Pharmacodynamics
Pharmacodynamics - what the drugs do to the body
drugs have multiple modes of action:
enzyme inhibitors
enzyme false substrates
methyldopa is converted to methyl noradrenaline which is released from nerve terminals to reduce blood pressure
receptor activators (agonists)
bind to receptors and activate them
receptor blockers (antagonists)
ion channel blockers
ion channel modulators
neurotransmitter uptake blockers
change gene expression
Receptors - proteins inserted into the membrane which bind neurotransmitters etc and produce a cellular response
there are different types of receptors:
ligand gated ion channels (ionotropic)
g-protein coupled receptors (metabotropic)
kinase linked receptors
receptors linked to gene expression
agonist - binds to a receptor and activates it
the agonist binds to the receptor and forms an agonist receptor complex which becomes activated and causes a conformational change of the receptor and leads to a response
the response can be measured experimentally:
muscle contraction
add drug to see how much muscle contracts
electrical current change in resting membrane potential (electrophysiology)
production of secondary messenger
inhibition of transmitter release
change in heart rate, blood pressure etc
humans - ecg and animals - telemetry
Example 1
recording a response in guinea pig ileum:
acetylcholine is used as an agonist. This binds to the receptors and causes it to contract. this causes the ileum to contract which pulls on a string. this is measured by a transducer which is put into a computer to have the data acquired. A concentration response curve can be plotted with the log of the concentration of the agonist against the the amount if ilium. This gives a sigmoidal curve
This curve can be modified so it can be done relative to a maximum. To do this, all points are divided by the maximum response value so that the maximum response is normalised to 1.
the potency can be measured by measure the EC50 from the modified graph
EC50 - the effective concentration that gives 50% of the maximum response.
it is a concentration response curve when the concentration and volume inside the vessel is known. When the drug is added, we can know the final concentration inside the vessel. However if the drug is given to a patient, the concentration is unknown so the graph will be plotted using dosage
There is a maximum response:
finite number of receptors which would all be occupied so that the response is directly proportional to the agonist receptor complex concentration
property of tissue
maximum muscle contraction
Stage 1: agonist binds to receptor
affinity - how well a drug binds to the receptor
high affinity - won’t need as much drug to occupy the receptor
stage 2: response
efficacy - a measure of the response once the drug is bound
low efficacy - poor at switching receptor on
Potency is a combination of both affinity and efficacy
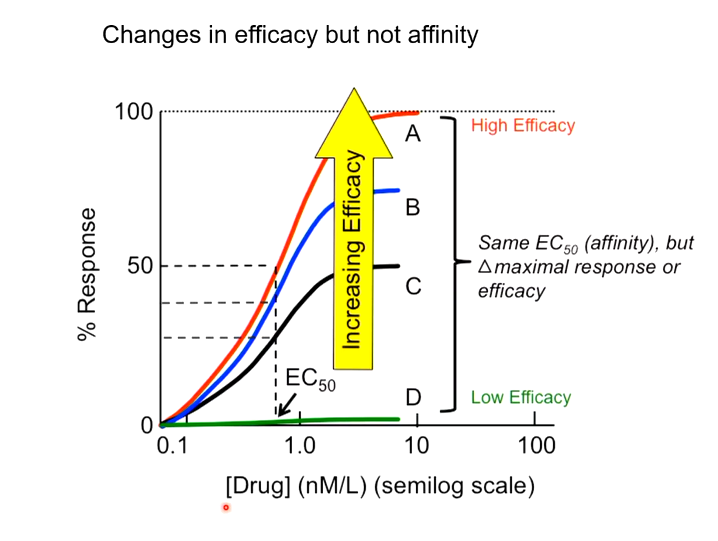
EC50 is the same so all need the same concentration to get to 50% occupied receptors, however A has a higher efficacy so can produce a maximum response but D cannot so has a low efficacy.
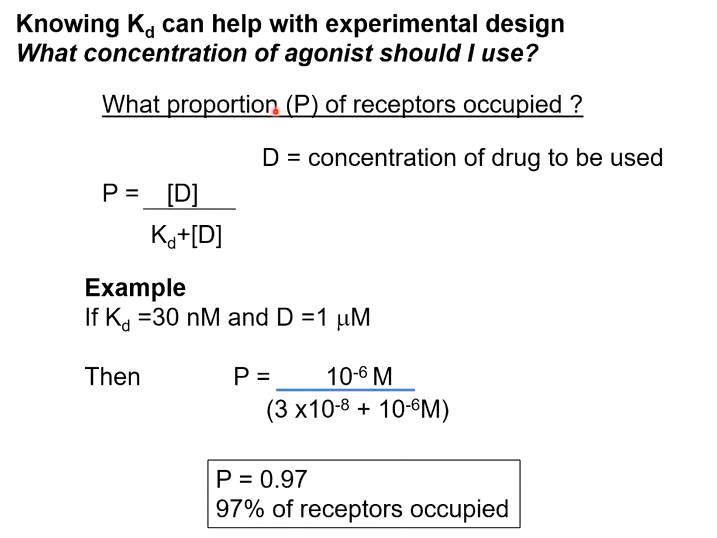
The first part of binding depends on the association and dissociation constants. The ratio between these will determine the affinity of the drug for the receptor. Dissociation divided by association is called the Kd
Kd - the concentration of drug required to occupy 50% of the receptors.
The lower the affinity, the higher the affinity.
If the Kd of the agonist is known, it can help in designing experiments:
If the concentration of agonist to use is unknown, knowing the Kd means you can calculate how many receptors are occupied
Affinity can be measured by using a ligand binding assay. You cannot measure a response as it involves a combination of both affinity and efficacy.
Ligand Binding Assay:
looks at displacement of radioactive ligand (hot ligand)
hot ligand is displaced by a cold ligand
the change in radioactivity is measured over time
plot that and measure the number of receptors and the Kd
the concentration of the ligand bound can be calculated by dividing the product of the Bmax and the concentration of the ligand by the sum of the concentration of the ligand and the Kd
The Bmax is the total number of binding sites in prep
the problem with this is that you must account for non specific binding. When the drug is used, some of the drug will bind to low affinity sites. This can be removed by adding in a large amount of the cold ligand to out compete the hot ligand
Desensitisation of the receptors can happen due to:
loss of receptors (they become phosphorylated and internalised)
exhaustion of secondary messengers
physiological adaptation (muscle fatigue)
Tachyphylaxis - a piece of muscle where the response gets smaller. desensitisation is a possible mechanism that could underlie this
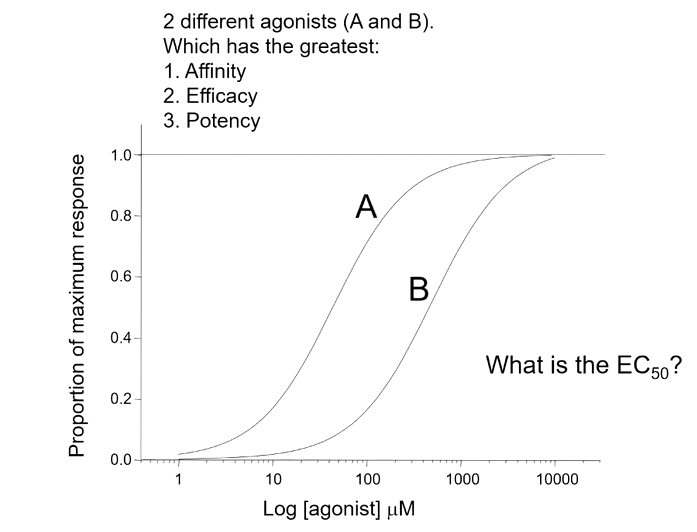
A has the greater potency potentially due to having a higher affinity
both have equal efficacy - both produce a maximum response
Having a higher potency means you get a bigger response at lower doses
Agonists are used in the clinic
adrenaline used to increase rate and force of contraction
salbutamol to treat asthma
dopamine
morphine
One type of agonist is called a partial agonist which cannot produce a full response. They do not necessarily have low affinity but they do have lower efficacy. This has the advantage of acting like both a blocker and an agonist so you reduce over activity but not the basal activity
Another type of agonist is an inverse agonist which produces the opposite response to an agonist
G protein coupled receptors
they can cycle without agonists (constitutive activity)
the inverse agonist will reduce the response by removing this activity
many antagonists are inverse agonists
GABA - A receptor
chloride channel that two gaba binds to to open the channel to let chloride through
without these receptors there would be seizure all the time as it controls the excitation levels in the brain
have a lot of modulatory sites one of which is called the benzodiazepine site
binding to this increases the frequency of opening of the receptor
an inverse agonist will bind to this site and decrease the action of gaba
a neutral agonist will block the site but don’t do anything
PAMs - positive allosteric modulator
NAMs- negative allosteric modulator
AgoPAMs - agonist with positive modulating activity
There can be sites within the transmembrane domain of G proteins which modulate the coupling to the G protein. A PAM will increase the coupling and make it more effective while the NAM will do the opposite. AgoPAMs activate the receptor also
This means that as there are many G proteins, they will all have these so new molecules can be produced to bind to these receptors. This means that if you want to reduce activity but not block it, a NAM can be used so that the activity is reduced but the same temporal pattern is still there
Antagonists - bind to the receptor but have no response
when applied at the same time as an agonist, the curve will be shifted to the right but with only the antagonist will have no graph.
A competitive antagonist will produce a graph that will still have a maximum response if there is enough agonist to outcompete it. there is a parallel shift
the potency of an antagonist can be found by measuring its Pa2 value
PA2 - negative log of the molar concentration of antagonist that reduced the effect of a known concentration of agonist to that of half the concentration.
the bigger the PA2 value, the better the antagonist. You must also consider receptor selectivity. Antagonists are also used in clinic
Non competitive receptors bind to allosteric sides or could bind to the ligand binding site covalently (non reversible)
The graph song have a parallel shift or a maximum response.
Spare receptors can be found using non competitive receptors. It could be only need to occupy a certain amount to get a maximum response, the spare receptors are called spare receptors.
this can be measured by using the non competitive antagonist:
when the NC antagonist is on, the receptors they are bound to can be removed so they cannot be activated by the agonist.
without any spare receptors, any of the receptors will reduce the maximum response
with spare receptors, the maximum response will not be affected as there will be enough receptors to produce it
because of spare receptors you don’t need to occupy all receptors for a full response. this means that the Kd does not always equal the EC50
reasons for spare receptors:
allows maximum response without occupying all receptors - increases system activity
in theory: the additional receptors can mop up excess agonist preventing an exaggerated response
the greater a receptor/ion channel is activated, the greater the block. this is done by opening the channel block or binding to inactivated state.
this has the advantages:
preserving basal activity
other activity is blocked.