Week 5 - L2b Pathology of the Kidneys and UUT Part 2
Primary objectives include:
Identifying and describing common pathologies using sonographic imaging.
Differentiating various renal pathologies including Renal Cell Carcinoma (RCC), Transitional Cell Carcinoma (TCC), Lymphoma, Wilms Tumor, and Renal Metastases based on aetiology, clinical indications, and sonographic appearances.
Correlating laboratory values and specific clinical indications with renal anomalies and diseases.
Renal Cell Carcinoma (RCC)
Definition and Prevalence:
RCC is the most common of all renal neoplasms.
Accounts for approximately 85-95% of all renal cancers.
Demographics:
It is twice as common in men as in women.
Typically affects individuals over the age of 40.
Most commonly develops during the 6th or 7th decade of life.
Clinical Presentation:
Often non-specific in the early stages.
The classic clinical triad includes:
Haematuria (blood in the urine).
Flank pain.
A palpable mass.
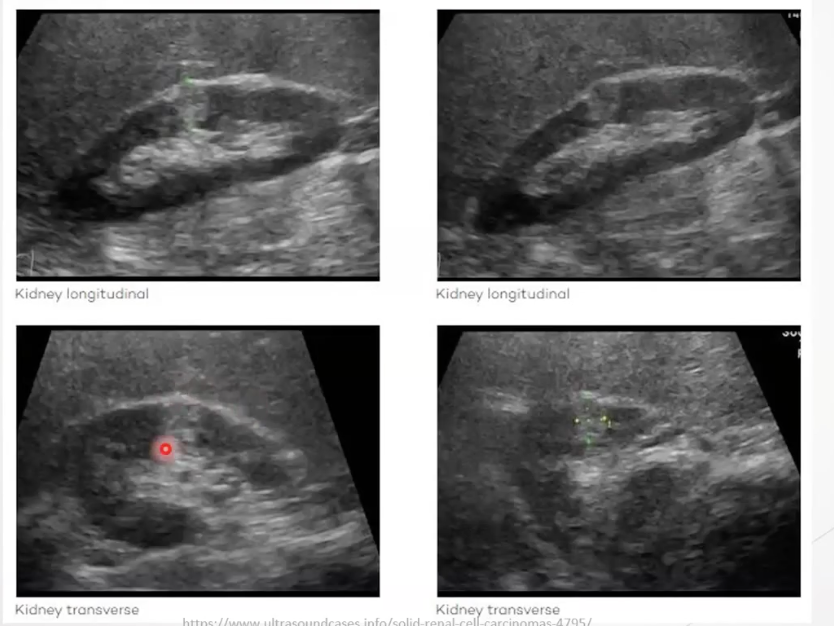
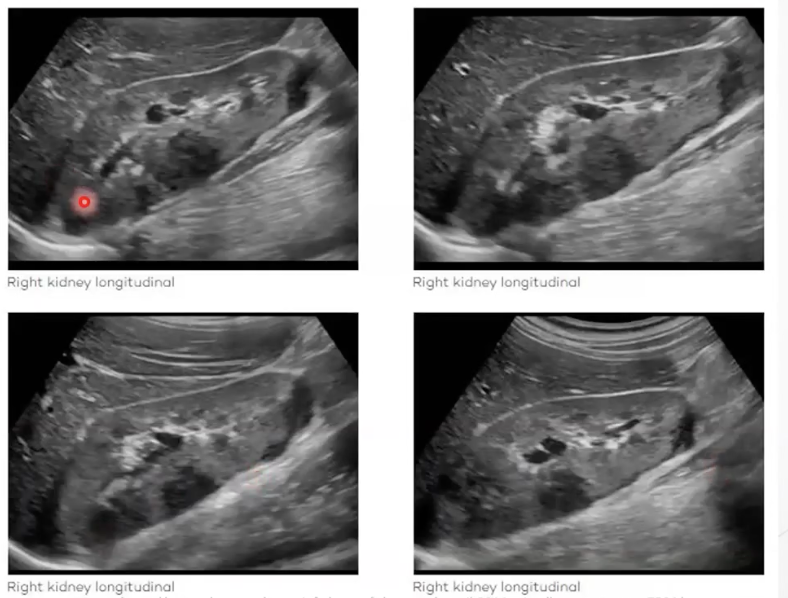
Sonographic Appearance:
Presentation is highly variable; it can mimic almost any renal condition.
Echogenicity:
Most often isoechoic, but can also be hyperechoic, hypoechoic or appear cystic (related to the Bosniak classification).
Small RCCs:
Often bulge the renal capsule.
Can appear more hyperechoic than the surrounding parenchyma, similar to adenomas or angiomyolipomas (AMLs), but typically feature "fuzzy" or less clean boundaries.
Large RCCs:
Appear as large, mid-level echoic, heterogeneous, and predominantly solid lesions.
Boundaries are often poorly defined within the renal cortex.
Infiltrative Nature:
Massive tumours may show no "mass effect" (displacing other structures) because they infiltrate through and take over the existing renal tissue rather than pushing it aside.
Vascularity:
RCCs are highly vascular.
Excess blood supply on color Doppler is a significant sign of a growing tumor.
Calcifications:
Some tumours contain microcalcifications.
Specific Subtypes and Mimics:
Clear Cell Carcinoma:
A subtype often confirmed via biopsy or surgical removal; it can look nearly identical to an angiomyolipoma with internal hemorrhage/bleeding.
Comparison with AML: RCC is often differentiated from AML by its lack of clear boundaries and its tendency to infiltrate surrounding tissue.
Spread and Seeding:
RCC spreads via the blood supply (vascular route).
Cancer cells enter the parenchyma (where arcuate and intralobular arteries are located) and seed into the renal veins.
From the renal vein, the cancer can spread into the Inferior Vena Cava (IVC) and then throughout the body.

Transitional Cell Carcinoma (TCC)
General Characteristics:
A rare type of kidney cancer compared to RCC, but very common in the bladder and lower urinary tract.
Can spread up the ureter or arise natively in the renal pelvis or the calyx.
Clinical Presentation:
Patients often present with back pain, hematuria, and frequent urination.
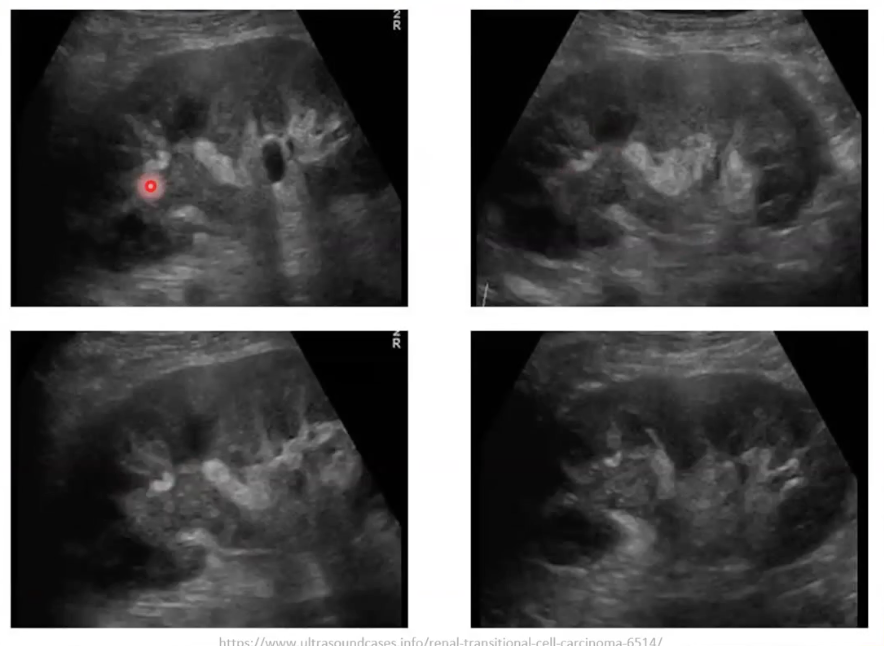
Sonographic Appearance:
Primary Feature:
A solid hypoechoic or mid-to-low level echo lesion originating within the renal pelvis or calyx (the collecting system).
Differentiation from RCC:
TCC is contained within the collecting system.
On ultrasound, one looks for the hyperechoic sinus fat surrounding the mass to confirm it is within the collecting system rather than the parenchyma.
Secondary Effects:
As the tumor grows, it can compress and thin the surrounding renal parenchyma.
Obstruction:
TCC can cause a "hold up" of urine in the pyramids, leading to dilatation (hydronephrosis) because the solid lesion blocks urine exit.
Colour Doppler:
Use of colour Doppler can show internal blood flow, which helps rule out a blood clot or thrombus (which would be avascular).
Spread Mechanism:
TCC spreads via the ureter (urinary route), not the vascular channels. It can migrate from the bladder up to the kidney or vice versa.
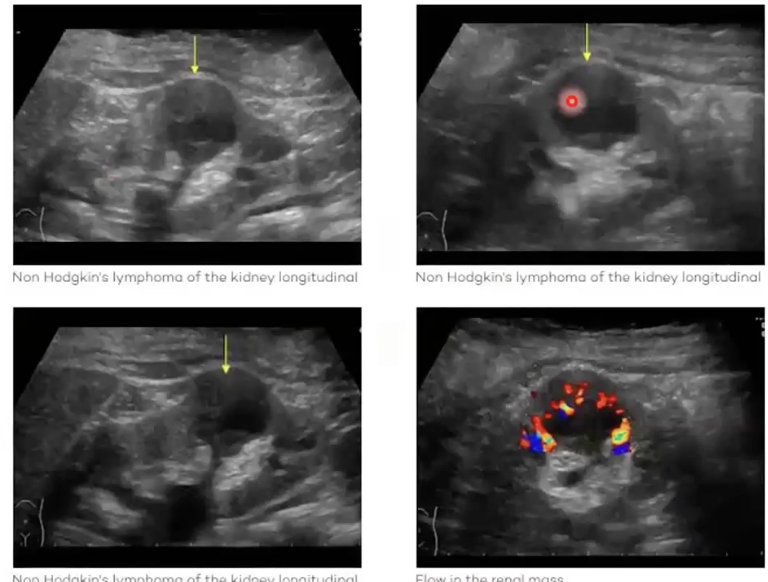
Renal Lymphoma
General Characteristics:
Primary lymphoma of the kidney is rare.
It is usually encountered as part of a multi-systemic spectrum of lymphoma.
Sonographic Appearance:
Presents as solid, hypoechoic lesions.
Often features multiple lesions throughout the kidney.
In complex or advanced cases, the images can look "mucky" and disorganised, destroying the normal renal architecture.
Can be easily mistaken for RCC on ultrasound; sonographers should list both in differential diagnoses.
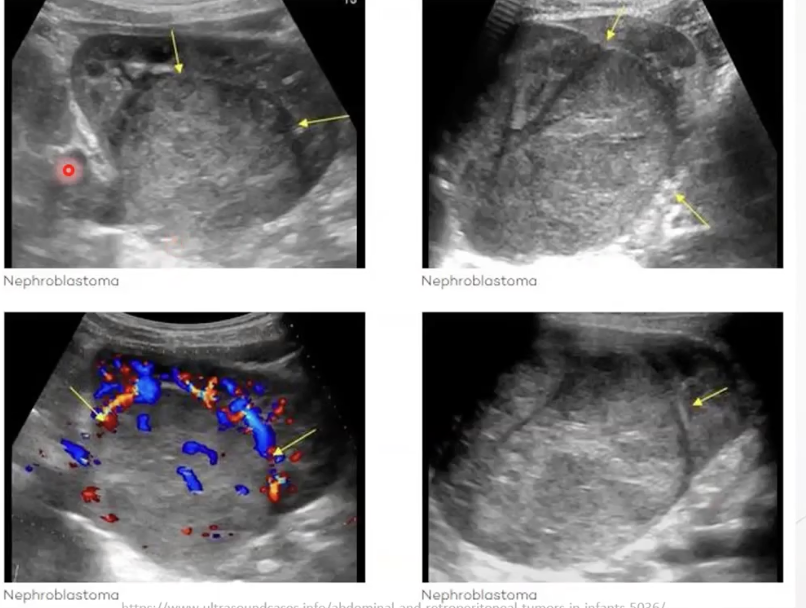
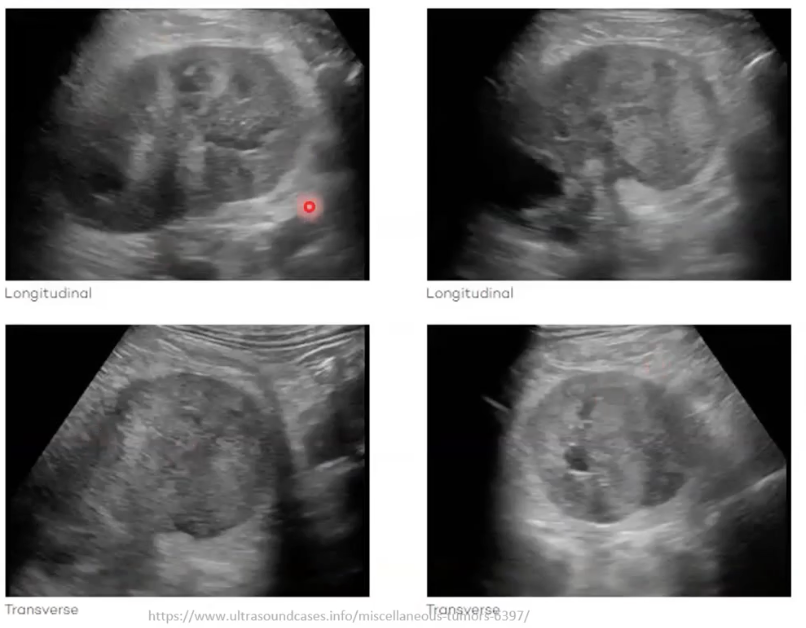
Wilms Tumor (Nephroblastoma)
Epidemiology:
The most common renal cancer in children.
Primarily affects children between the ages of 3 to 4
Instances are less common after the age of 5.
Occasionally seen in utero; rarely seen in adults.
Paediatric condition
Clinical Presentation:
Constipation, abdominal pain, nausea, and vomiting.
Abdominal swelling or discomfort.
Fever and loss of appetite.
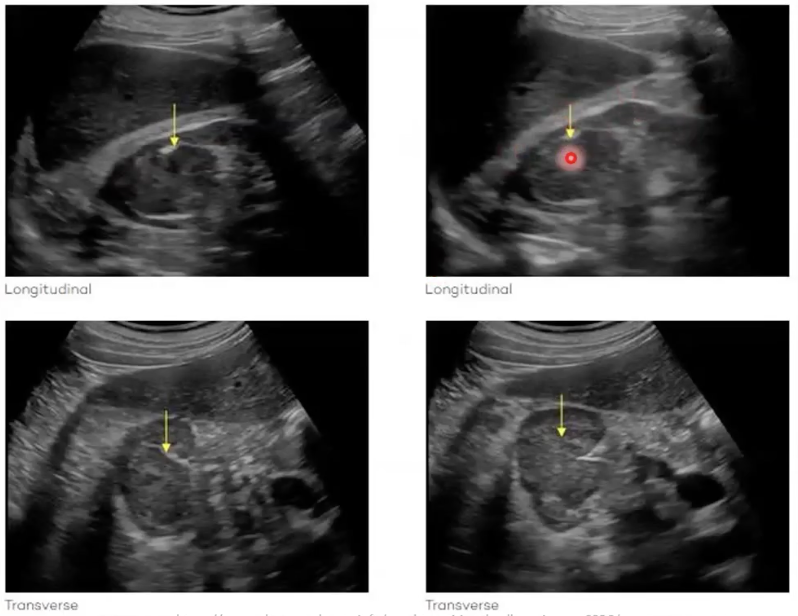
Sonographic Appearance:
Large, solitary, and predominantly solid masses.
Typically echogenic, though they may have cystic components or a multiloculated appearance.
They exhibit a significant mass effect due to their size.
Often invasive and poorly defined medially, making it difficult to identify normal kidney architecture or the origin of the tissue.
Colour Doppler:
May show both peripheral and internal blood flow.
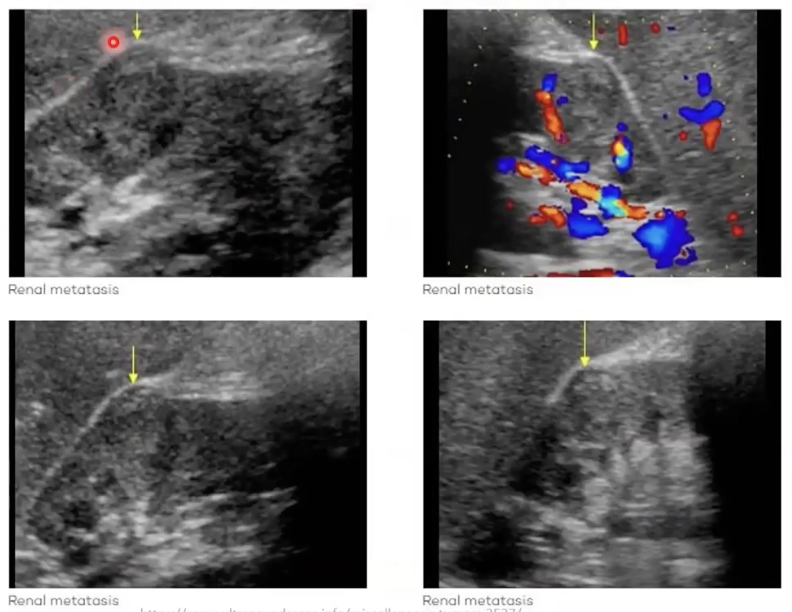
Renal Metastases
Primary Sources:
Most common primary cancers that metastasise to the kidneys include lung, colon, rectum, ENT (ear, nose, and throat), breast, soft tissue, and thyroid.
Clinical Presentation:
Symptoms include flank pain, hematuria, and weight loss.
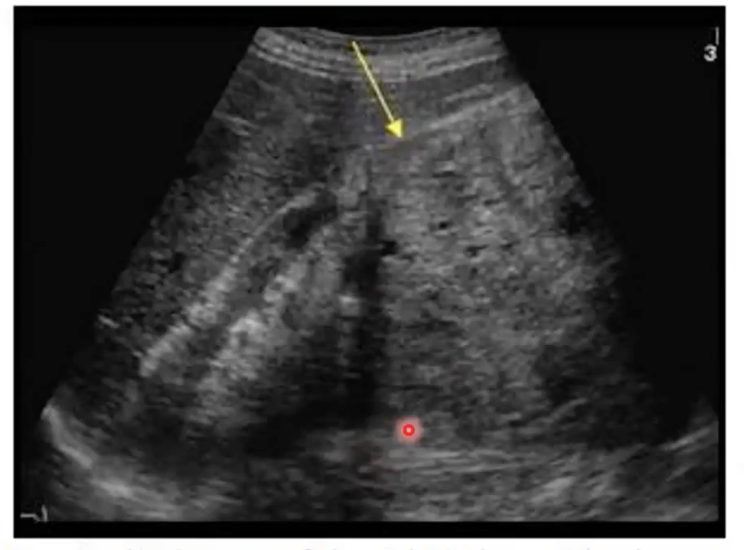
Sonographic Appearance:
Appearance is highly variable and often subtle.
Infiltrative Growth:
These lesions often destroy tissue by invading it directly rather than creating a distinct mass effect.
Subtle Signs:
One indicator can be the lifting of Glisson's capsule (the renal capsule).
Diagnostic Challenges:
Metastases can sometimes be mistaken for Time Gain Compensation (TGC) artefacts if the sonographer is scanning too quickly, as they may appear as subtle changes in the upper or lower poles without clear boundaries.
Summary of Disease Spread
Renal Cell Carcinoma (RCC): Spreads via the vascular system (Renal vein/IVC).
Transitional Cell Carcinoma (TCC): Spreads via the ureter (urinary tract).