EKG!!
EKG
Why would an EKG be used?
detect arrhythmias
if coronary artery disease (narrowing/blockage) is causing chest pain or MI
whether you have had a previous heart attack
evaluating for need for a pacemaker/pacemaker functionality
signs & symptoms = chest pain, dizziness, confusion, syncope, palpitations, rapid pulse, SOB, weakness, fatigue
How does an EKG work?
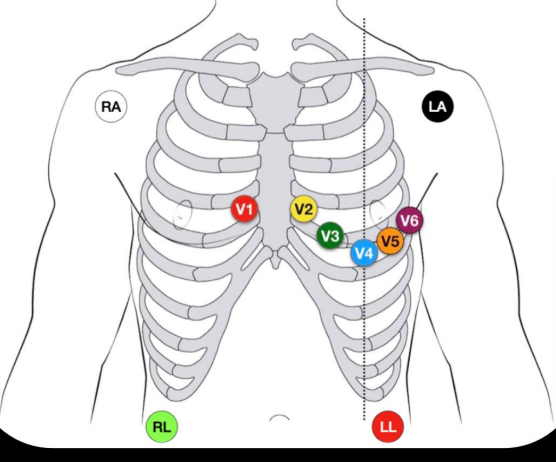
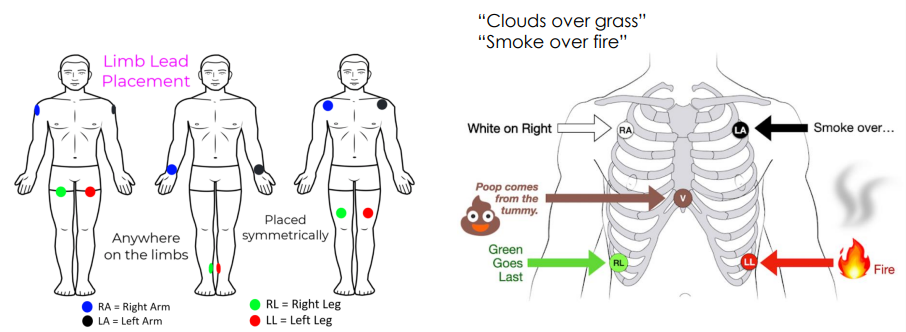
12 lead/full EKG = 12 electrodes attached to chest and limbs
only uses 10 electrodes, 4 are used for limb leads (same as monitor leads), 6 of these replace the v lead and are precordial leads
4 lead EKG = monitor patient during coronary angiogram/cardiac intervention
Defibrillation?
→ The administration of electric shocks to the heart in order to reset normal heart rhythm in persons who are experiencing cardiac arrest or whose heart function is endangered because of severe arrhythmia.
is the treatment for immediately life-threatening arrhythmias with which the patient does not have a pulse, ie ventricular fibrillation (VF) or ventricular tachycardia (VT)
Usually around 120 -360 joules are delivered (depending on the type of defibrillation).
Note = Hands-free pads are preferred over paddles due to their potential benefits and efficiency, they allow more rapid defibrillation as compared to defibrillation paddles, also they deliver more energy.
Heart Anatomy/Physiology
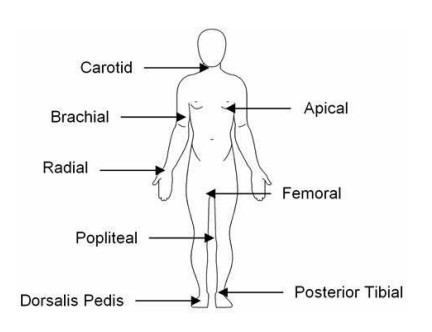
Pulses …
rhythm = regularity of heart beats → should be constant
irregular rhythm = arrhythmia can be determined by comparing apical pulse with a peripheral pulse, EKG can determine type
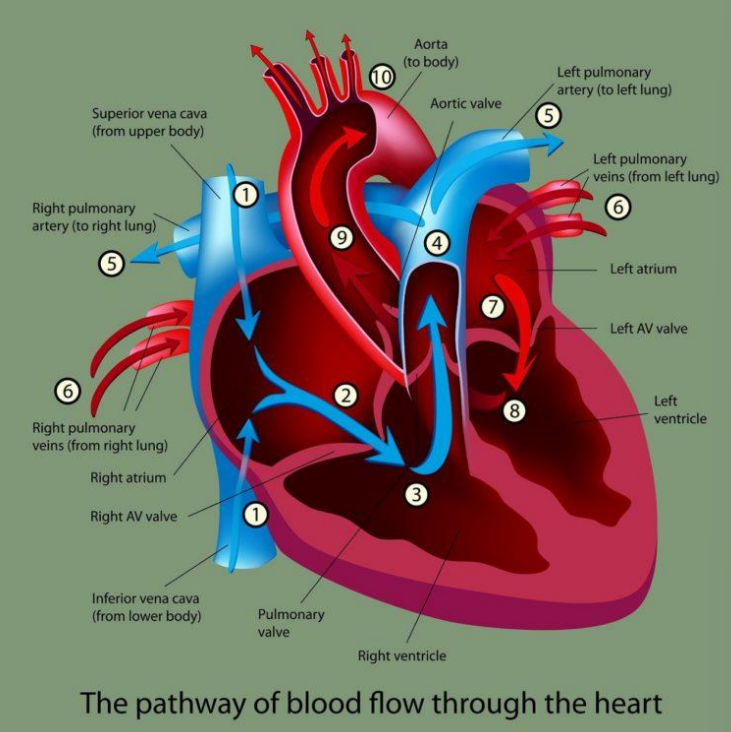
tricuspid = right atrioventricular valve
mitral = left atrioventricular valve
diastole = tricuspid and mitral valves open → blood flows into ventricles = ventricular filling phase
systole = contraction of ventricles AV valves closed → semilunar valves open which allows blood to be pumped into large vessels
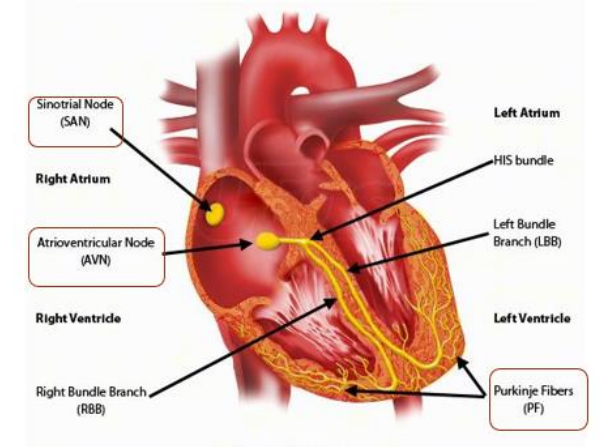
Cardiac Conduction System
SA sinoatrial node = natural pacemaker, initiates the electrical impulses that start each heartbeat, 60-100bpm
AV atrioventricular node = receives electrical impulse from the SA node and delays it slightly allowing atria enough time to eject blood into ventricles before they contract, 40-60bpm
Bundle of HIS = transmits electrical impulses from AV node to the ventricles, splits into left and right bundle branches, 20-40bpm. Slower rate because of its role to ensure that ventricles contract after the atria allowing for efficient blood flow through the heart.
left and right bundle branches = essentially just conduct impulses through the interventricular septum to the Purkinje fibers
Purkinje fibers = distribute the electricle impulses throughout the ventricles, causes them to contract and pump blood.
CARDIAC CYCLE
starts with atrial contraction ends with ventricular relaxation
Normal Sinus rhythm includes…
P wave | QRS wave | T wave |
|
|
|
NOTES!
diastole / relaxation / repolarization
systole / contraction / depolarization
ST segment = time between depolarization of ventricles and the repolarization of ventricles
PR segment = time between end of p wave and start of QRS - basically the small moment of break after the atria contract
PR interval = time between when atria starts to contract to when the ventricles start to contract
QT= time it tames for ventricles to fully contract then relax
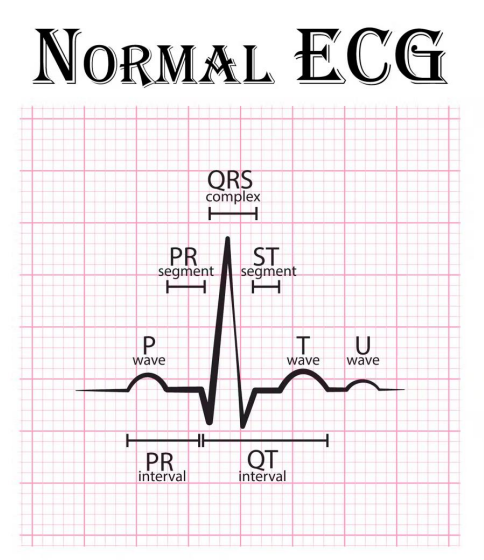
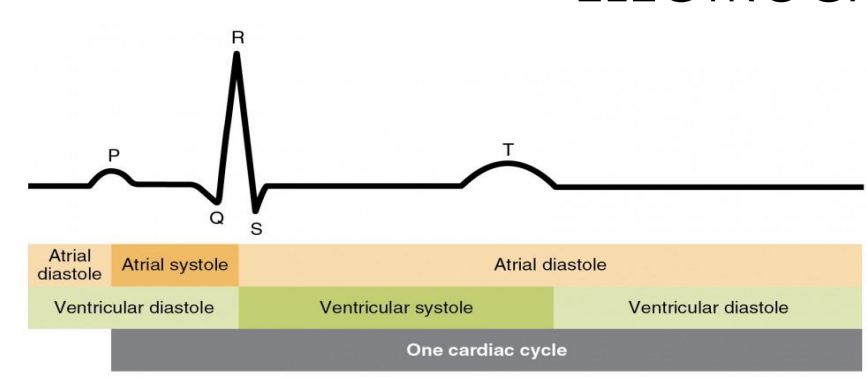
“Initially, both the atria and ventricles are relaxed (diastole). The P wave represents depolarization of the atria and is followed by atrial contraction (systole). Atrial systole extends until the QRS complex, at which point, the atrial relax. The QRS complex represents depolarization of the ventricles and is followed by ventricular contraction. The T wave represents the repolarization of the ventricles and marks the beginning of ventricular relaxation.”
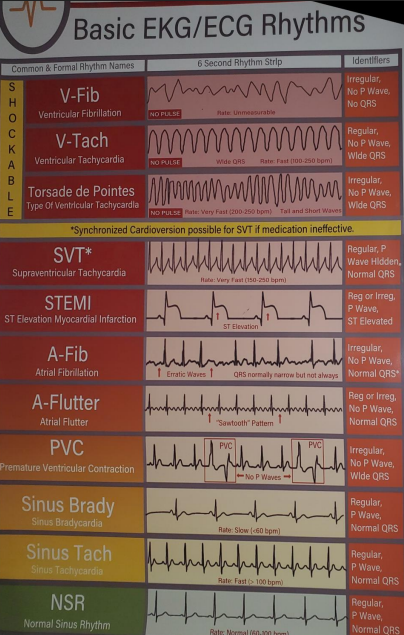
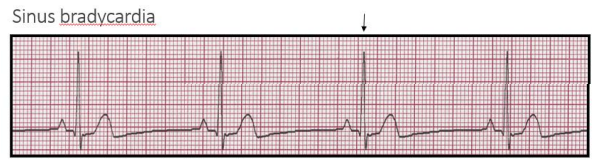
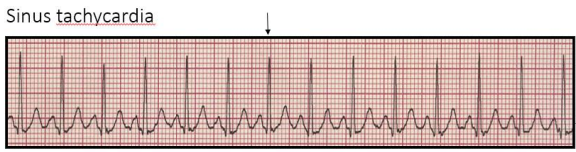
EKG rhythms!
Sinus bradycardia = normal slow, exercise (athletes), sleep, drugs
Sinus tachycardia = normal fast, exercise, anxiety, alcohol/caffeine, drugs
Common Supraventricular Arrhythmias (atrial)
Premature atrial contract PAC’s = extra heartbeats, may feel like a skipped beat or extra ones, usually does not require treatment (not shockable)
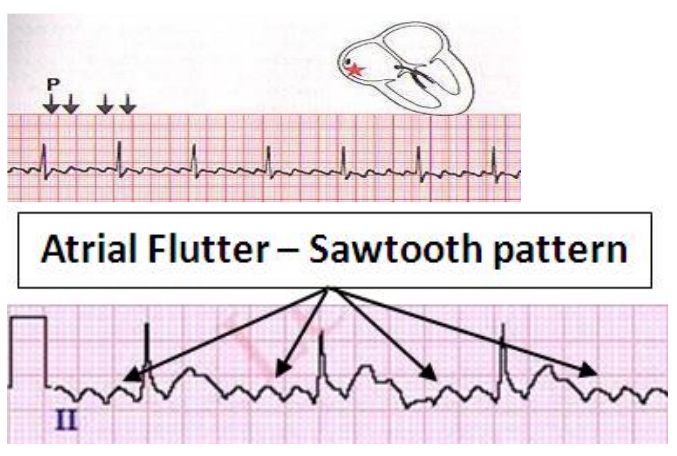
Atrial flutter
more regular and organized tha AFIB, it is a fast but regular rhythm.
rapid, regular or irregular atrial depolarizations
Sawtooth pattern, no P wave.
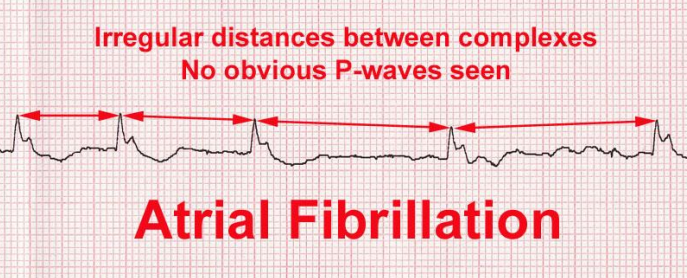
Atrial fibrillation AFIB - most common chronic arrhythmia
irregular, disorganized, very rapid heart rhythm, occurs in the upper chambers of the heart, can increase stroke risk
erratic atrial electrical activity with ventricular rates 120-200bpm
P wave is absent on the surface EKG and may be replaced with coarse fibrillatory waves, meaning atrial activity is sometimes unidentifiable
QRS complexes are irregularly irregular with varying R-R intervals
loss of atrial contraction

Ventricular arrhythmias
Premature ventricular contraction PVC’s = extra heartbeats, begin in one of the ventricles can disrupt the regular heart rhythm, may cause a sensation of fluttering, benign but may need treatment if frequent or if patient has underlying heart issues.
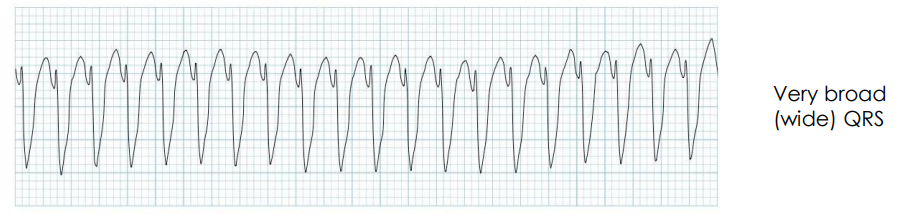
Ventricular tachycardia VTach = regular but rapid electrical signals in the lower chambers of the heart, requires CPR and defibrillation
The rapid rhythm keeps the heart from adequately filling with blood, and less blood is able to pump through the body
rate of 100bpm+
symptoms = palpitations, dizziness, chest pain, SOB
longer than 30 secs = requires intervention
Non-sustained VT: 3 or more activities of less than 30 sec
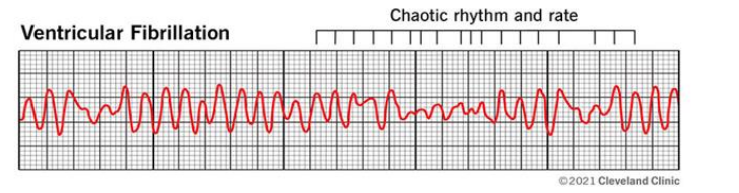
Ventricular fibrillation V-fib
erratic disorganized firing of impulses from the ventricles, thus cannot produce an effective contraction, unable to pump blood. requires CPR and defibrillation
most common cause of sudden cardiac death
signals basically cause the lower heart chambers (ventricles) to twitch (quiver) uselessly.
no P wave or QRS
Other rhythms
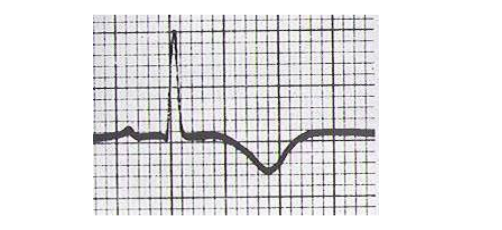
Ischemia
decreased → no flow to a region
T wave is reversed, can occur during angina
visualized 24-48hrs post MI
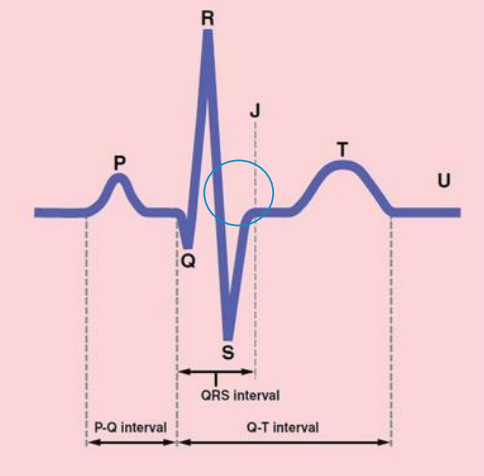
ST depression
Occurs when the J point (end of the S wave and beginning of the T) is displaced below baseline.
Ultrasound, Coronary angiogram and blood tests are vital to further evaluate these abnormal ECG waves.
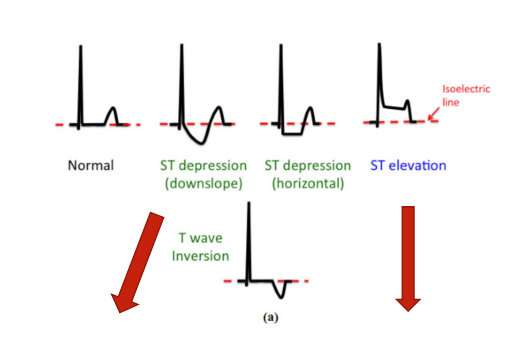

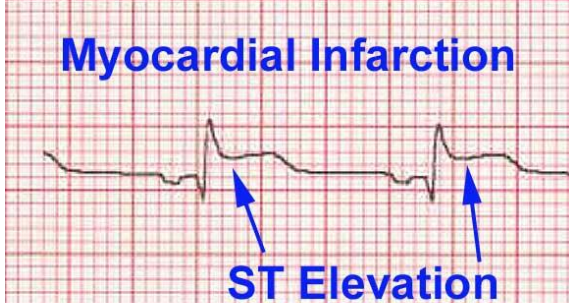
STEMI → ST elevation myocardial infarction
Occurs from occlusion of one or more of the coronary arteries that supply the heart with blood. immediate care necessary in the golden 90 min time slot for flow to be restored
tombstone sign

Asystole - FLATLINE
Asystole is NOT a shockable rhythm, and defibrillation may actually make it harder to restart the heart.
Defibrillation is only an option if your heart goes from asystole to a shockable rhythm, which is possible when someone with asystole receives effective CPR.
Represents the cessation of electrical and mechanical activity of the heart.
Carry on with CPR, Do not shock.