Skeleton and Metabolism
Learning Objectives
Explain how the gut, kidneys and skeleton are involved in maintaining the homeostasis of calcium and phosphate
Explain the role of parathyroid hormone in the control of extracellular calcium concentration
Explain the role of vitamin D3 in calcium and phosphate metabolism
Explain how bone is an endocrine organ influencing phosphate homeostasis via the hormone FGF-23
Explain how disruptions to mineral homeostasis lead to metabolic bone diseases, and classify their pathogenesis.
Bone - Structure and Function
Function:
Support and movement: attachment site for muscles
Protection for internal organs
Provides a home for bone marrow
Acts as a mineral reservoir
Endocrine: source of some ‘non-classical’ hormones
Structure:
Cortical - compact
Trabecular - spongy cancellous
Composition:
Protein: organic osteoid matrix (25%) - mainly type 1 collagen → flexibility and tensile strength
Mineral (75%) - hydroxy apatite, calcium and phosphate and rigid, brittle - high compressive strength
Cells:
Osteoblasts - Bone-forming cells. They secrete the organic matrix (osteoid) and participate in its mineralization.
Osteoclasts - Bone reabsorbing cells. They remove old bone by dissolving the mineral and digesting the protein matrix.
Osteoclasts and osteoblasts work together in a continual cycle of eating away old bone and replacing it with new. This is called remodelling and is essential for skeletal health.
Osteocytes are terminally differentiated osteocytes. A fraction of the osteoblasts become embedded within the bone matrix they secrete.
Osteocytes maintain the balance between bone resorption and formation.
Organs in Maintenance of Homeostasis
Bone can serve as a metabolic organ as the bone turnover serves as a homeostasis of serum calcium, and phosphate in conjunction with
PTH
Vitamin D
Calcitonin
FGF-23 - hormones that are secreted from the skeleton and osteocytes themselves - endocrine effects
Oestrogen - health
Androgen - health; aromatase deficiency in men can lead to osteoporosis
Cortisol - high levels of cortisol promote bone reabsorption (long-term can lead to bone mass loss)
Calcium is not just responsible for our bone strength, but it is the source of electrical energy in our nervous system and muscles
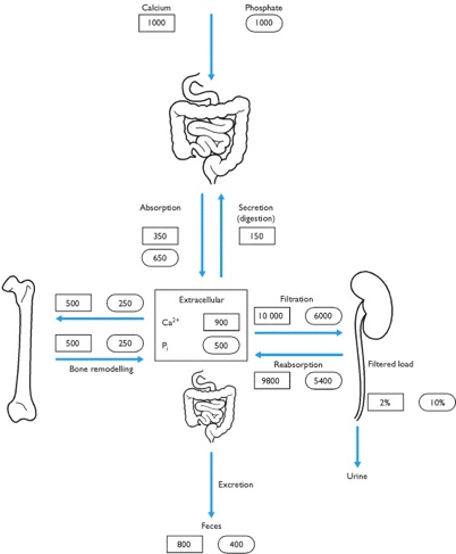
1. The Gut:
Absorption: Calcium and phosphate are absorbed from dietary intake through the intestinal lining.
Vitamin D’s Role:
Vitamin D3 (calcitriol) increases calcium absorption by stimulating the production of calcium-binding proteins in intestinal cells.
Phosphate absorption is also facilitated by Vitamin D.
• Net Balance:
Of 1000 mg/day of dietary calcium, ~200 mg is absorbed into the blood.
Of 1000 mg/day of dietary phosphate, ~650 mg is absorbed.
2. The Skeleton:
• Reservoir: The skeleton stores ~99% of body calcium and ~85% of phosphate as hydroxyapatite crystals.
• Remodeling:
• Bone is constantly remodelled by osteoclasts (which release calcium and phosphate into the blood) and osteoblasts (which redeposit them into bone).
• Hormonal Regulation:
• PTH: Stimulates osteoclasts to release calcium and phosphate when blood calcium is low.
• Calcitonin: Promotes osteoblast activity to deposit minerals back into bone.
3. The Kidneys:
• Filtration and Reabsorption:
• The kidneys filter calcium and phosphate, but most of it is reabsorbed to avoid excess loss.
• PTH increases calcium reabsorption and phosphate excretion.
• FGF-23 decreases phosphate reabsorption to maintain appropriate blood levels.
• Fine-tuning:
• ~200 mg/day of calcium and ~600 mg/day of phosphate are excreted in urine.
Coordination: These organs work together to maintain stable calcium (~2.2-2.6 mM) and phosphate levels while balancing absorption, storage, and excretion.
Coordinated Regulation of Homeostasis:
1. Calcium Homeostasis:
• When blood calcium levels drop:
• PTH increases bone resorption (calcium release), promotes kidney reabsorption of calcium, and stimulates calcitriol production to boost intestinal calcium absorption.
• When blood calcium levels rise:
• Calcitonin suppresses bone resorption and increases calcium deposition in bone.
2. Phosphate Homeostasis:
• Phosphate levels are regulated by:
• FGF23, which reduces phosphate absorption in the gut and reabsorption in the kidney.
• PTH, which decreases renal phosphate reabsorption to enhance excretion.
3. Interplay:
• Calcium and phosphate must remain in balance to prevent excessive deposition in soft tissues or inadequate mineralization of bone.
• Vitamin D plays a central role in harmonizing absorption, storage, and excretion.
Key Takeaways:
• The gut is responsible for absorbing dietary calcium and phosphate, influenced by Vitamin D.
• The skeleton serves as a storage depot, releasing or storing minerals based on hormonal signals (PTH, calcitonin, Vitamin D).
• The kidneys filter the minerals, reabsorbing most of them and excreting the excess to fine-tune their levels in the blood.
PTH - extracellular calcium concentration control
PTH is synthesised by parathyroid chief cells
Secreted as 84 AA polypeptide
Short half-life in circulation (<5 min)
Parathyroid. 80K cells continuously monitoring blood Ca, and increasing or decreasing PTH secretion accordingly.
There are 4 of these that sit behind the thyroid gland and consist of about 80,000 cells. This is first transcribed as a pre-pro hormone, the signal sequence is then cleaved in the ER and then the Golgi and this produces your 84 amino acid polypeptide. The chief cells of the PTH glands defend against hypocalcemia.
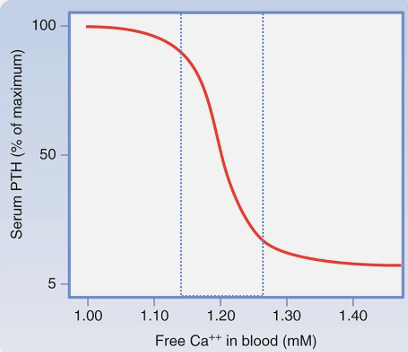
The major role of the PTH is defence against hypocalcaemia. The plasma calcium is maintained at 2.2-2.6mM (and the free ionised calcium is approximately half). The free calcium is what is sensed by the GPCR on chief cells and the calcium binding prevents and suppresses the PTH release. The calcium binding triggers intracellular signalling and it suppresses the PTH release. You can see from this graph that between 1.1-1.3mmol, the calcium concentration more steeply affects the PTH release. The PTH secretion increases when calcium is too low.
The actions of PTH are that:
• Promotes release of Ca from bone (and also phosphate in equal quantities)
• Increases renal Ca reabsorption (from the GI tract)
• Increases renal Pi excretion
• Upregulates 1α hydroxylase activity
There is negative feedback control of the PTH and you have to ensure the sufficient calcium is in the circulation to aid the bone growth process. There is therefore an increased absorption from the diet. In the absence of vitamin D, the absorption is poor. (osteomalacia in adults and rickets in children, which is just a lack of vitamin D meaning that your bones are very soft).
• 99% of body calcium is in bone
• Remaining 1% is mainly intracellular
• Hormonal control of the tiny (<0.1%) extracellular fraction is what maintains Ca balance
• With the PTH, there is a release of calcium and phosphate as when the bone is dissolved, both are released in equal quantities. You have to increase the calcium reabsorption from the kidney tubule and you don’t want to raise the phosphate, so there is an opposing action here.
Actions of PTH on the bone:
• PTH receptors on osteoblasts and osteocytes (there are no receptors on the osteoclasts but it activates indirectly by RANK L or indirectly by intermediate cytokines to produce RANK L).
• Promotes bone formation / remodelling
• Activates osteoclasts via RANKL
• Promotes bone remodelling (osteocytes used in bone formation)
Effect depends on concentration dynamics
• Intermittent low doses are anabolic
• Persistent high concentration leads to excess resorption over formation – bone loss
• Anabolic steroids promote bone remodelling and formation (more though) and this process releases bone mineral.
• PTH can be used to treat osteoporosis in a specific dose, time and it will work.
• Calcium homeostasis is central to the role of this PTH.
Vit D3 - calcium and phosphate metabolism
• Calcitriol (really a steroid hormone, not a vitamin!)
• Synthesised in skin in response to exposure to UV (‘sunshine vitamin’). There is a cholesterol derivative in the skin (7-dehydrocholesterol) which is converted to a prohormone, cholecalciferol. There are 2 steps to activate it.
• Activated by 2 metabolic steps
• 25 hydroxylation in liver to form 25OH D3, major circulating metabolite
• 1α hydroxylation of 25 OH D3 in kidney produces 1,25(OH)2 D3, or calcitriol, the active hormone
• Calcitriol is the active form of vitamin D3.
Nuclear receptor, VDR, typical steroid, DNA binding element, etc. Dimerises with RX receptor. Effects mainly increasing (sometimes decreasing) transcription of target genes.
The 1α hydroxylase enzyme determines the level of active hormone produced as the 25-hydroxycholecalciferol is longer lasting and more stable. You can then measure this for any assays that you want to do.
Site of regulation is control of 1α hydroxylase in kidney
Increased by
• PTH
• Low phosphate
Actions:
• Increase absorption of Ca and Pi from GI tract
Little absorption in absence
• Inhibits PTH secretion (transcription)
• Complex effects on bone, generally in synergy with PTH
The only way to increase the body’s Ca reservoir is via absorption from the gut, and little takes place in the absence of vitamin D.
VDR (vitamin D receptor) knockout mice develop hypocalcaemia, secondary hyperparathyroidism, and rickets, indicating a role for 1,25(OH)2D3 in bone mineralization. However, a diet high in calcium and phosphate rescues the abnormal mineral biochemistries and bone phenotype in the VDR knockout mouse, indicating that the main effects of 1,25(OH)2D3 on bone are to provide sufficient calcium and phosphate for normal mineralization, particularly by mediating intestinal calcium and phosphate absorption.
Calcitriol also has important secondary effects on PTH secretion. By increasing calcium uptake in the gastrointestinal system, calcitriol increases plasma calcium, maintaining PTH secretion at low levels and thus favouring osteoblast action and protecting bone structure.
A low serum phosphate means that there is higher calciferol synthesis and therefore activates vitamin D production.
FGF-23 - bone influencing phosphate homeostasis
FGF-23 is a hormone secreted by osteocytes.
Discovered in 2000
• Hypophosphatemic rickets: rare phosphate-wasting conditions leading to bone mineralization defects (osteomalacia)
• Consortium investigating autosomal-dominant HR (ADHR) traced mutation in gene that turned out to be FGF-23
• Central role in phosphate homeostasis
The FGF is identified as a growth factor. It is phosphate wasting, so you have an excessive loss in the urine. The kidneys are not reabsorbing phosphate and this is a problem in bone mineralisation. This is a gain of function mutation and this increases the functions of FGF. The recognition site of the peptide has to be cleaved to activate it and in the missense mutation, the site is not activated so this provides a gain of function mutation.
Actions of FGF-23 are:
• Expressed and secreted by osteocytes
• Increased by calcitriol and Pi
• Inhibits calcitriol synthesis
• Increases renal Pi excretion (by reducing Na-Pi reabsorption from proximal tubule)
• Normally, the FGF should lower phosphate levels, but you have a fain of function mutation and you have a lower amount of phosphate, which means you have phosphatemia.
There is a lower sodium / phosphate co-transporter in the kidney tubule and this contributes to the homeostatic levels. An increase in phosphate means an increase in FGF-23, which lowers the phosphate in a negative feedback mechanism. Calcitriol acts as a stimulus to increase the secretion of FGF and the FGF inhibits calcitriol synthesis. You then get control of phosphate levels and there is a lower level of plasma phosphate in response to the rises of FGF-23.
Metabolic bone disease
Normal range 2.2 – 2.6 mM (normal for >35 years)
Hypocalcaemia
Hypercalcaemia
Clinical features of too much calcium (hypercalcaemia) are that:
• Depression, fatigue, anorexia, nausea, vomiting,
• Abdominal pain, constipation
• Renal calcification (kidney stones)
• Bone pain
"painful bones, renal stones, abdominal groans, and psychic moans,"
• Severe: cardiac arrhythmias, cardiac arrest
This hypercalcaemia is not uncommon but can go undetected. There are very diffuse symptoms, including mostly neurogenic symptoms. If there is a prolonger hypercalcaemia, then this means that you get kidney stones.
Causes of hypercalcaemia are:
Most common causes:
• In ambulatory patients: primary hyperparathyroidism (advanced cancer of malignancy)
• In hospitalized patients: malignancy
Less common causes include:
• Hyperthyroidism
• Excessive intake of vitamin D
Primary hyperparathyroidism:
• Usually due to a benign adenoma in one or more PT glands (increase in PTH changes the set point and resets the calcium to higher levels and keeps it there.
• Often detected on screening – many patients asymptomatic
• ~10% of patients present with clinical evidence of bone disease (persistently high levels of PTH can cause osteoporosis).
• 10 - 20% of patients present with kidney stones
• Resolved by surgical removal of affected gland(s)
There is also hypercalcaemia of malignancy:
• Common problem of advanced malignancy
• Tumour may secrete PTH-related peptide, binds and activates PTH receptor
• This is very rare though and only present in terminally ill patients. The PTH related peptide produces hypercalcaemia after binding to the PTH receptor and over 2.6mmol indicates a low PTH.