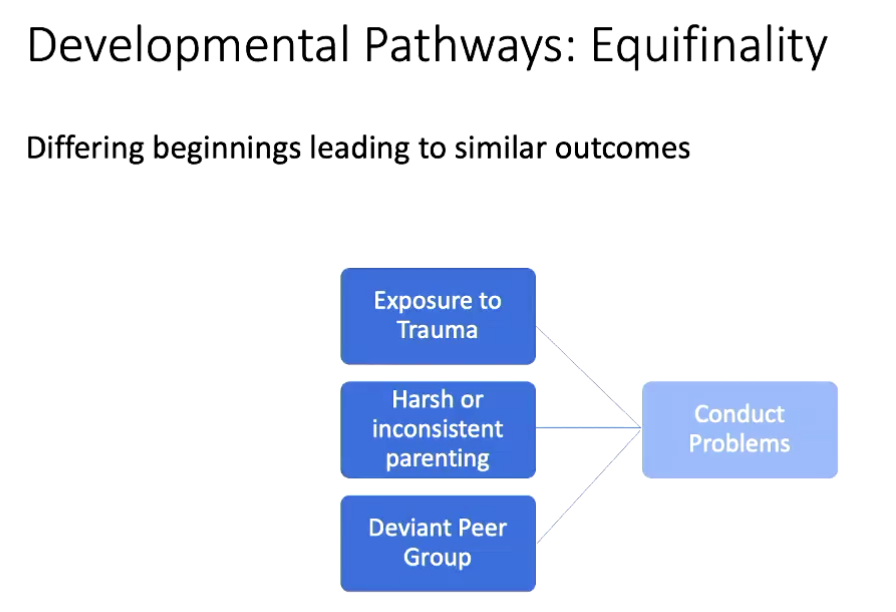
Developmental pathways:
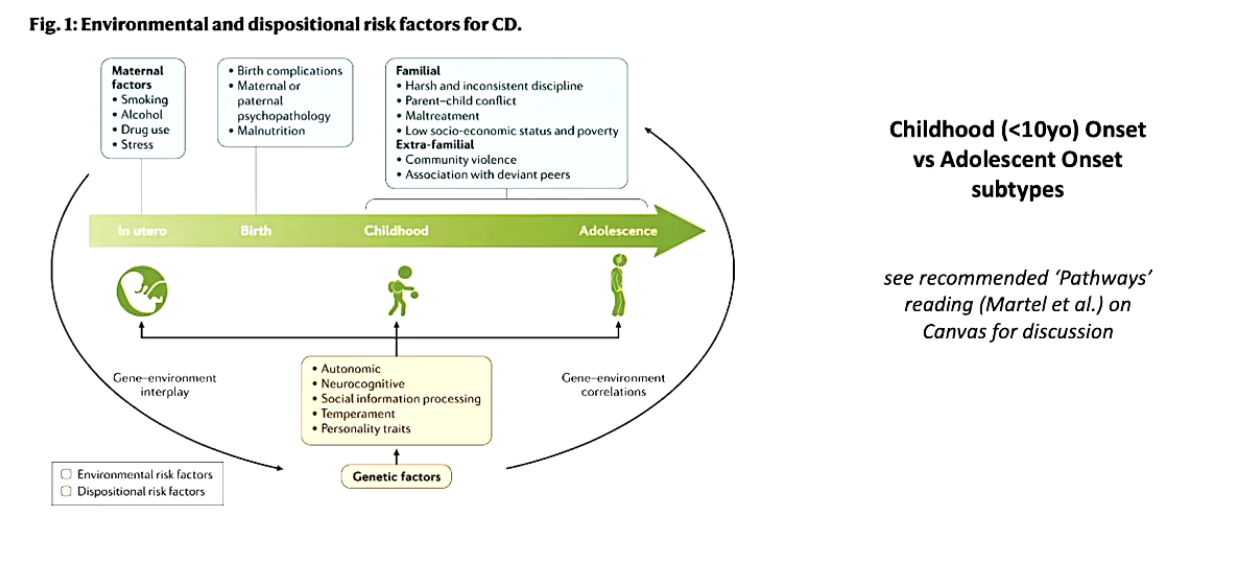
Multiple factors (individual and systemic) interact dynamically and bi-directionally to influence the course of an individual’s development.
There are individual risk factors, vulnerabilities and protective factors for each child.
Genetic, biological and systemic factors interact to influence - but not to determine - outcomes: Probabilisitc Epigenesis
PROTECTIVE FACTORS
RESILIENCE
RESILIENC = successful adaptation despite exposure to considerable risk
-it is not a static trait, can vary across context and time