Nutrition Basics: Micronutrients
- ]]Define the terms: vitamin and mineral.]]
- ==Vitamins== - organic essential nutrients required in tiny amounts to perform specific functions that promote growth, reproduction, or the maintenance of health and life. Both fat soluble and water soluble.
- Properties of fat soluble - stored in the body so deficiencies appear more slowly. Greater potential for toxicity.
- %%Vitamins A, D, E, K%%
- Properties of water soluble - excess is secreted because most are not stored. Deficiencies may appear more quickly.
- %%B-vitamins, Vitamin C%%
- ==Minerals== - inorganic, essential nutrients required in varying amounts that function primarily as structural components or regulators of body processes
- E.g. calcium, magnesium, potassium (macrominerals)
- E.g. iron, zinc, fluoride, chromium (microminerals)
- ==Vitamins== - organic essential nutrients required in tiny amounts to perform specific functions that promote growth, reproduction, or the maintenance of health and life. Both fat soluble and water soluble.
- ]]Explain the difference between enrichment and fortification.]]
- %%Enrichment%% - addition of nutrients to replace those lost in food processing
- %%Fortification%% - addition of nutrients to foods that didn’t have them in the first place
- ]]Discuss circumstances when it might be suitable to supplement with vitamins and/or minerals.]]
- Vitamin and mineral needs should usually be met by eating a balanced diet with a variety of foods
- Health Canada fortifies many foods in an effort to prevent nutritional deficiencies
- Vitamins A + D → added to milk and margarine
- B vitamins + iron → added to enriched flour
- Iodine → added to table salt
- Supplements might be recommended when:
- Requirements are increased
- Difficult to obtain sufficient amounts from diet (e.g. pregnant/lactating women → folic acid, iron)
- Drug-nutrient interactions
- Smokers (vitamin C)
- Intake from diet is likely inadequate
- People on low calorie diets (<1600 kcal/day)
- Those who avoid entire food groups (vegetarians/vegans)
- Chronic substance abuse
- Elderly with a poor diet
- Lactose intolerant (may need calcium)
- Malabsorption is a risk
- Following bariatric surgery (e.g. gastric bypass, weight loss surgery)
- GI diseases known to cause malabsorption (e.g. cystic fibrosis)
- Elderly
- Therapeutic uses
- Correction of a deficiency (UL do not apply)
- To prevent or treat a disease or condition unrelated to a deficiency (e.g. Vit B6 for CV disease, Vit C for cold)
- ]]For each nutrient be able to discuss its: chemical name of active substances/forms (if given); physiological function in the body; symptoms of deficiency and explain circumstances under which this might occur; adverse effects associated with excess intake; therapeutic use and evidence (other than to correct a deficiency)]]
- ==Anti-oxidant vitamins==
- %%Vitamin A and beta-carotene%%
- Sources: animal (vitamin A - preformed), plant (carotenoids - most potent is B-carotene (precursor form))
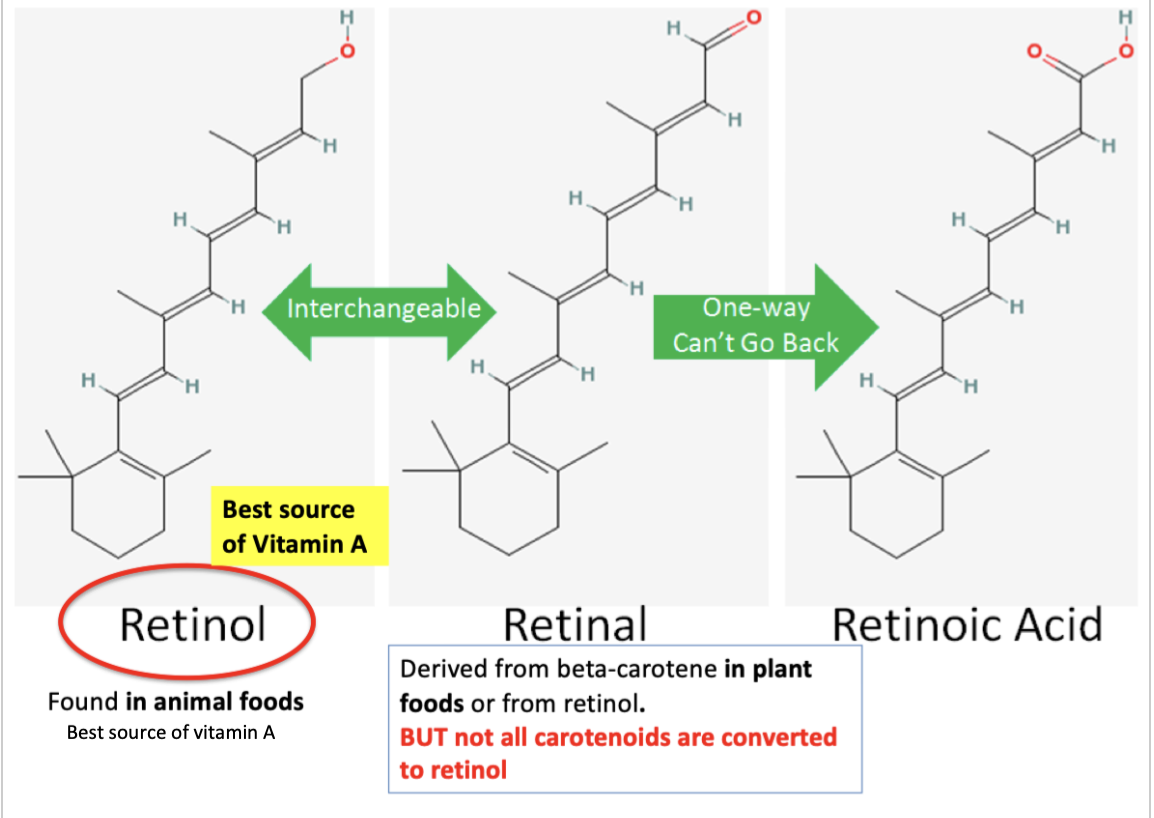
- 3 forms of vitamin A are active in the body, each with a different role. Collectively called retinoids
- Retinol (used in reproduction)
- Retinal (used in vision)
- Retinoic acid (used to regulate growth)
- ==Anti-oxidant vitamins==
 * Beta-carotene from supplements is better absorbed than that from diet
* Some carotenoids (e.g. lutein, lycopene) have no vitamin A activity (i.e. won’t produce retinol)
* Physiological function:
* Promote vision (esp. night vision) → in the retina, vitamin A in the form of retinal makes rhodopsin, a light sensitive pigment that carries visual information to the brain
* Maintains the health of epithelial tissue and skin (via protein synthesis and cell differentiation) → growth
* Fetal development, growth and cell differentiation → reproduction
* Supports overall immune function
* Beta-carotene: can convert to vitamin A (in the intestinal mucosa and liver), or if unconverted, has anti-oxidant properties
* Deficiencies:
* Very rare in North America, but common in undeveloped countries (in association with malnutrition)
* Night blindness: without Vitamin A in the diet (→ liver stores get exhausted), this cycle comes to a halt because there is not enough retinal in the retina to regenerate rhodopsin, and the ability to see in low light decreases
* Toxicity and effects:
* Intake > 1500 mcg (2x the RDA) is associated with decreased bone density and increased risk of fracture in adults → can lead to osteoporosis
* Teratogenic → if excess of 10,000 IU or 3,000 mcg/d are taken during the first 2 months of pregnancy → increases chance of birth defects @@(AVOID)@@
* Therapeutic uses:
* Vitamin A - only in the correction of a deficiency
* %%Beta-carotene:%%
* Investigated due to anti-oxidant activity (but no benefit in reducing risk of cancer or CVD)
* 2 studies found increased risk of lung cancer in smokers
* Increased risk in total mortality
* Used for ^^treatment of macular degeneration^^
* %%Vitamin E%%
* 8 naturally occurring anti-oxidant forms (called tocopherols)
* Alpha-tocopherol is the only form that our bodies can use; found in circulation and tissues
* Alpha-tocopherol and Vitamin E are used interchangeably
* Dietary sources of alpha-tocopherol: vegetable oils, nuts, meat, poultry, eggs, and whole grains (food high in FAT)
* Synthetic (dl-a-tocopherol) → 8 isomers (only ½ are active in body)
* Natural (d-a-tochopherol) → provides twice the biological activity as synthetic form
* Supplements:
* Made from both synthetic and natural Vit E
* Content expressed IU
* Synthetic Vit E contains less of the active form, often sold in higher doses
* Physiological function:
* No metabolic function
* Lipid-soluble anti-oxidant
* Protect cell membranes against oxidative damage by free radicals
* Protects lipids from oxidation
* Deficiencies:
* Very rare; may be found with diseases of fat malabsorption (such as cystic fibrosis)
* Toxicity and effects:
* Risk of bleeding at higher doses (especially with synthetic form); and,
* Vitamin E and warfarin together have been observed to increase risk of bleeding
* Therapeutic uses:
* May slow the progression of ^^Alzheimer’s Disease^^ by 6 months → no evidence for prevention of dementia
* CVD → results have been largely negative, with some harmful outcomes (increased risk of heart failure, mortality, stroke)
* Wound healing/scar prevention (topical) → not shown to be effective
* Cancer → 400 IU of Vit E every other day did not reduce the overall risk of cancer in men
* may actually increase risk of prostate cancer → supplements, not foods
* ^^BOTTOM LINE: supplementing may actually be harmful^^
* %%Vitamin C%%
* Also known as ascorbic acid
* Physiological function:
* Act as coenzyme involved in collagen synthesis (helps with wound healing), carnitine production, and neurotransmitter (noradrenaline) formation
* Act as an anti-oxidant
* Defends against free-radicals (or neutralizes free radicals)
* Protects tissues from oxidative damage, so may help prevent diseases
* Regenerates other antioxidants within the body (e.g. Vitamin E)
* Deficiencies:
* Severe deficiency, scurvy is uncommon (need Vit C intake to be
* Beta-carotene from supplements is better absorbed than that from diet
* Some carotenoids (e.g. lutein, lycopene) have no vitamin A activity (i.e. won’t produce retinol)
* Physiological function:
* Promote vision (esp. night vision) → in the retina, vitamin A in the form of retinal makes rhodopsin, a light sensitive pigment that carries visual information to the brain
* Maintains the health of epithelial tissue and skin (via protein synthesis and cell differentiation) → growth
* Fetal development, growth and cell differentiation → reproduction
* Supports overall immune function
* Beta-carotene: can convert to vitamin A (in the intestinal mucosa and liver), or if unconverted, has anti-oxidant properties
* Deficiencies:
* Very rare in North America, but common in undeveloped countries (in association with malnutrition)
* Night blindness: without Vitamin A in the diet (→ liver stores get exhausted), this cycle comes to a halt because there is not enough retinal in the retina to regenerate rhodopsin, and the ability to see in low light decreases
* Toxicity and effects:
* Intake > 1500 mcg (2x the RDA) is associated with decreased bone density and increased risk of fracture in adults → can lead to osteoporosis
* Teratogenic → if excess of 10,000 IU or 3,000 mcg/d are taken during the first 2 months of pregnancy → increases chance of birth defects @@(AVOID)@@
* Therapeutic uses:
* Vitamin A - only in the correction of a deficiency
* %%Beta-carotene:%%
* Investigated due to anti-oxidant activity (but no benefit in reducing risk of cancer or CVD)
* 2 studies found increased risk of lung cancer in smokers
* Increased risk in total mortality
* Used for ^^treatment of macular degeneration^^
* %%Vitamin E%%
* 8 naturally occurring anti-oxidant forms (called tocopherols)
* Alpha-tocopherol is the only form that our bodies can use; found in circulation and tissues
* Alpha-tocopherol and Vitamin E are used interchangeably
* Dietary sources of alpha-tocopherol: vegetable oils, nuts, meat, poultry, eggs, and whole grains (food high in FAT)
* Synthetic (dl-a-tocopherol) → 8 isomers (only ½ are active in body)
* Natural (d-a-tochopherol) → provides twice the biological activity as synthetic form
* Supplements:
* Made from both synthetic and natural Vit E
* Content expressed IU
* Synthetic Vit E contains less of the active form, often sold in higher doses
* Physiological function:
* No metabolic function
* Lipid-soluble anti-oxidant
* Protect cell membranes against oxidative damage by free radicals
* Protects lipids from oxidation
* Deficiencies:
* Very rare; may be found with diseases of fat malabsorption (such as cystic fibrosis)
* Toxicity and effects:
* Risk of bleeding at higher doses (especially with synthetic form); and,
* Vitamin E and warfarin together have been observed to increase risk of bleeding
* Therapeutic uses:
* May slow the progression of ^^Alzheimer’s Disease^^ by 6 months → no evidence for prevention of dementia
* CVD → results have been largely negative, with some harmful outcomes (increased risk of heart failure, mortality, stroke)
* Wound healing/scar prevention (topical) → not shown to be effective
* Cancer → 400 IU of Vit E every other day did not reduce the overall risk of cancer in men
* may actually increase risk of prostate cancer → supplements, not foods
* ^^BOTTOM LINE: supplementing may actually be harmful^^
* %%Vitamin C%%
* Also known as ascorbic acid
* Physiological function:
* Act as coenzyme involved in collagen synthesis (helps with wound healing), carnitine production, and neurotransmitter (noradrenaline) formation
* Act as an anti-oxidant
* Defends against free-radicals (or neutralizes free radicals)
* Protects tissues from oxidative damage, so may help prevent diseases
* Regenerates other antioxidants within the body (e.g. Vitamin E)
* Deficiencies:
* Severe deficiency, scurvy is uncommon (need Vit C intake to be
- ==Nutrients for metabolism==
- %%B vitamins%%
- Help body use fuel from energy-yielding nutrients (carbs, fats, proteins)
- Can work individually and interdependently
- 8 essential B vitamins
- %%Thiamine (B1)%%
- Dietary sources:
- Whole grain products, legumes (e.g. beans and lentils), nuts, meat (esp. pork) and yeast
- Canada → wheat flour is fortified with thiamine
- Lost during production of white flour and white rice
- Physiological function:
- Essential co-enzyme (thiamine pyrophosphate - TPP) used in carb and amino acid metabolism
- Required for the formation of acetyl-CoA from pyruvate and ATP generation
- Deficiencies:
- Dietary (developing countries)
- Rare in Western countries due to consumption of whole grain products (exceptions: malnourished (homeless), alcohol abuse)
- Beriberi - condition that can happen after prolonged deficiency which can result in both neurological (peripheral neuropathy) and cardiac symptoms (heart failure)
- Wernicke-Korsakoff Syndrome - severe deficiency caused by alcohol abuse (impairs thiamine absorption and increased excretion in urine). Symptoms include: jerky eye movements and motor abnormalities
- Therapeutic uses:
- Prevention and treatment of thiamine deficiency
- Other uses under investigation: Alzheimer’s disease, Diabetes
- Marketed to provide “more energy” → does provide ATP but doesn’t increase energy levels (unless you are deficient)
- No UL; no known toxicity
- %%Riboflavin (B2)%%
- Dietary sources:
- Found in many different foods in small amounts; milk, yogurt, fortified cereal, beef, enriched grains
- Physiological function:
- converted to coenzymes FMN (flavin mononucleotide) and FAD (flavin adenine dinucleotide) - FAD is part of electron transport chain that produces ATP
- Involved in the activation + metabolism of vit B6, folic acid, niacin (other B vitamins) to their active forms in the body (example of interdependency)
- Deficiencies:
- Rarely happens because it’s recycled in the body and widely available in foods
- Therapeutic use:
- ^^Migraine prophylaxis^^ - taking high dose (400mg/day) for 3 months can decrease frequency and number of headache days
- %%Niacin (B3)%%
- Dietary sources:
- Milk, eggs, meat, poultry, fish, whole-grain, fortified cereals, nuts and all protein containing foods
- Physiological function:
- The coenzymes NAD and NADP are required in many oxidative-reduction reactions including glycolysis. Helps body to metabolize carbohydrates, fats, and proteins.
- Both niacin forms are converted to the niacin coenzyme
- Deficiencies:
- Pellagra - inability to absorb niacin may cause this. Dermatitis, diarrhea, and dementia (if left untreated - death)
- Secondary deficiency can occur from malabsorption (chronic alcohol abuse, anorexia, prolonged diarrhea)
- Toxicity and effects:
- when used in high doses may see pruritus, GI distress, and abnormal liver function
- When taken at therapeutic levels to resolve hyperlipidemia, common adverse effects including flushing and other vasodilation symptoms (flushing can be reduced by ASA or NSAIDs before niacin dose)
- Therapeutic uses:
- Effective at ^^lowering LDL^^ and ^^increasing HDL^^
- ^^Treatment of Pellagra^^
- %%Pantothenic acid (B5)%%
- %%Pyridoxine (B6)%%
- Dietary sources:
- Meats, fish, poultry, bananas, and blueberries, fortified cereals
- Occurs in 3 forms: Pyridoxine, pyridoxal, pyridoxamine → all 3 can be converted to co-enzyme ^^pyridoxal phosphate (PLP)^^
- Physiological function:
- PLP acts as a co-enzyme used in amino acid, glycogen and fatty acid metabolism (a co-factor for more than 100 enzymes)
- Helps to convert tryptophan to niacin and serotonin
- B6, B12 and folate → work together to lower homocysteine levels
- Helps to make RBCs
- Deficiencies:
- It synthesizes key neurotransmitters
- Early signs of B6 deficiency include depression and confusion
- Low levels of B6 have been associated with increased risk of some cancers and CV disease
- Can be drug induced
- Toxicity and effects:
- High doses B6 (>20 mg/day) and B12 (>55 mcg) have been associated with increased risk of lung cancer by 2-fold (in men only and greater in smokers)
- Can cause sensory neuropathy with intakes >200 mg/day for several months
- Therapeutic uses:
- ^^Pre-menstrual syndrome (PMS)^^ - 50-100 mg/day may be of value to treat PMS, mostly mood symptoms
- Depression - benefit is questionable, although in seniors it did show decrease in depression symptoms
- ^^Morning sickness^^ - somewhat effective for nausea in pregnancy
- ^^CVD^^ - elevated homocysteine can lead to heart disease. Studied alone and in combo with B12 and folic acid - mixed evidence.
- %%Biotin (B7)%%
- Part of a co-enzyme used in energy metabolism, fat synthesis, amino acid metabolism and glycogen synthesis
- Food sources: yogurt, nuts, eggs, salmon, sweet potatoes
- Also produced by GI bacteria
- Deficiency:
- Extremely rare - skin rashes, thinning hair and brittle nails
- Therapeutic uses:
- ^^Brittle nails^^ - may improve nail thickness and splitting of brittle nails
- ^^Hair growth and improving skin^^ - only in children + case reports
- %%Folic acid (B9)%%
- %%Cobalamin (B12)%%
- Dietary sources:
- exclusively animal sources: meat, fish, poultry, milk, cheese, eggs; fortified foods like cereal
- Our ability to absorb from dietary supplements is limited by the capacity of intrinsic factor - only about 10 mcg of a 500 mcg oral supplement is actually absorbed in healthy people
- ^^Stomach acid and intrinsic factor^^ are required for the absorption of B12
- Physiological function:
- Interdependent role with folate (coenzyme in folate and fatty acid metabolism)
- Required for normal nerve function
- Assists hemoglobin and red cell production
- Lowers homocysteine levels
- Deficiencies:
- elderly
- Pernicious anemia (lack of intrinsic factor) - main cause
- Atrophic gastritis (decrease in stomach pH)
- Vegan diet
- It could take up to 3 years once eliminating animal sources due to recycling of B12 in the body
- Surgery in the GI tract
- GI disorders (Celiac, Chron’s)
- Can be drug induced
- Toxicity and effects:
- No UL; no known toxicity
- High doses - increased risk of lung cancer (men and smokers)
- Therapeutic uses:
- Treatment of vitamin B12 ^^deficiency^^ in patients with pernicious anemia, malabsorption disorders of neurological involvement
- People at risk of deficiencies: elderly, vegans or strict vegetarians
- Because 10-30% of older people don’t absorb food-bound B12, those ^^>50 y/o are advised to supplement^^
- May decrease risk of developing ^^age-related macular degeneration^^ when combined with B6 + folic acid
- Energy and endurance - no beneficial effect on performance in the absence of a nutritional deficit
- ^^CVD^^
- %%B vitamins%%
- ==Nutrients for bone health==
- %%Calcium%%
- Dietary sources:
- Mainly from milk and dairy products
- Green leafy vegetables (broccoli, bok choy, kale)
- Salmon and sardines
- Physiological function
- \ > 99% of calcium is stored in bone, which acts as a reservoir and helps with bone structure
- Required for: cell signalling, current flow across excitable membranes, muscle contraction, blood coagulation, formation structure and remodelling of the skeleton (bone growth and density)
- VERY IMPORTANT that calcium levels in blood and ECF be maintained within very narrow limits to support normal physiological functions
- Regulated by PTH and calcitonin (regardless of dietary intake)
- When plasma Ca2+ levels are low, the bones suffer (PTH pulls from bone)
- Requires adequate levels of vitamin D
- Deficiencies
- Silent (no symptoms) - also blood calcium remains normal
- If chronic inadequate intake:
- May prevent attainment of peak bone mass (i.e. max calcium stores)
- May contribute to accelerated bone loss and development of osteoporosis
- Toxicity and effects:
- High doses can cause kidney stones
- Most common: constipation (Mg can offset this - but too much causes diarrhea)
- Calcium-alkali syndrome: caused by very high doses of calcium carbonate, leading to hypercalcemia, vascular and soft tissue calcification, and renal insufficiency
- Therapeutic uses
- ^^Dyspepsia^^ (calcium carbonate)
- ^^Renal failure^^ (calcium acetate + carbonate are phosphate binders)
- ^^Lactose intolerant^^
- No evidence for fracture prevention in healthy adults
- Calcium carbonate (TUMS)
- 40% calcium content (highest)
- Needs acidic environment for best absorption - take with food
- Don’t use if on PPI or H2RA
- SE: gas/bloating/constipation
- Absorption is greatest when each dose does not exceed 500mg - recommended divided doses
- If combined with vit D or K, take with a fatty meal to increase absorption
- Calcium citrate
- 21% calcium
- Absorption independent of stomach pH
- Larger pills required to get same dose
- Less side effects
- Interactions:
- Decreased absorption of bisphosphonates, levothyroxine, antibiotics (quinolones, tetracycline) - space up to 4 hrs apart
- Thiazides decrease calcium excretion by the kidneys → hypercalcemia or calcium-alkali syndrome (concern if taking large amounts of Ca carbonate)
- IV calcium: can cause precipitation of some drugs (e.g. ceftriaxone)
- Dietary sources:
- %%Vitamin D%%
- Two forms: ergocalciferol (D2) from yeasts and fungi; cholecalciferol (D3) from animal tissues
- Sources:
- Formed naturally in the skin on exposure to UVB (endogenous production) - main source
- Foods: fatty fish (mackerel, salmon, sardines), fish liver oils, egg yolks, or fortified milk
- Natural Health Products - most are D3
- All produce calcidiol, which will then go on to produce the active form (calcitriol, a steroid hormone)
- Production and activation
- Vit D3 is produced in the skin epidermis then taken to the liver for activation
- Next, transported to the kidney for secondary hydroxylation to the active form, calcitriol
- Vit D2 also gets converted to calcidiol - but D2 is less active
- Physiological function
- Together with calcitonin and PTH, it regulates plasma calcium - helps support normal bone mineralization, neuromuscular function and cell physiology
- Also has widespread receptors (brain, prostate, breast, colon, immune cells, etc.)
- Can regulate the expression of >2500 genes involved in skeletal and other biological functions (e.g. decreases cell proliferation of normal and cancer cells and induces their differentiation)
- Influences immune cell function
- Generally lowers inflammation
- Deficiencies
- Deficiency is rare but insufficiency is very common
- Factors that lead to deficiency include:
- Dark skin (melanin absorbs UVB and competes with vit D)
- Exclusively breastfed infants without Vit D supplement
- Lack of sunlight or covering all exposed skin (or using SPF >= 8 or greater when outside)
- Not using fortified milk
- In Vancouver, only not getting adequate UV levels in November to February
- Elderly → deficiency very likely
- Lose ability to make and activate Vit D
- Drink less milk
- Stay indoors more (and cover up when they go outside)
- \ > ^^51 y/o → take 400 IU of Vit D in supplement form each day (in addition to what they consume through diet)^^
- Signs of deficiency:
- Rickets (children)
- Failure to mineralize new bone
- Results in soft bones, deformed joints
- Osteoporosis
- Osteomalacia - generalized decreased in bone density and mineralization, with muscle weakness, bone pain
- Toxicity and effects
- Hypercalcemia (very rare)
- raises concentrations of blood calcium leading to weakness, fatigue, headache, N/V/D
- Impaired renal fxn
- Can lead to: calcification of soft tissues, irreversible kidney failure
- UL: 4000 IU/day (adults and children)
- Toxicity is seen at doses >10,000 IU/day
- Therapeutic uses
- Osteomalacia
- Rickets
- Preventing corticosteroid-induced osteoporosis
- Osteoporosis
- URTI
- Prevention of heart failure in elderly who have inadequate Vit D levels (not useful for treatment of HF)
- Often recommended in the elderly
- <<NOTE: to go from IU to mcg: divide by 40; To go from mcg to IU: multiply by 40<<
- %%Vitamin K%%
- 2 compounds:
- Vitamin K1 (phytomenadione) - plants, green vegetables, kiwi
- Vitamin K2 (menaquinone) - synthesized by intestinal bacteria
- Physiological function
- Coenzyme for Vit K dependent carboxylase - an enzyme required for synthesis of proteins involved in:
- helping to bind calcium to form bone (calcification) and decreasing bone turnover
- blood clotting (needed to produce prothrombin)
- Deficiency and toxicity
- Both very rare
- Deficiency:
- Results in hypoprothrombinemia, leading to an increased tendency to hemorrhage
- Low bone density (but long term effects on bone health are unknown)
- In ^^newborns^^ → all get a Vit K injection
- Toxicity:
- No adverse effects seen with high intake (no UL needed)
- Therapeutic uses
- To overcome excess effects of the coumarin oral anti-coagulants
- To prevent hemorrhagic disease in newborns
- Bruising - but no evidence for treatment/prevention
- Osteoporosis:
- Findings are mixed with both K1 + K2: some show improved BMD and fracture reduction, other’s don’t
- Some evidence that a high dietary intake of K1 improves BMD in women (not men)
- Drug interaction: Vit K antagonists (e.g. Warfarin) - pts need to eat consistent diet (same amount of Vit K day-to-day)
- 2 compounds:
- %%Calcium%%
- ]]List 2 major sources from which each vitamin can be obtained.]]
- ]]Discuss the clinical implications of the AREDs studies.]]
- %%Age-related Macular Degeneration (AMD)%% is the leading cause of vision loss
- Characterized by:
- Reduced central vision (not peripheral like glaucoma)
- Reduced visual discrimination
- Altered ability to read, drive, recognize faces, etc.
- ^^Age-related Eye Disease Study (AREDs)^^
- Interventions (4 arms):
- Anti-oxidants (vitamin C, vitamin E, beta-carotene) alone
- Anti-oxidants + Zn + Copper
- Zn + copper alone
- Placebo
- Only effective for intermediate to advanced AMD
- AREDS 2
- Removed the beta-carotene; added 2 other carotenoids (lutein, zeaxanthin); lowered dose of zinc (diarrhea); added Omega-3 fatty acids; only studied people with intermediate or advanced AMD
- No benefit adding Omega-3; adding lutein/zeaxanthin gave slight benefit (and beneficial to prevent harm in former smokers); lowering dose of Zn produced no change in efficacy
- BOTTOM LINE:
- taking AREDS or AREDS 2 supplements ^^reduces the risk of progression^^ from intermediate to advanced AMD by about ^^25%^^
- Do not prevent AMD onset
- Do not have an effect on cataract
- Omega-3 → no effect on cataract or AMD
- Current + former ^^smokers^^ should take the ^^AREDS2^^ formula and avoid the AREDS formula (increased lung cancer risk with beta-carotene)