Suppositories and Inserts- Dr. Miroshynk
Based off Dr.Miroshynk’s “Final Exam Study Guide”
Suppositories and inserts: definition and clinical use.
Suppositories
the term used for the solid dosage forms only designed for rectal administration
solid dosage forms in which one or more APIs are dispersed in a suitable base and molded or otherwise formed into a suitable shape for insertion into the rectal area to provide local or systemic effect
Uses: promote defecation, treat anorectal diseases, introduce drug into the body
Inserts- the similar dosage forms that are inserted into a naturally (nonsurgical) occurring body cavity other than the mouth or rectum
Are solid, single-dose dosage forms in which one or more APIs are dispersed in a suitable base and molded or otherwise formed into a suitable shape for insertion into the vagina
Uses: vaginal infections, vaginal disorders
The advantages and disadvantages of rectal/vaginal drug delivery versus oral drug delivery.
Disadvantages of rectal
rectal has lower rate and extent of drug absorption compared to oral
poor patient compliance
upward movement of the dosage form can increase 1st pass metabolism
suppositories can leak
insertion can be hard
erratic absorption
Advantages of rectal
Ideal for drugs liable to degradation in the GI
Hepatic 1st-pass elimination of high clearance drugs is partially avoided
Better for drugs that irritate the stomach
Large doses can be administered
Taste/smell masking
Benefits of Vaginal
Local drug delivery
If Oral intake restricted
Preferential delivery to the uterus
Favorable alternative to the parental administration
Avoids hepatic 1st pass effect
Enables self-administration and removal
Limitations of Vaginal Administration
Gender specific
Premature discharge/leakage of the dosage form
Systemic absorption
Physiological and physicochemical factors affecting the drug absorption from suppositories and vaginal inserts.
Physiological- Rectal
Quantity of fluid available
Property of rectal mucus
Contents of the rectum
Motility of the rectal wall
Lymphatic circulation
Physiological- Vaginal
Epithelium thickness
pH
amount, composition, and viscosity of the vaginal fluids
Physicochemical of APIs- Rectal
Surface properties
Log P
pKa
Particle size
Amount
Physiochemical of APIs- Vagina
MW
Log P
pKa
particle size
surface charge
Physicochemical of the base- Rectal and Vaginal
Composition
Melting behavior
Rheological properties
Suppository/inserts bases: classification and properties.
Properties:
Solid at room temp
Non-irritating
Nontoxic
Physiologically inert
Stable
Compatible w/ other drugs
Viscous enough to prevent fluid leakage
Classification
Fatty
Aqueous
Less frequently used, m.o. above body temp, DOES NOT MELT at body temp, but slowly dissolves in body fluids
Ex: PEG bases
Must be at least 20% water
Issues: hygroscopicity, slow down drug release, oxidation
Ex: Glycerinated Gelatin Base
Translucent, hygroscopic
Not for rectal use- only vaginal
Issues: hygroscopicity, hard to manufacture, potential API issues
Water soluble
Water miscible
Water-dispersible
Polymorphism of cocoa butter.
Can crystallize into many different forms
Various melting points
Exhibits polymorphism due to triglyceride content
Principles of drug incorporation into suppository bases.
base-soluble drugs
menthol
dissolve in molten base
water-soluble
Novacain, ZnSO4
Use concentrated aqueous solutions
Filtrate before mixing with the base
insoluble drugs
zinc oxide, bismuth subgallate, iodoform
spatulate powder with molten base
Typical suppository excipients.
M.p. increasing agents
Beeswax
Magnesium stearate
Colloidal silicon dioxide
M.p. decreasing agents
PEG
Polysorbate 80
Visocity-increasing agents
Silica gel
Tend to decrease release rate
Preservatives
Antioxidants
Surfactants
Absorb many drugs
Only for lipophilic bases/drugs
The methods of suppository preparation.
Fusion molding
Most common
Compression
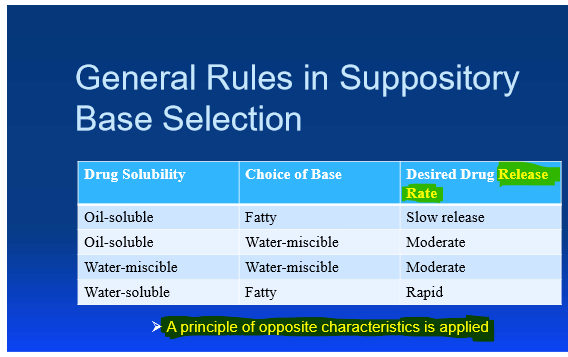
‘The principle of opposite characteristics’ as applied to suppositories and inserts.
We want mismatched drug and base
Ex: oil-soluble drug and water-miscible base
Packaging and storage.
Packaging
Tightly closed glass containers
Compartmented boxes
Individually wrapped
Disposable molds
Storage
Humidity most important/ keep low
Best to keep refrigerated
Quality control of suppositories.
Texture uniformity
Disintegration
Dissolution rate
Content uniformity
Key patient counseling information associated with suppositories and inserts.
Warm to room temp if it was in the fridge
Cocoa butter-based sup should be rubbed gently
Glycerinated gelatin or PEG sups should be moistened w/ water before insertion