Alterations in Tissue
Anatomy
functions: against infection, UV, chem, injury, temp regulation, sensation, insensible fluid loss
produce vit d / excrete water, ammonia, urea
stratum
corneum
lucidum
granulosum
spinosum
basale
epidermal contains normal flora
→ Staphyloccoccus
epidermitis
aureas
cutibacterum acnes
dermis → sweat glans, hair/follicles, muscle, sensory, blood/ lymph
hypodermis → fat, connective tissue, follicles, sensory, vessels
5ht decade → thin
stages of healing
hemostasis/ inflammation
clotting cascade, vasoconstriction, fibrin mesh
vasodilation → hyperemia + edema
chemotactic + growth factors → healing
neutrophils → cytokines
proliferation: 3-10days → weeks
granulation
repair of vascular
→epithelialization + fibroblasts
tissue remodeling: 21 days → 1y
synthesis of new cells to degradation of tissue
collagen
wound edges are closer
apoptosis of fibroblast
no more angiogenesis → normal blood flow
risk factors for skin injury
inc age (<65y), physical limitations, poor nutrition, incontinence, poor circulation/ O2, decreased sensation, altered cognitions (aggresive) , polypharmacy(steroids), ADL dependent
inc physiological stress → surgery, trauma, illness, exarbation of chronic, emotional stress
healthcare system
skin irritations, pressure, friction, shearing of skin
Moisture:
inc susceptibility of shearing and friction → skin flora can enter
incontinence- associated dermatitis
skin folds are susceptible
intertrigo → inflammation of skin folds → maceration → infection w/ candida
Moisture-associated skin damage
Friction: superficial
mechanical force of dragging skin across surface
Shearing: deeper
interior body move in opposite directions = deep tissue injury
when body is pulled down or up
those with impacted mobilty →
skin tears: wounds due to mechanical forces
→ partial flop or total flop
conditions for wound healing
perfusion is necessary → if not = chronic wounds, non healing
proteins, COH, fats, Vit, growth factors
Proteins:
fuel for tissue repair
10% of lean mass loss= low immunity
lost in wound exudate
amino acids:
arginine: inflammatory process + collagen synthesis → GH + T-cells
glutamate: inflammatory + guard against wound infection
COH:
fuel
increase hormone and growth factor
Fats:
normal cell functions
precursor to prostaglandins → inflammation and metabolism
Vitamin:
A: fibroplasia, epithelialization
B: enzymatic
C: Collagen, antitoxin, angiogenesis
D : structural integrity + epithelial movement
E: negative effect in collagen
Minerals:
Zinc: immune
curcumin (turmeric) : inflammatory, proliferation, remodeling phases
conditions that impact wound healing
Vasoconstriction
causes → cold, alpha androgenic 1, beta antagonists, pain, fear, hypovolemia, nicotine
Medications: immunosuppress
corticosteroids
anti-inflammatory in first few days of injury
chemo
Conditions that affect perfusion:
PAD, radiation, excessive pressure
CVD: venous HTN
DM: poor infusion, neuropathy, low collagen, angiogenesis
impaired immunity
wound hypoxia w/ low angiogenesis + neovascularization
Tobacco, nicotine, epinephrine
inc CO2 + low immune
obesity:
oxidative stress → low perfusion + epithelization + infection
stress: inc cortisol, glucocorticoids, catecholamines → impair immune
wound conditions:
excessive exudate, hemorrhage, biofil, infection, slough, eschar
impact in overall health
scarring:
excessive wound healing → continuous wound inflammation
hypertrophic: excess collagen → organized and smooth → aligned w/ wound → can shrink
keloid scarring: expand beyond borders
→ associated w/ infection, tension, foreign body, trauma
hyperactive fibroblasts
chronic wounds: open for more than a month and do not go to normal wound healing
→ by metabolic disorders (DM/ obesity), vascular deficits, pressure in skin
diabetic foot ulcers → impacts blood flow → slow healing more infection → necrotic, amputation, sepsis
s/s: pain, diff sleeping, low function (low ADL)
→ tx = pain control (prior to any dressing changes)
also check psychological s/s since may impact wound healing
s/s
pain, warmth, red, bleeding, oozing
acute alterations from acute wounds
skin incisions
tears
abrasions
Moisture-associated skin damage
chronic wounds
arterial ulcer:
deep wound w/ punched out appearance
smooth, well- demarcated borders
may contain eschar
poor perfusion → pale, hairless, cool
venous:
shallow wound in medial area of LE + edema
no eschar
DM ulcer:
plantar of foot
callous
superficial → deep
wound classification: size, location, depth, and drainage
systematic cause: DM, malnutrition, connective tissue disease (RA)
Regional: neuropathy, arterial/ venous insufficiency, lympj
local: continued pressure, infection, and autoimmune
labs:
ABI
lower than 0.8 = PAD
Doppler
Acute infection s/s not present in chronic
→ biopsy = >100K = infection
→ use Levine tech
dx:
digital planimetry → epithelialization, necrotic tissue
ultrasonography, CT, MRI, SPECT, terahertz spectroscopy → wound tissue + bony structure
Lab:
CBC (anemia, WBC, platelet)
BMP, serum protein, pre/albumin, transferrin
bacterial protease activity (BPA) = detect pathogenic
excessive inflammatory protease activity (EPA) = identify unlikely healing wounds
→ further wound debridement is warranted
infection → CRP, procalcitonin, presepsin, microbial DNA
STONEES:
Size becoming larger
Temperature increasing
Os (bone exposed)
New breakdown
Erythema
Exudate
Smell
nursing role
Ensure proper equipment
pain meds before dressing change
affordability
assess tissue + cultural preferences
PPE + debriment equipment
wound, ostomy, continence nurses (WOCN)
education::
assess knowledge of condition, cultural, SDOH,
caregiver preference + barriers to learning
EBP, resources
implement and evaluate plan = teach back
assessment:
Clinical Judgment Measurement Model
look for wound not progressing
depth, width, length, describe bed and edges
undermining, tunneling
COCA
color, odor, consistency, amount
health hx + reasons (systematic, regional, local)
VS, incontinence
analyze:
PAD, DM, CV, edema, immobility
hypothesis
tx infections is priority → nutritional deficiency, (control BG, blood flow, Medications)
check protein lavels, pain management,,
take implementations:
abx, position change, control moisture, dietary education
types of dressing
if wound wet → remove wet
if dry → moisturize
tx:
diet:
protein, calorie count, accurate I&O
Rx:
analgesics, abx, wound dressing
common infections: staphylococcus aureus, coagulation-negative staphylococci, enterococci, Escherichia coli, and pseudomonas.
surgical management:
surgical debriment
large wounds w/ surgical closure or placement of skin graft
negative pressure wound therapy tx:
dressing, sealing w/ occlusive dressing and vacuum w/ -50 → -125mm Hg
electric stimulation: electrodes near wound → 150- 250 volts
hyperbaric O2: pressure chamber w/ ATM and 100% O2
→ improves circulation, O2, and lower edema
light adn phototherapy (PDT) : light doses → reduce bacteria, inc perfusion, inc ATP prduction
→ also works w. inflammatory conditions and cancerous lesions
lab/dx: Pressure injuries
Pressure, friction, shearing = bidirectional = bony prominence + hard surface place pressure on skin → blood flow is compromised
sacrum, hip, buttock, heel, back of head, shoulder, elbow
factors:
fragile skin
low blood flow, muscle
spinal cord injury
nutrient
moisture from incontinence
Braden Scale:
immobility and older age (low healing due to low perfusion/ protein/ tissue density)
stages:
nonblanchable red
partial thickness loss + ~ blisters, wound bed moist + pink
adipose tissue
check for undermining or tunneling
full thickness loss; fascia muscle, or bone
unstageable: full thickness extent to wound by slough or eschar
deep tissue injury: non/intact persistent nonblanchable deep red/maroon/ purple
~ blood-filled blister
nurse role:
safety check for fall hazards
wound specialists → use EBP
education:
mobilization and postion change
proper hygiene in skin folds and perineal
Braden Scale, head-to-toe assessment
size, shape, location, depth, drainage, undermining, or tunnelin, color, temperature, drainage, or odor of the wound.
infection → debridement → wound perfusion
interventions:
heels, elevate then, position q2h
airbeds, turn pt 30 degrees, lateral side-lying
protect sacrum with soft silicone multi-layered
HOB less than 30 + glide sheets
moisture control: pH cleaners, barrier cream, breathable incontinence pad
healing:
offload pressure from injury
nutrition management, infection prevention
photgraph wound
DIDN’T HEAL
DM
Infection
Drugs
Nutrition
Tissue Necrosis
Hypoxia
Excessive wound tension
Another wound
Low temperature in area of wound
tx:
NSAID, acetaminophen → morphine, oxycodone
superficial → topical abx
deeper → PO or IV abx
surgical management:
debridement: necrotic tissue, biofilm, infected material
cleaned after debridement
Common skin inflammation / infection
inflammation → WBC + inflammatory mediators = bradykinin + histamine
vasodilation causing red + warmth
all wounds have flora → infection when contaminated by skin normal flora or other
if multiplying but does not overwhelm immune system = colonization
local infection = colonization → challenge immune
→ surrounding tissues → systematic
inflammation:
Omega 3/6 protective against inflammatory infections
negative effect → smoking, alcohol, poor sleep, obesity
infections:
impacted by immune system, # of microbes, species, and combination, and location
Staphy. aureus + MRSA
Streptococcus, Group A = necrotizing fasciitis
risk factors:
gluten, low fiber, omega
smoke, drink, obesity
atopic dermatitis in children → if adults = its eyes
older adults →
pruritis, eczema, seborrheic dermatitis, and fungal
immunocompromised, steroids, malnutrition
Comorbidities:
gluten, DM, CV, infection, inflammatory skin, immune, SUD, connective tissue disorders
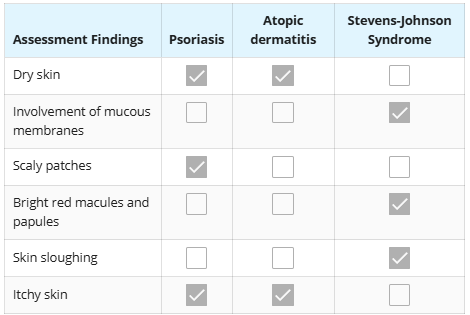
Inflammation disorders:
acne: when oil block hair follicle
allergic reactions: bright red macules / papules ~ blisters
SJS + toxic epidermal necrolysis → skin will slough off
atopic dermatitis: eczma
~genetic, immune, or environment
inflammation, redness, irritation
rash bubble up → fluid
scratching → bleed
contact dermatitis:
itchy, red, inflamed d,ue to contact
Herpes: cold sore/ shingle
painful sores → tingling, itching, burning
HSV 1/2
Infections: Athlete’s foot, cellulitis, warts
Psoriasis / Rosacea← overactive immune
dry, thick raised
scale/ plaque
scalp, elbow, knees
Urticaria (Hives) ← allergic response, stress, cold, unknown
patches of red bums
Bacteria infections:
cellulitis: redness, swell, pain, warmth ~ in LE
impetigo: red itchy sores → fluid = yellow crusty ~ in nose/mouth
Skin Staphy → red pimples, boils, painful, swollen, leak fluid
Fungi:
Athlete’s foot: dry skin, itching, burning, peeling, swelling, blistering
Yeast: mouth, throat, skin folds, vagina
cracks on corner of lips, white patch in tongue, itching in skin folds, vaginal itching, sore, drainage
Parasite:
Lice → itching, tiny bites
Scabies: itching, pimple like rash
Virus:
shingles: painful blistering rash → scab ~ 7-10 days
Wart appearance: raised bumps or flat
~ Herpes Simplex
Infection Continuum:
contamination
colonization
—- biofilm/ abx needed —-
local infection: topical
spreading infection: IV/ PO/ Topical
swelling of lymph nodes → malaise, anorexia
systematic
lab/dx:
by s/s
patch tests, blood, or bipsy
patch for contact dermatitis → 2-4 days → specific cause
CRP, presepsin, procalcitonin
Microbial DNA
role of nurse:
check if is contageous → standar abd PPE, and Contact precaustions (scabies, lice, impetigo)
education about contact in schools, daycare, communal living,
assess:
hx inflammation, experience with a similar skin condition; medications taken; or exposure to any chemical or irritant.
infections
check if anaphylaxis:
hives, GI upset, dizzy, tight throat, low BP, wheeze, high HR< impending doom, CV arrest
allergens:
nuts, fish, shell, milk, egg
latex
penicillin, ASA, NSAID, anesthesia
insect: bee, wasps, hornets, yellow jackets, fire ants
tx:
topical steroids for inflammatory
cool compress, not scratching, emollients/ lotion
anaphylaxis:
epinephrine, steroids, antihistamines
SAFE: Seek tx (911), Allergen idntify, Follow up wl specialist, Carry epinephrine
abx + s/s of infection
prioritize:
acute infection, anaphylaxis → severe rash, fever, mucous membreanes, skin breakdown
Rx:
inflammatory:
Steroids: hydrocortisone, prednisone, topical
antihistamines: diphenhydramine, cetirizine, loratadine, fexofenadine
reduces itching
Calcineurin inhibitor: pimecrolimus
pain: acetomenaphen + NSAID
Abx:
abx topical: bacitracin, neomycin, centamicin
abx oral: vancomycin, linezolid, doxycycline, clindamycin
abx IV: dalbavancin, oritavacin, tedizolid, delafloxacin
antifungal: fluconazole, ketoconizole
antiviral: acyclovir
Lece/ scabies: Rib/ Nix, Permethrin
Burns:
release cytokines → local and systemic reactions + histamine, prostaglandins → vasodilation
→ improves blood flow + O2
→ vascular permeability → exudate leak → edema
3 dimensional zones:
coagulation zone: protein coag + low blood flow = tissue loss
potential for skin loss but can be reversed w/ burn resuscitation
outermost → hyperemia from histamis → less damage
causes: flames, scald, electrical, chemical
increase metabolic + fluid demands (4days - 3yrs) → can loss lean mass → become malnurish
low fluid → organ failure + CV + AKI
K released, myoglobin → rhabdomyolysis + AKI
cause psychological stress
s/s:
epidermis → sunburn
epidermis + dermis
^^ → skin grafting
^^ + fat layer
muscle layers
bone
suoerficial → epidermis
superficial partial thickness → pink + blistering + wet
deep partial thickness: deep in dermis and white/ yellow, dry, nonblanchable
full thickness: damage to epi/ dermis, subq → white/ brown and leathery, nonblanchable
chemical acid: coag
alkali: deep penetration into skin → necrosis
electrical: small entry and exit wound but significant damage under skin
radiation: itching, red, edema → severe burn
thermal: depends
lab:
CBC: bleeding, anemia, WBC daily
BMP, albumin (fluid/ protein), BUN, Cr, GFR, ABG + carboxyhemoglobin
Coagulation: PT, INR, PTTM Thrombo, time, Xa, V, fibronogen
LFT
ionized calcium, albumin, Cr kinase
CXR, CT, PFT, bronchoscopy when resp is suspected
nutrition: Protein, carbohydrate, and fat needs should be met, glutamate, vitamin C, zinc, and selenium.
limited mobility: ROM exercises
sedation, edema, bulky, edema
perfusion ~ shock
aseptic and private room
if electrical → remove from scene
decontamination procedures
nursing:
assess:
body substance isolation (BSI): gloves, gowns, eye protection, and respiratory protection
hx of burn: type, location, length of exposure, other trauma
primary: AB (in chest, neck) CD(assess neuro) E (remove clothing, jew, lenses, assess temp to avoid making pt low T)
second:
hx of events/ health
Head-to-toe
depth, size, severity
check for inhalation injury, compartment syndorm, hypothermia
Rx may require ventilation, check fluid volume
burn center referral criteria:
>10%
face, hands, feet, genitalia perineum, or major joints
3rd
electrical, chemical
inhalation injury
preexisting conditions that could complicate + other traumatic injuries
severity of burn is reassess 48hr to 72hrs since may not reveal true extent
total body surface area:
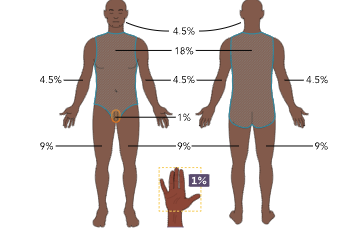
or Lund and Browder chart
for transfer:
→ safety, stabilize VS, ABC, fluid resuscitation, pain, large bore PIV
minor burn → cool burn w/ cool water for 3-5 minutes (no ice)
→ chem need more time
4C
Cool w/ tap water/ saline
clean w/ mild soap
cover w/ antimicrobial ointment + absorbent dress
comfort w/ OTC
older than 14y 500ml of LR/ hr
fluid formula: 2-4mL x kg xTBSA
urinary catheter when fluid resuscitation (0.5 mL/ kg/ hr) , NG tube, check edema/ compartment syndrome, HOB elevated at all times
schedule dressing changes, check for ROM
check for potential infection
tx:
diet:
daily weight/ lab: serum protein, albumin, pre-albumin, and glucose
PO/ enteral/ or IV
Rx:
opioid: morphine, fentanyl, hydrocodone, oxycodone
BZ:
topical abx: bacitracin, silvadene
silver sulfadiazine can be used but not in eye or pregnat
silver nitrate: abx but → tissue blackening and low Na
nanosilver, slowly release silver → less changes
Mafenide acetate → penetrate eschar (ADR metabolic acidosis)
debridement: necrotic tissue removed 48hrs after burn → antimicrobial dress, autograft, allograft, skin substitute
skin graft nonadherence → poor wound be preparation, shearing/ trauma, or infection
antimicrobial dress: Bacitracin, xeroform, and Silvadene (1-2 changes/day)
biologic dressing: apiary honey
autograft: unburned skin to burn
→ if large, no so cultured epithelial → grow
allograft: from donor to temporarily cover wound
skin substitutes → adhere to wound until epithelization occurs and allows exudate to leave
xenograft → porcine skin (animal)
escharotomy: remove eschar
fluid requirements: main choice crystalloid, nd somtimes colloids (albumin/plasma)
ABA: (TBSA x kg )/ 8 = mL/hr ( 40-80kg)
Rule of 10: al least 40kg, for every 10kg, increase over 80kg + 100mL/hr
TBSA x 10
TBSA (if client weighs less than 80 kg) x 10 (round to nearest 10) and multiply by 10 for the amount of fluid
Parkland: 2-4mL x kg xTBSA
1st half 8hr, next 16hrs
Goals:
0.5 mL/kg/hr;
base deficit less than 2 to normalize pH;
systolic blood pressure greater than 90;
no AMS
those w/ rhabdomyolysis or AKI = 1mL/kg/ hr
check HR + lactate
CO, SV, Systematic vascular resistance
Urine output, BP, HR