The Family and Culture
The Family in Cultural and Community Context
Perinatal and pediatric nurses have responsibilities to families.
Family is a potent support system.
Family health practices are influenced by culture.
Nurses collaborate with families to achieve wellness goals.
Canadian population is diverse, thus nurses need to be culturally competent.
The Family in Society
Social context is viewed in relation to social and demographic trends.
Families set up boundaries between members and outsiders.
Some families isolate, others have community networks.
Defining Family
Traditionally viewed as the primary unit of socialization.
Pivotal role in health care.
Influences and is influenced by other people and institutions.
No universal definition; individual perspective (own frame of reference, judgement, discipline) determines family.
Biologists: Fulfills biological function of perpetuation of the species.
Psychologists: Emphasize the interpersonal aspects of the family and its responsibility for personality development.
Economists: Family as a productive unit providing for material needs.
Sociology: Social unit interacting with larger society, creating cultural values and identity.
Relationships:
Consanguineous: Based on blood relationships.
Affinal: Based on marital relationships.
Family of origin: Family unit a person is born into.
Definition has broadened to reflect structural and functional changes.
Current Definition: An institution where individuals related through biology or enduring commitments. Represents similar or different generations and genders, participate in socialization, nurturance, and emotional commitment.
Family Organization and Structure
Individuals define their family and support system.
May include 2 or more different people parents, siblings, grandparents, partners, aunts, uncles, or friends.
Nuclear Family:
Male and female partners and their children living as an independent unit.
Multigenerational (Extended) Families:
Grandparents, children, and grandchildren living in the same household.
Becoming increasingly common.
Network is an important resource for Indigenous peoples.
Blended Families:
Formed as a result of divorce and remarriage, consist of unrelated family members.
Lone-Parent Families:
Unmarried biological or adoptive parent.
Result from loss of spouse by death, divorce, separation, or desertion; from unplanned or planned pregnancy; adopting of child by unmarried person
Significant statistic point to most have female family head. Female-headed lone parent more likely to have lower income and experience poverty
Same-Sex Couple Families:
Live together with or without children.
Children maybe be conceived from previous relationship
Transgendered Couples:
Form families and often become parents through fertility treatments, adoption, or self-pregnancy (for transmen).
Family Dynamics
Ideally provides a safe, intimate, and nurturing environment.
Provides for nurturing and socialization of children.
Earliest relationships and close relationships with parents influence self-worth and later relationships.
Influences child’s perceptions of the outside world.
Provides the growing child with an identity of past and future.
Cultural and religious beliefs, values, and rituals are passed down.
Develops protocols for problem-solving based on family values and attitudes abt appropriateness of behaviour and influenced by social, moral, political, and economic messages.
Power to make decisions is given through tradition or negotiation.
All families have strengths and potential for growth.
Family Nursing
Primary focus of health care delivery for perinatal and pediatric nurses.
Share information in a positive, useful, timely, complete, and accurate way.
Support family participation in care and decision making.
Nurses must be aware that family members may interact differently from the nurse's own family.
Family beliefs about health may conflict with Western health care principles; nurses must incorporate these beliefs.
Family nursing is nursing with childbearing and child-rearing families.
Family-focused nursing practice foregrounds the family in relation to the individual person. Recognizing environmental and community context.
Nurse work with families, relating to them in meaningful way. Draw on relational stance of learning with people, identifies patterns of responsibilities, social commitments, and addresses social determinants that influence health
Family nursing practice is collaborative, directed by needs and goals, growth-oriented, building on strengths (capacities and resources).
Respectful of family knowledge and expertise.
Congruent with the principles of multi-disciplinary family-centred care.
Principles of Family-Centred Interprofessional Health Care (FCC)
Important in all health care contexts.
Informed by research evidence.
Requires a holistic approach.
Requires collaboration among care providers.
Culturally appropriate care is important in a multicultural society.
Indigenous people and communities have distinctive knowledge, health needs, and experiences.
Providing care to families as close to home as possible is ideal.
The attitudes and language of health care providers affect the family’s experiences with health care.
Functions within a health care system that requires ongoing evaluation.
Learning about FCC practices globally may offer valuable options for consideration in Canada.
Theories as Guides to Understanding and Working With Families
Family theory describes families and their response to events.
Each makes assumptions, has strengths and limitations.
Guides assessment and interventions.
Theories and Models Relevant to Family Nursing Practice
Family Systems Theory
Family is viewed as a unit, focusing on interactions among members rather than individuals.
Part of a larger supra-system and composed of sub-systems.
The family, as a whole, is greater than the sum of its individual members.
A change in one member affects all members.
Balances change and stability.
Behaviors are understood through circular causality.
Family Life Cycle (Developmental) Theory
Families move through stages.
Life cycle is the context for the identity and development of the individual.
Relationships go through transitions.
Main value in irreplaceable relationships.
Different structures and cultures organized in various ways.
Developmental stresses may disrupt the life cycle process.
Family Stress Theory
Concerned with how families react to stressful events.
Stress studied within internal and external contexts.
Internal Context: Elements the family can control/change (family structure, psychological defenses, philosophical values).
External Context: Elements outside family control (culture of larger society, history, economy, maturity of individuals, success of family in coping with stressors, genetics).
McGill Model of Nursing
Strength-based approach compared to deficit approach
Identify family strengths and resources, provision of feedback about strengths, assistance given to family to develop, and elicit strengths and use resources are key interventions
Relevant for childbearing families, as pregnancy is a “teachable moment”.
Collaborative Partnership Approach
Builds on the McGill model.
Develops collaborative partnership = pursuit of PCC thru dynamic process that requires active participation and agreement of all partners
Sharing expertise and power.
Being respectful, accepting, and non-judgemental.
Being open to learning together and living with ambiguity.
Being reflective and self-aware.
Family Assessment
Consider focus of care, prioritize health promotion.
Help the family foster a healthy pregnancy, childbirth, and integrate newborn.
Address conditions of vulnerability (i.e., poverty, ill children) while promoting health.
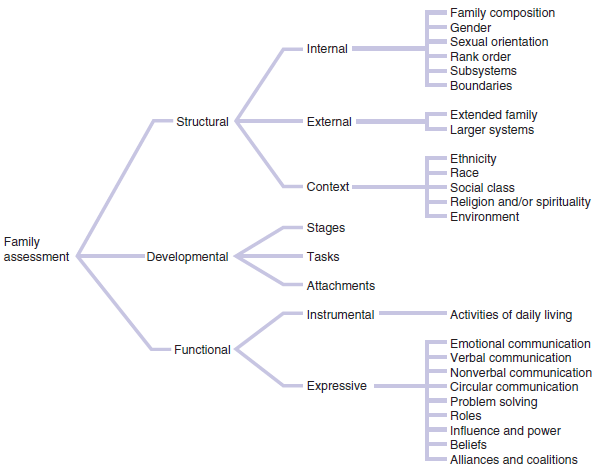
Calgary Family Assessment Model (CFAM)
Guide for assessing family aspects.
Based on nurse’s experiences, beliefs, and relationships.
One perspective at one point in time
Consists of three categories: structural, developmental, and functional.
Provides data to understand the family and formulate a plan of care.
Interviews with family members gain understanding of structure, development, and function.
Box 2.2: Three major categories
Structural Assessment
determine members of family, relationship among family members, and context of family
genograms and ecomaps outlines internal and external structures of family
Developmental Assessment
describe developmental life cycle - typical trajectory most families experience
Functional Assessment
evaluate ways in individuals behave in relation to each other in instrumental (= activities of daily living) and expressive (=communication, problem-solving, roles, among others) aspects
Graphic Representations of Families
Family Genogram
Family-tree format depicting relationships over at least three generations.
Provides info about family, placed in the nursing care plan.
Ecomap
Graphic portrayal of social relationships of the individual and family.
Helps understand the social environment and identify support systems.
Family Nursing as Relational Inquiry
Nurses need to be “in relation” with families.
Identify patterns and build knowledge for health promotion.
Recognizing families are socially located in historical, cultural, and environmental contexts
Relational nursing moves towards holistic health promotion.
Process of inquiry forms the framework for thoughtful thought.
Nurses learn with the family about what matters most.
Phenomenological Lens: Learn about experiences of health and illness, explore values of the family.
Sociopolitical Lens: Attend to power, gender, class, ethnic, racial, and professional relationships.
Spiritual Lens: Health has personal, cultural, and religious meanings.
Socioecological Perspective: Focuses on the family in their environmental context, supporting choices and enhancing capacity.
Cultural Factors Related to Health
Historically, culture evolved from anthropology and referred to the beliefs, values, and traditions of the exotic and essentialized “other”.
Now understood as constructed historically by the person’s life experiences, and by their gender and social position.
People express cultural identities in many ways beyond population groupings.
Dynamic and changes throughout life.
Think about multiple “identities” that make up cultural backgrounds.
Requires attention to the interplay of beliefs, values, and practices.
Multiculturalism in Canada
In 1971, Canada adopted multiculturalism as an official policy.
Affirmed the value and dignity of all Canadians, regardless of origin, language, or religion.
The rights of Indigenous peoples.
Status of Canada’s two official languages: French and English.
Promotes participation in social, cultural, economic, and political affairs.
Every-one is equal and has a right to be heard.
Government intentions have not been sufficient to achieve equity and integration.
Racism and cultural oppression are realities for many minority groups, especially for Indigenous people who have experienced the long-standing impacts of poverty, poor health, loss of identity, and marginalization.
Cultural Context of the Family
Culture is influenced by religion, environment, and historical events.
Ongoing process that influences people throughout life.
Determine the social determinants of health.
Cultural knowledge includes beliefs and values about each facet of life, passed to the next generation.
Influences perceptions of illness, health care-seeking behaviour, and responses to treatment.
Insight into how a person might react to illness, pain, medical procedures, as well as patterns of human interaction and expressions of emotion.
Nurses working with childbearing and child-rearing families should be aware of the impact that highly technological health care environments may have on the ways that family members experience health care and nursing practices.
Be aware of multiple identities of client.
Acculturation
Changes within or among groups when cultures come in contact.
Can result in similarities in dress, lifestyle, and mannerisms.
Diversity and multiculturalism are valued.
Ethnocentrism
View that one's own way is best, others unnatural or inferior.
Leads to ethnic stereotyping.
Influences ability to evaluate beliefs of others.
Biases interpretation.
Culturally competent nurse should be empathetic.
Nurses must respect cultural beliefs.
Self-awareness helps avoid stereotyping.
Attitudes have an impact on people around them.
Providing Culturally Competent Nursing Care
Professional and ethical responsibility to be mindful of culture.
Examine own beliefs to appreciate beliefs of patients.
Values of respect, valuing difference, inclusivity, equity, and commitment to culturally safe care.
Assess beliefs, values, and practices of individuals and families, and value diversity while seeking to learn from families.
Understand and value diversity.
Cultural competence is an ongoing, interactive process.
Aboriginal Nurses Association of Canada (2009) identifies two foundations:
Culture is a complex shifting relational process.
Cultural safety requires understanding power differentials and addressing inequities.
Cultural competence can also be understood as a lifelong process of relational inquiry, by working with Indigenous communities across Canada.
Involves self-reflection on cultural values.
Improving Indigenous maternal and child health includes:
Holistic Approach vital to Indigenous maternal and child health.
The physical, mental, social, spiritual, and emotional components of health are inseparable
Embodying mutual respect and addressing what matters most to the person and family.
Cultural Safety
Environment free of discrimination and racism, safe to receive health care.
Recognize and address power imbalances.
Cultural Humility
Process of self-reflection to raise awareness of biases.
Maintain respectful relationships based in mutual trust.
Acknowledge own practices are not always the “best”.
Need to recognize barriers to transcultural communication and work toward removing those barriers, be aware of the “nursing culture”.
Be responsible and incorporate culturally appropriate and safe care into nursing practice.
Spirituality
Gives ultimate meaning and purpose in one’s life, inviting ways of being in the world in relation to others, oneself, and the universe.
Important in all phases of life, affecting how patients face health issues.
One can be spiritual without being religious.
Component of holistic nursing.
Open to a range of spiritual perspectives.
Reflect on own spiritual beliefs to provide beneficial care.
Nurses can arrange visits with clergy, pose questions about preferences/requests for prayers/blessings/counselling.
Baptisms, anointings, blessings, sacrament of the sick, memorial services etc. may be held.
Can choose to remain for the service or decline respectfully.
Nurse need not be of the same religion to provide support in difficult times such as death.
Spiritual Care
Relational practice to increase the spiritual well-being of the person and family.
Features of spiritually literate person: being present, having compassion, and hope, being kind, listening, having meaning openness, and using silence.
Requires listening, knowing what is important to the patient and responding accordingly.
Communication
Complex, involving understanding the individual’s language and interpersonal style, and accurately interpreting speech volume, touch, and gestures.
Avoid rushing to judgement.
Need to enlist assistance to verify the true intent and meaning.
Use of Interpreters
Services sought by agencies for linguistically appropriate health care.
Interpreter should have same native language, religion, or country of origin as patient and specific health-related language skills.
Avoid using children or family members.
Access professional interpreters over telephone when unavailable in person.
Create atmosphere of respect and privacy.
Address questions to the person, not the interpreter.
Ensure confidentiality.
Ensure culturally and linguistically appropriate educational materials are available.
Personal Space
Traditions define appropriate space for social interactions.
Physical dimensions of comfort zones differ from culture to culture.
Actions such as touching, proximity, taking possessions, and making decisions for individual can decrease security and heighten anxiety.
Respecting need for distance supports autonomy and control.
Time Orientation
Affects health behaviors.
May be oriented to past, present or future.
Orientation affects nursing care; consider family focus when planning.
Family Roles
Expectations and behaviours associated with a member’s position in the family.
Social class and cultural norms also affect these roles.
Acknowledge which family member makes the major decisions.
The way that health care practitioners facilitate such a family’s care may influence the family’s experience and perception of the Western healthcare system.