Multiple Sclerosis
Welcome to the lecture Multiple Sclerosis referred as MS. MS is a chronic, progressive, degenerative disorder of the central nervous system (CNS). It is characterized by segmental demyelination of the nerve fibers of brain and spinal cord.
Please watch a short video in the hyperlink to understand pathophysiology behind the symptoms of multiple sclerosis.
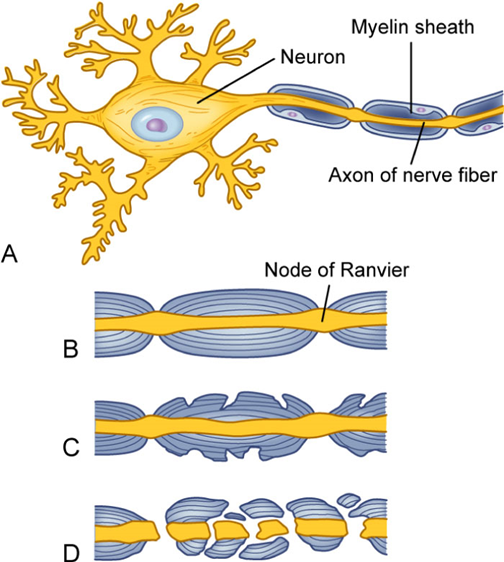
Picture on the slide shows different stages of myelin sheath disruption. On top part A shows Normal nerve cell with myelin sheath,
Part B- shows a normal axon
Part C shows Myelin breakdown
& in part D Myelin is totally disrupted resulting in an axon that cannot function.
Although the cause of MS is unknown, it is unlikely to be related to a single cause.
Genetically susceptible person is at risk for developing disease after an environmental exposure such as infection. Some of the precipitating factors can be infection, smoking, physical injury, emotional stress, excessive fatigue, pregnancy, and a poor state of health. It is believed that multiple genes are involved in the inherited susceptibility to multiple sclerosis and having a first-degree relative with MS increases a person’s risk of developing the disease.
Three pathologic processes for MS are characterized by
1.Chronic inflammation
2.Demyelination and
3.Gliosis which is scarring in the CNS-central nervous system.
●
Onset of the disease is often insidious and gradual, with vague symptoms occurring intermittently over months or years
The initial attacks cause damage to myelin sheaths of neurons in brain and spinal cord, and the nerve fiber is not affected initially. However, patient experiences noticeable impairment of function.
Transmission of nerve impulses still occurs, but it is slowed. At this stage myelin can regenerate , symptoms disappear and patient goes in remission. However in later stages, myelin loses its ability to regenerate due to ongoing inflammation causing disruption of the nerve impulse transmission resulting in loss of nerve function. Glial scar tissue is replaced with damaged tissue after inflammation subsides and leads to formation of hard, sclerotic plaques. These plaques are found throughout the white matter of the CNS.
The onset of multiple sclerosis disease is often insidious and gradual. The disease can manifest as chronic, progressive deterioration in some patients and
remissions and exacerbations in others. The overall trend is progressive deterioration in neurologic function. Initially the symptoms can be very vague and can occur intermittently over months to years. Patients often do not seek medical attention in this period as the symptoms are not serious enough subside on their own. The symptoms manifest according to areas of CNS involved. Some patients may have severe, long-lasting symptoms even early in the disease while others can have occasional mild symptoms for several years. Early signs and symptoms of MS include changes in motor skills, vision, and sensation. Some of the first symptoms of the disease may include nystagmus, blurry or double vision, red-green color distortion and blindness of one eye.
Motor manifestations of MS include weakness or paralysis of limbs, trunk, and head, spasticity of muscles and scanning speech. Scanning speech is when spoken words are broken into syllables. MS can cause partial or complete paralysis in the worst cases. Many patients experience muscle weakness in the extremities as well as problems with coordination and balance affecting a person’s ability to walk or stand.
Sensory manifestations of MS include numbness and tingling, pain especially in the low thoracic and abdominal regions, hearing loss, Vertigo and tinnitus, chronic neuropathic pain, Lhermitte’s sign which is sensory symptoms often described as an electric shock radiating down the spine or into the limbs with flexion of the neck.
Cerebellar manifestations of MS include Nystagmus which involves rapid and uncontrolled eye movements, Ataxia which is impaired balance, Dysarthria which involves slurred and slow speech and Dysphagia which is difficulty swallowing. Severe fatigue is present in many MS patients and can be a reason for significant disability in those patients. Heat, humidity, deconditioning, and some medication side effects can aggravate fatigue.
MS patients may experience bowel and bladder dysfunction if sclerotic plaque is located in areas of the CNS that control elimination. Usually patients experience constipation rather than fecal incontinence. Urinary problems can vary depending on spasticity or flaccidity of the bladder. In a spastic bladder, the bladder capacity is limited for urine that results in urinary urgency, dribbling and incontinence. In a flaccid bladder, there is large capacity for urine as there is no sensation or desire to void and patient feels no pressure or pain. Patients with flaccid bladder often experience urinary retention.
MS patients can also experience sexual dysfunction.
Cognitive manifestations for MS include difficulty with short-term memory, attention, information processing, planning, visual perception and word finding.
Emotional manifestations may include anger, depression and euphoria which is very rarely found , its a state of being unrealistically happy.
Please make sure to watch the video provided in the hyperlink to better understand the pathophysiology behind clinical manifestations of MS.
There is no definitive diagnostic test for MS. The diagnosis is primarily based on patient’s history , clinical manifestations, and results of certain diagnostic tests such as MRI or CT scan.
MRI of brain and spinal cord may show presence of plaques, inflammation, atrophy, and tissue breakdown and destruction that can help in diagnosis of MS.
Cerebral spinal fluid (CSF) analysis may show increased levels of Immunoglobulin G and presence of oligoclonal banding. Evoked potential responses are often delayed in persons with MS because of decreased nerve conduction.
So to diagnose MS there should be an evidence of at least 2 inflammatory demyelinating lesions on at least 2 different locations within CNS.
There should be damage or an attack occurring at different times usually more than a month apart.
Also, all other possible diagnoses must be ruled out.
Currently there is no cure for MS. The main goal of Interprofessional care is to treat the disease process and provide relief from the symptoms. The disease pattern is considered while creating a treatment plan. The early intervention is most effective in treatment of MS. Immunomodulator drugs are used to modify the disease progression and prevent relapses. Immunosuppressive therapy such as a combination of Cyclophosphamide (Cytoxan) and methylprednisolone (Solu-Medrol) can be used to stabilize the disease process. Some of the immunomodulators used in MS are
Interferon β-1a such as Rebif and Plegridy and Avonex
Interferon β-1b such as Betaseron and Extavia and
Glatiramer acetate (Copaxone)
Corticosteroids (methylprednisolone, prednisone) are useful in treatment of acute exacerbation as they help in reducing edema and acute inflammation at the site of demyelination.
IV immunoglobulin G treatment may be considered in acute exacerbations when treatment with corticosteroids alone does not achieve symptom improvement.
Therapeutic plasma exchange (plasmapheresis)- can also be used to remove antibodies responsible for the symptoms.
The other forms of drug therapy used in MS to treat symptoms involves muscle relaxants, CNS stimulants, Anticholinergics, Tricyclic antidepressants, Selective potassium channel blockers and Antiseizure drugs.
The Muscle relaxants are used for spasticity. CNS stimulants such as methylphenidate [Ritalin], and modafinil [Provigil]) are used to treat fatigue. Anticholinergics are used to treat bladder symptoms. Tricyclic antidepressants and antiseizure drugs are used for chronic pain syndromes.
The selective potassium channel blocker Dalfampridine (Ampyra) is used to improve walking speed in MS patients as it helps in improving nerve conduction in damaged nerve segments. Dalfampridine (Ampyra) should not be used in patients with a history of seizure disorders or moderate to severe kidney disease.
Currently there is no cure for MS. The main goal of Interprofessional care is to treat the disease process and provide relief from the symptoms. The disease pattern is considered while creating a treatment plan. The early intervention is most effective in treatment of MS. Immunomodulator drugs are used to modify the disease progression and prevent relapses. Immunosuppressive therapy such as a combination of Cyclophosphamide (Cytoxan) and methylprednisolone (Solu-Medrol) can be used to stabilize the disease process. Some of the immunomodulators used in MS are
Interferon β-1a such as Rebif and Plegridy and Avonex
Interferon β-1b such as Betaseron and Extavia and
Glatiramer acetate (Copaxone)
Corticosteroids (methylprednisolone, prednisone) are useful in treatment of acute exacerbation as they help in reducing edema and acute inflammation at the site of demyelination.
IV immunoglobulin G treatment may be considered in acute exacerbations when treatment with corticosteroids alone does not achieve symptom improvement.
Therapeutic plasma exchange (plasmapheresis)- can also be used to remove antibodies responsible for the symptoms.
The other forms of drug therapy used in MS to treat symptoms involves muscle relaxants, CNS stimulants, Anticholinergics, Tricyclic antidepressants, Selective potassium channel blockers and Antiseizure drugs.
The Muscle relaxants are used for spasticity. CNS stimulants such as methylphenidate [Ritalin], and modafinil [Provigil]) are used to treat fatigue. Anticholinergics are used to treat bladder symptoms. Tricyclic antidepressants and antiseizure drugs are used for chronic pain syndromes.
The selective potassium channel blocker Dalfampridine (Ampyra) is used to improve walking speed in MS patients as it helps in improving nerve conduction in damaged nerve segments. Dalfampridine (Ampyra) should not be used in patients with a history of seizure disorders or moderate to severe kidney disease.
Muscle relaxants can be helpful in relieving spasticity of muscles for most patients , however some patient may need surgery. The surgical procedures such as neurectomy, rhizotomy, cordotomy may be required. Dorsal-column electrical stimulation, or intrathecal baclofen (Lioresal) pump may also be an option for some patients.
Thalamotomy or deep brain stimulation can be used for tremors that become unmanageable with drugs.
Exercise helps in relieving spasticity of muscles and improving coordination. Physical therapy can help patients to train in substituting unaffected muscles for impaired muscles. Water exercise is also considered very helpful as water gives buoyancy to the body which allows the patient to have more control over the body and perform activities that would normally be impossible.
Nursing assessment involves collecting subjective as well as objective data. Subjective Data involves asking questions about Health history in terms of Muscle weakness or fatigue, tingling or numbness, muscle spasms, Blurred or lost vision, diplopia, vertigo, tinnitus, Decreased libido, impotence, Anger, depression, euphoria, isolation. Any viral infections or vaccinations, Residence in cold or temperate climates, Physical and emotional stress, Medications, Elimination problems, including urinary retention, incontinence or constipation, weight loss and dysphagia.
Objective Data includes observing/assessing patient for clinical manifestations such as
Apathy, inattentiveness, Pressure ulcers, Scanning speech, Tremor, Nystagmus, Ataxia, Spasticity
Hyperreflexia, decreased hearing, Muscular weakness, Paresis, Paralysis, Foot dragging and Dysarthria
In the nursing management, the main goal of care is to help patient in being able to maximize neuromuscular function, maintain independence in activities of daily living for as long as possible, manage disabling fatigue, optimize psychosocial well-being, adjust to the illness and decrease factors that precipitate exacerbations.
Nursing interventions involve helping patient to identify triggers and develop ways to avoid them or minimize their effects.
The diagnostic period can be very emotionally challenging for the patient, so we need to be available to provide emotional support and reassurance. Assist patients in dealing with anxiety and grief caused by diagnosis. Exacerbations of MS are triggered by Infections especially upper respiratory and urinary tract infection, trauma, fatigue, immunization, delivery after pregnancy, stress, and change in climate. Therefore, patient teaching should be provided to avoid triggers .
In acute exacerbation, the patient may be immobile and confined to bed, therefore nursing interventions should focus on preventing major complications of immobility, such as respiratory and urinary tract infections and pressure ulcers. Patient teaching should involve nutrition such as educating patient on nutritious, well-balanced meals and increase fiber intake if patient is constipated.
Teach patient on good balance of exercise and rest. Patient teaching must include information on treatment regimens, drug side effects, how to identify and manage side effects, and drug interactions with over-the-counter medications. Since MS patients take immunosuppressive therapy, therefore they should be taught to avoid people with any type of upper respiratory illness . Medication should be taken as prescribed and should not be stopped on their own. Women should be counselled that even though symptoms of MS may improve during pregnancy but the symptoms usually can get worse during the postpartum period. The infants of the women with MS are often smaller than gestational age. Bladder control is major problem in MS, mostly anticholinergic help in decreasing spasticity, however some patient may need to education on self catheterization. MS patients and care givers experience many emotional challenges and need to make many life style changes due to unpredictability of the disease. The National Multiple Sclerosis Society and its local chapters can offer a variety of services to meet the needs of patients with MS.








