OB Exam 1 SG.docx
\
- Describe the stages from an egg in the ovary to implantation, including names of the cells as it grows.
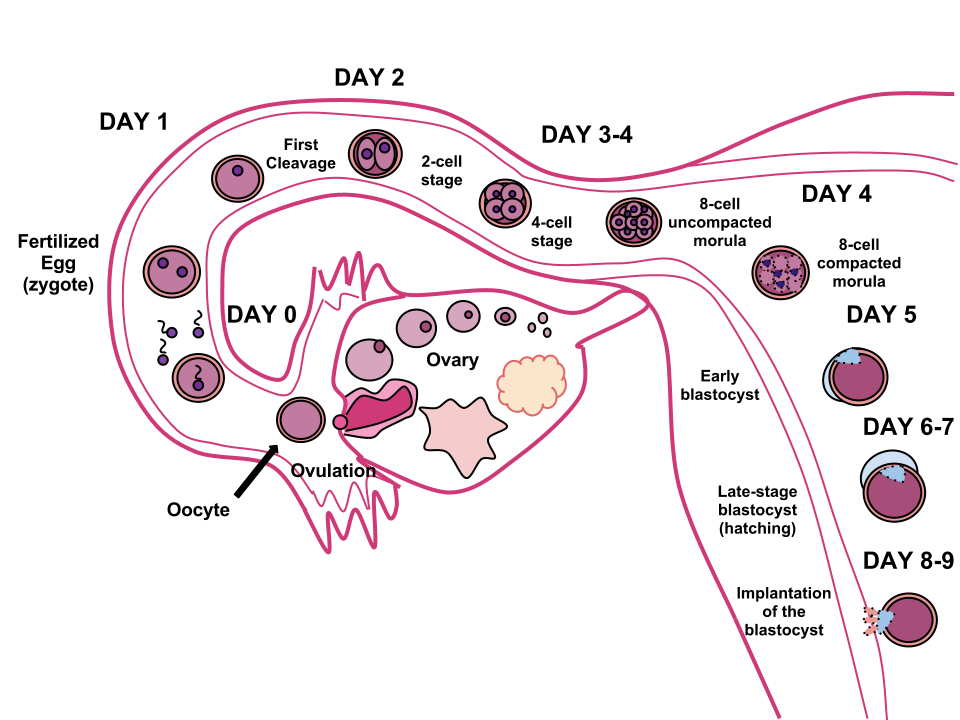
- 1. Oogenesis (the process of ovum formation) begins during fetal life and takes place in the ovaries → meiosis occurs in the female in the ovarian follicles & produces an egg each month during ovulation & the egg is surrounded by 2 layers: zona pellucida (inner, thick layer) & corona radiata (outer layer)
- 2. Fertilization → takes place in the ampulla (outer third) of the fallopian tube…this is where the sperm penetrates the outer membrane of the ovum & they are now enclosed in the membranes
- 3. Conception → the formation of a zygote (the 1st cell of the new unique individual)
- 4. Day 1 → first cleavage (1 cell → 2 cells)
- 5. Day 2 → cleavage again (2 cells → 4 cells)
- 6. Day 3-4 → cleaved into an 8 cell & 16 cell morula - a solid ball of cells
- 7. Day 5 → morula separates into 2 parts: trophoblast (give rise to placenta) & embryoblast (give rise to embryo); a cavity forms within the mass forming a blastocyst cavity (early blastocyst)
- 8. Day 6-7 → blastocyst forms when the cavity becomes recognizable
- 9. Day 8-9 → Implantation of blasyocyst into endometrium; endometrial blood vessels erode, which can casue the implantation bleeding & chorionic villi develop out of the trophoblasts & extend into the vascular system
- During what time in fetal development is the fetus the most vulnerable?
- “the first 3 months of pregnancy are recognized as the most critical period for emnyronic & fetal development” (pg 247) * this is when all of the main organ systems, external structures, and rapid cell division is occuring
- teratogens have the greatest effect during days 15-60 (p247)
- Review the anatomy of the placenta and cord. Make a rough drawing of how blood moves between the mother and fetus.
- 2 artieries & 1 vein * arteries carry deoxygenated blood & waste products from fetus * vein carries oxygenated blood & provides O2 & nutrients to fetus
- What is the EDD by Naegles’ rule with an LMP of 5/5/2022?
- Naegele's rule: LMP -3 months + 1 year +7 days * 5/5/2022=2/12/2023
- her power point says this instead… LMP - 3mo + 10days +1 year * 2/15/2023
- What is an appropriate fetal heart rate baseline range?
- The baseline FHR is the average rate during a 10 min segment that excludes periodic or episodic changes, periods of marked variability, & segments of the baseline that differs by more than 25 bpm (p364 ch 18)
- Normal FHR range is 110-160 bpm
- Describe the difference between preeclampsia and eclampsia.
- preeclampsia: * usually occurs after 20 weeks of pregnancy, typically in the 3rd trimester. when it occurs before 32 weeks of pregnancy, it is called early-onset preeclampsia. It can also occur in the postpartum period. * HTN, presence or absence of proteinuria, thrombocytopenia, renal insufficiency, impaired liver function, pulmonary edema, or cerebral/visual symptoms * placenta is the root cause, so this usually resides after delivery of placenta * management: * mild preeclampsia: bed rest; daily BP monitoring (q4-6h); more prenatal visits; fetal movement counts; 48-64 oz water; IV magnesium sulfate during labor; betamethasone (to promote development of fetal lungs) in women <34 weeks gestation * severe preeclampsia: hospitalization necessary…treatment is aggressive, quiet dark environment, sedatives, seizure precautions; BP control & monitoring; prenatal aspirin; betamethasone; IV magnesium sulfate prophylaxis; preparation for birth; during labor- IV mag sulfate, anti-HTN, & oxytocin, & watch closely for mg sulfate toxicity
- eclampsia: * seizure occurring in pregnancy & linked to high BP * Seizures typically begin with twitching around mouth. Body then becomes rigid in a state of tonic muscular contractions that last 15-20 seconds. Facial muscles & all body muscle contract & relax in rapid succession. Respiration ceases during seizure bc diaphragm tends to remain fixed (breathing rsumes shortly after seizure). Postictal sleep occurs. * requires immediate care: medical emergency to prevent mortality of mother & fetus; seizure interventions (ABC – airway suctioned & administer O2); monitor FHR; monitor for uterine contraction; IV mag sulfate, anti-HTN; betamethasone; birth via c-section or induced after seizures are controlled * Remember, magnesium sulfate acts like a depressant! Theraputic range is 4-7 mg/dL * toxicity: RR <12, Dec DTR’s, UOP <30ml/hr (Mg is excreted in urine, so dec UOP means inc mg levels), EKG changes….antidote is calcium gluconate
- Describe the difference between chronic hypertension and gestational hypertension.
- chronic HTN: * HTN that is present & observable before pregnancy (p585 ch 27)
- gestational HTN: * BP elevation that 1st occurs in the 2nd half (after 20 weeks) of pregnancy. Although this usually resolves after childbirth, it may increase the risk of developing HTN in the future
- What is HELLP syndrome?
- a laboratory diagnosis for a variant of preeclampsia that involves the hepaitc dysfunction characteristics below. These women may not have s/s of preeclampsia. A diagnosis is associated with an increased risk for maternal death & adverse perinatal outcomes (pulmonary edema, AKI, DIC, placental abruption, liver hemorrhage, ARDS, sepsis, stroke) * H – hemolysis * E & L – elevated liver enzymes * L & P -- low platelet
- aggressive treatment needed…same as that for severe preclamsia
- What can pass across the placenta from the mother to the fetus?
- O2, CO2, carbs, proteins, calcium, iron, water, inorganic salts, fats, vitamins, glucose, amino acids
- metabolic waste products of the fetus
- many viruses & some bacteria or protozoa
- majoirty of medications
- caffeine, alcohol, nicotine, carbon monoxide, other toxic substances in cigarette smoke, & prescription & recreational medications
List known teratogens.
- box 12.1 for chemical teratogens (off to right)
- box 12.2 for infectious diseases with teratogen effects (below)
- What is hyperemesis gravidarum?
- Excessive vomiting that begins before 9 weeks gestation, peaks 8-12 weeks, and extens beyond 1st trimester
- leads to weight loss, electrolyte imbalance, nutritional deficiencies, dehydration & ketonuria
- interventions: * initiate measures to manage n/v, including medications; may need TPN or IV fluid replacements; monitor VS, I&O, weight, calorie count, ketones in urine, FHR; encourage small portions of food & fluids
What physical assessment findings can be present in preterm labor?
- preterm birth → reaches 20 weeks but ends before 37 weeks
- uterine contractions, dull backache, menstrual-like cramps
- When is a pregnancy considered full term?
- b/t 37-42 weeks
- Describe the screening process for gestational diabetes.
- performed between 24-28 weeks, but high risk factors will be screened earlier
- 2 step screening: * 50 g oral glucose with plasma glucose measurement 1 hour later – level of 130-140 is considered a positive screen & requires step 2 – a 3 hour oral glucsoe tolerance test (OGTT) on another day * OGTT – 3 days unrestricted diet, 12 hours no smoking, no caffeine – 100 g glucose & blood glucose 1, 2, & 3 hours later * \ * if 2 or more checks are met or exceeded
- How much fluid should a pregnant patient ingest daily?
- 8-10 glassess (2.3L / 2,300 mL) of water
- What increase in calories are recommended in the 2nd and 3rd trimester?
- 2nd → 2,200 calories/day 3rd → 2,400 calories/day (p 300)
- How can gestational diabetes affect the mother and fetus?
- mom → Preeclampsia, c section, and development of type 2 diabetes later
- fetus → More at risk for macrosomia and associated risks for trauma and electrolyte imbalances (hypoglycemia and hyperinsulinemia) & congenital defects
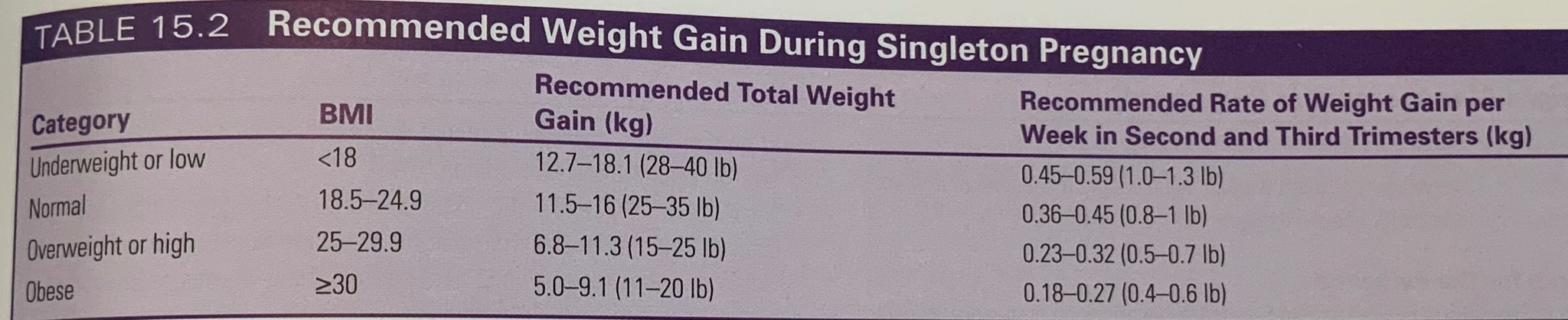
- Describe weight gain recommendations based on BMI ranges and by trimester.
- Describe pelvic inflammatory disease.
- causes: most cases it is more than 1 organism…most commonly gonorrhea or chlamydia
- s/s: * pain (usually abdominal) * 1 or more of the following: fever, chills, N/V, inc vaginal discharge, s/s of UTI, & irregular bleeding
- Dx: no 1 test – a combo of med history, s/s, pelvic exam, blood & urine tests, ultrasound
- Tx: broad spectrum antibiotics & analgesics
- What labs should be done at a first OB visit?
- urine, cervical, & blood samples are routinley obtained during the intial visit for a variety of recommended screening & diagnostic tests for infectious diseases & metabolic
conditions that can affect mom and/or baby (table 14.1 below) * urine tests for protein, glucose, leukocytes.
- PAP smear
- HIV test and education
- syphilis, hep B, chlamydia, gonorrhea, if high risk, repeat at 3rd trimester.
- TB test.
- Describe the cardiovascular changes in pregnancy.
- blood volume (by 40% - 50%, plasma, total RBCs volume increases
- anemia occurs as plasma increase exceeds the increase in production of RBCs
- iron requirements increases
- heart size increases, & is elevated slightly upward & to the left bc of displacement of diaphragm from uterus
- HR may increase about 10-15 bpm, BP slightly decreases in 2nd tri & increases in 3rd tri (but not above prepregnancy BP)
- What are the 2 most common surgeries in pregnancy?
- removal of appendix (appendectomy) & gallbladder (cholecystectomy)
- What considerations should be given for a pregnant patient with a vegetarian diet?
- All pregnant women who consume vegan/vegetarian diets should be referred to a dietician for nutritional counseling
- Daily consumption of a variety of different plant proteins—grains, dried beans and peas, nuts, and seeds—can provide all of the essential amino acids
- If well planned, can be nutritionally adequate for pregnant and lactating women
- Describe fetal kick counts.
- Also called daily fetal movement count (DMFC) * it is frequently used to monitor the fetus in pregnancies complicated by conditions that may affect fetal oxygenation
- during third trimester, the fetus makes about 30 gross movenents each hour. The mother is able to recognize 70-80% of these movements
- What is an ectopic pregnancy? Why can this be an emergency?
- the fertilized ovum is implanted outside the uterine cavity
- leading cause of infertility
- ectopic pregnancies are often called tubal pregnancies bc at least 90% are located in the uterine tube * less common areas can also occur in the abdominal cavity, on an ovary, on the cervix, or on a previous cesarean scar
- most cases of ectopic pregnancy are diagnosed before rupture based on the 3 most classic symptoms: 1. abdominal pain 2. delayed menses & 3. abnormal vaginal bleeding (spotting) * if it is not diagnosed until after rupture, referred shoulder pain may be present in addition to generalized, one-sided, or deep lower quadrant acute abdominal pain
- this can be an emergency bc if it bursts, it can cause severe bleeding and/or infection
- What is HCG? How do we expect HCG to change during pregnancy?
- HCG is the human chorionic gonadotropic hormone it can be detected in the maternal serum for 8-10 days after conception
- HCG reaches its maximum level at 60-70 days then decreases to lowest levels at approximately 100-130 days as the placenta becomes the primary source of estrogen and progesterone
- What are Braxton-hicks contractions?
- Painless contractions that occur intermittently after the first trimester, appear to enhance movement of blood through the intervillous spaces, aiding placental circulation
- What is a contraction stress test? What outcome is desired?
- Also called oxytocin challenge * A test done to stimulate uterine contractions for the purpose of assessing fetal response to stress, it identifies a stable fetus that is stable at rest but shows evidence of compromise after stress
- A negative CST indicates no late decelerations observed with the contractions
- Provide patient education related to pap smear screening.
- Women should receive routine checkups for cervical and vaginal cancer
- women aged 21-65 should be screened every 3 years or for women ages 30 through 65 every 5 years
- Women may choose to stop screening after age 65 after 3 negative tests and no risks and after total hysterectomy for benign disease
- What three parts of the fetal circulatory system change after birth?
- Ductus arteriosus
- ductus venosus
- foramen ovale
- Why should women not lay flat on their backs after 20 weeks of gestation?
- the weight of the baby/placenta can compress the descending vena cava
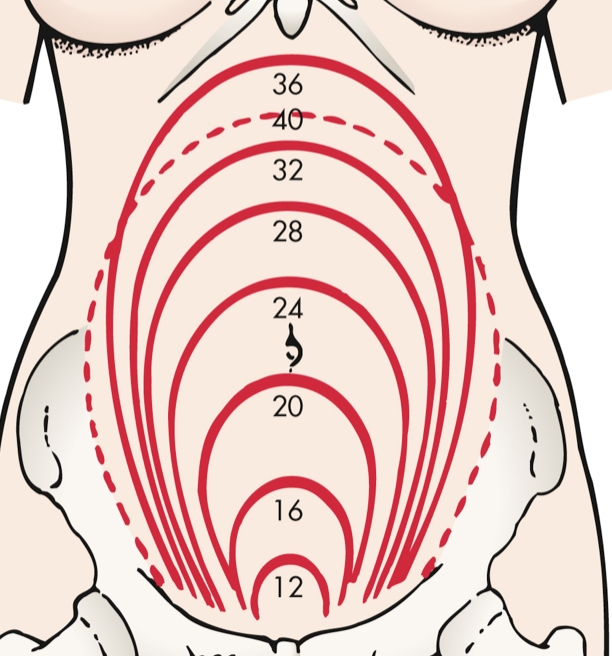
- What fundal height measurement would you expect at 12 weeks? 20 weeks? 36 weeks?
- 12 weeks → pubic symphysis
- 20 weeks → umbilicus (belly button)
- 36 weeks → diaphragm
- Describe MSAFP and NIPT screenings.
- maternal serum 𝛂-fetoprotein * 𝛂-fetoprotein levels are used as a screening tool for neural tube defects (NTDs) in pregnancy * screening is recommended for all pregnant women * can be performed b/t 15 & 20 weeks, with 16-18 weeks being ideal
- NIPT – noninvasive prenatal testing * noninvasive test to tell whether or not fetus has a genetic condition
- What is the difference between amniocentesis and CVS?
- amniocentesis → performed to obtain amniotic fluid, which contains fetal cells * possible after week 14 * used for genetic concerns, assessing fetal lung maturity, and identification and follow-up of fetal hemolytic disease
- CVS (chorionic villus sampling) → earlier diagnosis & rapid results * a technique for genetic studies in the 1st trimester * indications are similar to those for amniocentesis, although CVS cannot be used for maternal serum marker screening bc no fluid is obtained
- Discuss non-hormonal contraception options including patient education on use.
- Transcervical sterilization: internal sterilization method that uses polyester fibers in a metal coil to stimulate scar tissue to occlude fallopian tube. * Good for obese women. * May take 3 months to fully occlude. * No longer made…
- Copper IUD, condoms, sterilization, abstinence, diapragm, sponge, spermicide, cervical cap, withdrawal, fertility awareness
- Non-hormonal IUD
- Paragard, made of copper. Doesn’t affect periods. Works up to 12 years. * causes increased menstrual cramping and pain * 99.2-99.9 effective
- Condoms.
- Can break. May be an allergen. Oil-based lubricants break condoms. Use condoms with a point at the end
- protects against STIs; 87% effective
- Sterilization (male or female): 99% effective.
- Vasectomy: need to have 2 negative sperm samples after, usually less invasive and recovery is faster.
- “Tying the tubes”: cutting out a section of the tube and cauterizing both ends.
- Internal Condom “female condom”
- as effective as a regular condom theoretically, but can move around more. breaks down with oil-based lubricant. never use it at the same time as a male condom!!
- Sponge
- a round piece of plastic foam with a little dimple on 1 side & a nylon loop across the top that looks like a shoelace material…insert up into vagina before sex. blocks cervix to keep sperm from getting into your uterus, & it continuously releases spermicide
- 73-86%; usually no side effects
- Diaphragm / cervical cap (very similar, but diaphragm is better option)
- Acts as a “hat” for the cervix to block any sperm from getting past the cervix. Put spermicide in it & around the ring as well ;more effective with someone who hasn’t given birth. go in before sex and keep in 6 hours after sex (no more than 24 hours though). typical use effectiveness is 83%.
- Discuss hormonal contraception options. What are their contraindications?
- llllIUD, implant, shot, patch, pills, emergency contraception
- Hormonal IUD – Mirena, Skyla, LILETTA, and Kyleena
- All 4 are made of plastic and release a small amount of the synthetic hormone progestin, which thickens your cervical mucus to keep sperm from reaching the uterus. Good for 3-8 yrs. Can make your period lighter. 99% effective.
- side effects: increase blood flow or cramping
- Implant (Nexplanon)
- Under the arm, releases progestin to keep ovaries from releasing eggs and thickens your cervical mucus. Works up to 5 years. 99.9% effective.
- side effects: irregular bleeding is the most common
- Birth Control Shot (Depo)
- shot containing progestin, lasts for 3 months then you need another shot. When the shot is stopped, it can take a year for fertility to come back.
- calcium supplement if older pt
- 99% effective
- side effects: irregular bleeding & increased appertite, leading to weight gain
- Birth control pill
- Most work by releasing hormones that keep your ovaries from releasing eggs. The hormones also thicken your cervical mucus, which helps to block sperm from getting to the egg in the first place. Tyical use effectiveness ~ 93%. Common SEs are sore breasts, nausea, spotting, & decreased sex drive.
- Birth control patch – Xulane, Zafemy, Twirla
- The patch gives hormones thru your skin that prevents your ovaries from releasing eggs. They also thicken your cervical mucus, which helps to block sperm from getting to the egg in the first place. Typical use effectiveness 93%. If your BMI is more 25/30, it may be less effective.
- SE: nausea, irregular bleeding, sore boobs (usually temporary)
- Birth control ring – Annovera & NuvaRing
- small bendable ring inserted into your vagina. Leave it in for 3 weeks at a time & then take it out for the 4th week. The ring works by giving off hormones to prevent your ovaries from releasing eggs & thicken cervical mucus, which helps block sperm from getting to the egg in the 1st place. Typical use effectiveness 93%.
- SE: temporarily irregular bleeding, sore boobs, nausea
- Emergency contraception – “morning after pill; plan B”; Non-hormonal IUD, ella
- can stop a pregnancy before it starts (this means they are NOT the same as the abortion pill). they will work up to 5 days after unprotected sex, but use it sooner rather than later.
- SE: increased blood flow, cramping, N/V
1. What anticipatory guidance would you give for permanent sterilization procedures (tubal ligation and vasectomy)? * tubal ligation
1. (what to expect after)
1. You should expect no change in hormones and their influence. 2. Your menstrual period will be about the same as before the sterilization. 3. You may feel pain during ovulation. 4. The ovum disintegrates within the abdominal cavity. 5. It is highly unlikely that you will become pregnant. 6. You should not have a change in sexual functioning; you may enjoy sexual relations more because you will not be concerned about becoming pregnant. 7. Sterilization offers no protection against STIs; therefore you may need to use condoms 2. what to expect day of procedure:
1. NPO prior 2. preoperative sedation and local anesthetic 3. sensations of tugging but no pain 4. completed in 20 minutes 5. within days the scar is almost invisible * vasectomy:
1. To reduce swelling and relieve discomfort, ice packs are applied to the scrotum intermittently for a few hours after surgery 2. A scrotal support may be applied to decrease discomfort 3. Moderate inactivity for approximately 2 days is advisable because of local scrotal tenderness 4. The skin suture can be removed 5 to 7 days after surgery 5. Sexual intercourse may be resumed as desired; however, sterility is not immediate
1. contraception needed until sperm count is 0 for two consecutive tests 6. no effect on potency of erection or amount of ejaculation 2. What is the difference in prenatal care that a midwife and physician can provide? * The midwifery model of care emphasizes the natural ability of women to experience pregnancy, labor, and birth with minimal intervention * reduced use of epidurals and fewer episiotomies and instrument-assisted births * Certified Nurse-Midwives: grad level nurses, care for women with low- and high-risk pregnancies; they practice collaboratively with physicians or independently with an arrangement for physician consultation based on the condition of the patient 3. Describe a biophysical profile (BPP). What is it and how is it scored? * noninvasive dynamic assessment of a fetus that is based on acute and chronic markers of fetal disease * includes AFV (amniotic fluid volume), FBMs (fetal breathing movements), fetal movements, and fetal tone determined by ultrasound and FHR reactivity determined by means of the NST * FHR reactivity, FBMs, fetal movement, and fetal tone reflect current CNS status, whereas the AFV demonstrates the adequacy of placental function over a longer period of time * usually in late 2nd tri to 3rd tri * only downside is that if the fetus is in a sleep state, it can end up being a long period of observation * Scoring:
1. 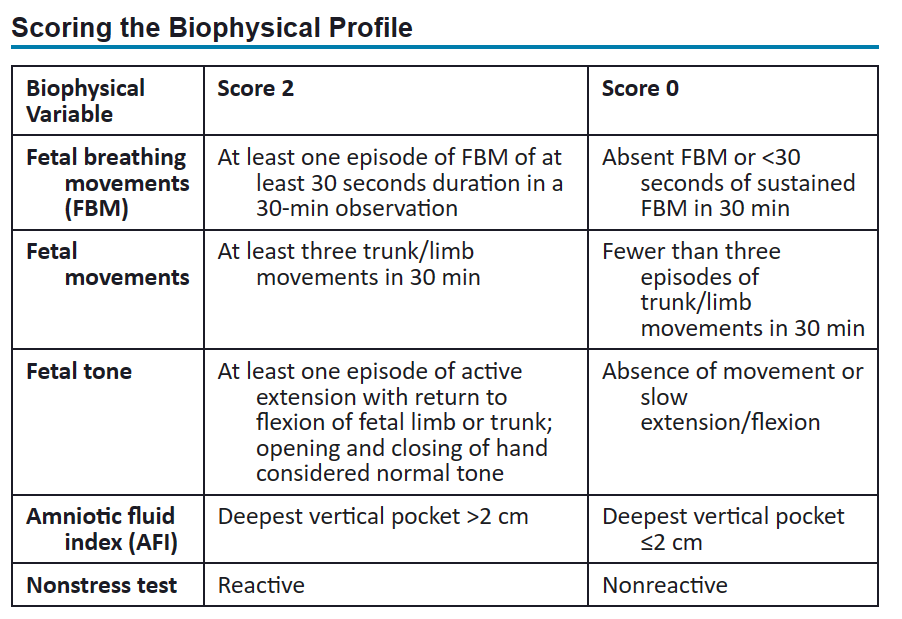
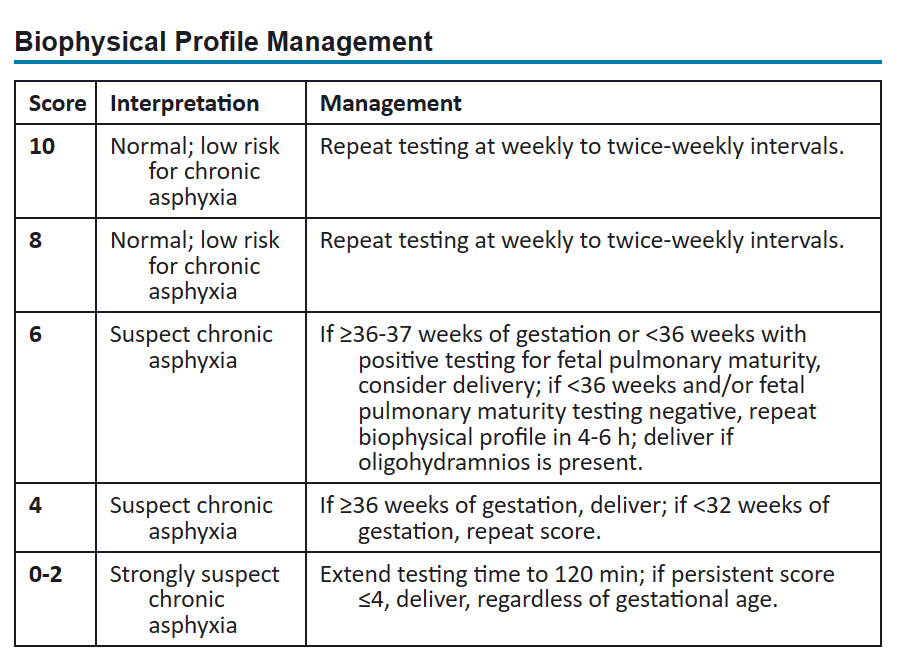
1. reactive: Two accelerations in a 20-min period, each lasting at least 15 seconds and peaking at least 15 beats/min above the baseline 15x15 rule 2. non-reactive: A test that does not demonstrate at least two qualifying accelerations within a 20-min window 5. What anticipatory guidance would you give for post abortion care? * clear instructions on when to return to to ED
1. fever greater than 100.4 or 38 c 2. chills 3. Bleeding greater than two saturated pads in 2 hours or heavy bleeding lasting a few days 4. Foul-smelling vaginal discharge 5. Severe abdominal pain, cramping, or backache 6. Abdominal tenderness (when pressure applied) * The woman may expect her menstrual period to resume 4 to 6 weeks from the day of the procedure * encourage counseling to deal with all of the emotions that come with this abortion * talk about contraceptive options * the woman usually will experience bleeding and cramping. Side effects of the medications include nausea, vomiting, diarrhea, headache, dizziness, fever, and chills 6. How should contraception patient education be modified for teens? * teens should be given all of the information/options to make an informed decision and should be encouraged to be safe without overly encouraging sexual activities * they should be educated on their risk of becoming pregnant on the different birth control methods and their risk of getting an STD 7. Describe the difference between accreta and placenta previa. * placenta accreta:
1. serious pregnancy condition that occurs when the placenta grows too deeply into the uterine wall 2. Typically, the placenta detaches from the uterine wall after childbirth. With placenta accreta, part or all of the placenta remains attached. This can cause severe blood loss after delivery. 3. usually no signs or symptoms other than bleeding in third trimester 4. may cause premature emergency c-section * placenta previa:
1. placenta completely or partially covers the opening of the uterus (cervix) 2. signs: bright red vaginal bleeding, usually without pain, after 20 weeks of pregnancy
1. The bleeding may also be triggered by sex or during a medical exam 8. What are the presumptive, probable, and positive signs of pregnancy? * Presumptive—subjective: changes experienced by the woman (e.g., fatigue, breast changes, quickening); these suggest the possibility of pregnancy but can also be caused by conditions other than pregnancy * Probable—objective: changes observed/perceived by an examiner (e.g., positive pregnancy test, Chadwick sign ( bluish discoloration of the cervix, vagina, and vulva), strongly suggest pregnancy * Positive—objective: changes observed/perceived by an examiner (e.g., fetal heart tones, ultrasound), indicate proof of pregnancy 9. What does GTPAL stand for? * Gravita: number of times an individual has conceived, including any current pregnancy * Term: This refers to the number of times an individual has carried a pregnancy to at least 37 weeks of gestation and delivered * Premature: Babies born between 20 and 36 weeks 6/7 days of gestation are all included in this section (different than parity Parity which is any delivery after 20 weeks of gestation, regardless of whether the child was born alive or stillborn) * Abortus: This refers to all times the individual has lost a pregnancy whether elective (i.e., medical or surgical) or spontaneous * Living: number of living children but refers to the number of live births an individual has had
- What is maternal PKU? * cause of cognitive impairment * Absence of the enzyme phenylalanine impairs the body’s ability to metabolize the amino acid phenylalanine found in all protein foods * toxic accumulation of phenylalanine in the blood occurs, which interferes with brain development and function * individuals with this disorder also have hypopigmentation of hair, eyes, and skin because phenylalanine inhibits melanin production * Currently, lifelong dietary restriction and therapy are recommended because they improve the quality of life for individuals with PKU * High maternal phenylalanine levels are associated with intellectual disability, microcephaly, seizures, growth impairment, and cardiac anomalies in their children * breast milk is high in protein, PKU babies get phenyl free formula * a mother who has PKU is ok to breastfeed as long as her baby does not have PKU
- \ * \
\