8. Brucella, Francisella, Pasteurella
Brucella, Francisella, Pasteurella: Overview
General Information
Tibor Pál, Department of Medical Microbiology and Immunology, University of Pécs, Hungary
Brucella
Clinical Case Example
Patient: 34-year-old male with lower back pain for 3 months.
Symptoms: Lower back pain, low-grade fever, weakness, increased RBC sedimentation.
Long standing, no specific symptoms
MRI Findings: Extradural defect at L4-L5.
Biopsy Results: Signs of granulomatous inflammation; ruled out tuberculosis.
Exposure History: Consumed raw milk from goats and camels in the Middle East.
Diagnosis: Elevated brucella-specific antibodies; identified as Brucella abortus via blood culture.
Microbiology
Small Gram-negative coccobacilli.
Slow-growing with 12 recognized species.
Main reservoirs: Wild and domestic animals.
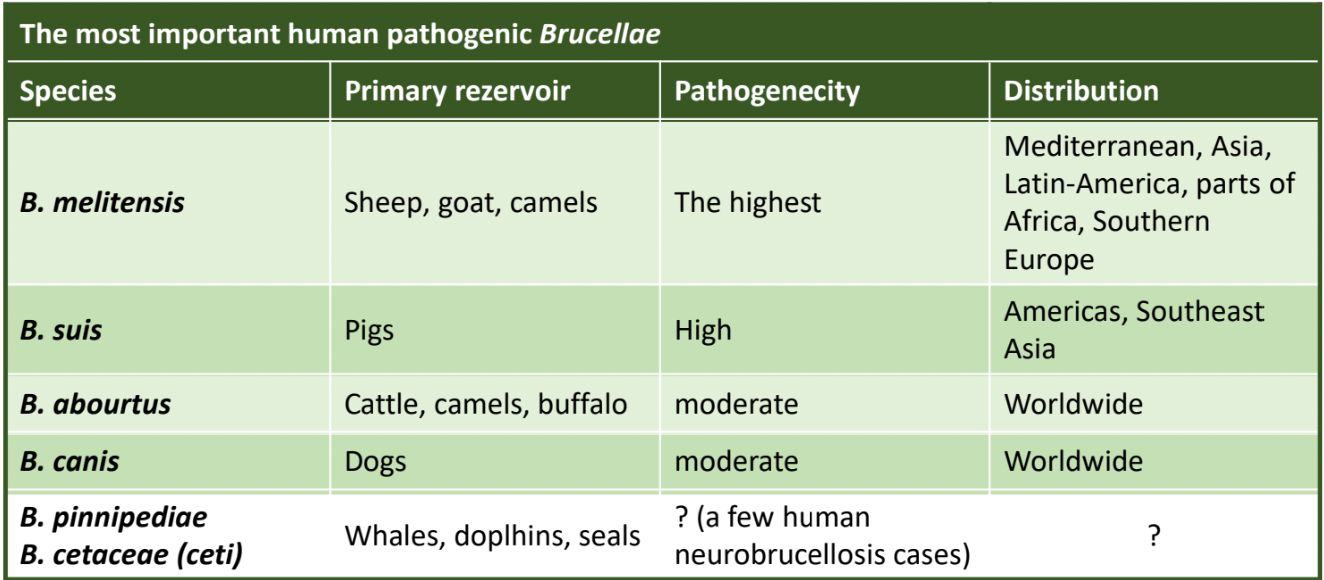
Human Pathogenic Species
B. Melitensis: Mostly from sheep, goats, camels (high pathogenicity, prevalent in Mediterranean, Asia, Latin America).
B. suis: Pigs (high pathogenicity, in Americas, Southeast Asia).
B. abortus: Cattle (moderate pathogenicity, worldwide).
B. canis: Dogs (moderate pathogenicity, worldwide).
Global Incidence
Approximately 2.1 million estimated human cases/year.
Most prevalent bacterial zoonotic infection.
Major economic impact due to abortions in animals.
Pathogenecity and Spread
Transmission: Primarily via unpasteurized milk; less commonly by aerosol or direct contact.
Intracellular parasite, primarily targets macrophages, cells of the RES; survives and replicates in ER.
Facultative IC parasite → can live in and outside of cells
Immune Response and Clinical Presentation
Symptoms can be acute or chronic. Common features include undulant fever, malaise, weight loss, joint pain, and abdominal symptoms.
Potential organ-specific symptoms include osteomyelitis, endocarditis, and urinary tract infections.
Laboratory Diagnosis
Culture and serology needed, as cultures may take weeks.
Blood samples are preferred; specialized media for culture.
also bone marrow biopsy, organ specific samples
write your suspicion as it is slow growing → extend incubation time
Standard Agglutination Test (SAT) diagnostic for B. abortus, with a titre of ≥160 being significant. (≥320 in endemic areas)
Work in BSL II safety cabinet
2-Mercaptoethanol test → treatment of serum with 2-ME eliminates cross-reacting or persisting IgM antibodies - testing serum simultaneously in SAT → IgG only!
main use: monitoring response to antibiotic therapy
Rose bengal Test
Coombs test
Treatment and Prevention
Treatment involves antibiotics such as doxycycline, rifampin, or gentamicin. Relapse potential decreases with proper treatment.
Children <8 years → TMP-SMZ
Pregnancy → Rifampin (+/- TMP-SMZ)
Prevention focuses on avoiding unpasteurized products and controlling animal exposure.
slaughtering infected animals, also vaccination of animals
Francisella
Clinical Case Example
Patient: 56-year-old with symptoms suggesting tularaemia after a tick bite.
Diagnosis: Identified as Francisella tularensis through culture.
Microbiology
Small, Gram-negative coccobacilli, aerobic and capsulated.
Multiple subspecies: Type A and Type B.
Reservoirs and Global Distribution
Zoonosis with reservoirs in a variety of wild and domestic animals.
Infection primarily occurs in the Northern Hemisphere.
Spread and Pathogenesis
Transmission via inhalation, mucosal surfaces, skin injuries, or ingestion.
Immune evasion via atypical LPS and modulation of cytokine response.
Clinical Picture
Depends on portal of entry: ulceroglandular, glandular, or pneumonic presentations.
Ulceroglandular: skin ulcer + localised lymphadenopathy
Glandular: lympadenopathy without skin ulcer
Oropharyngeal: chronic pharyngitis with or without mucosal ulcer and swollen lymph nodes
Oculoglandular: conjunctivitis with lymphadenopathy
Pneumonic: inhalation or hematogenous spread to the lungs
Typhoidal: Sysetmic after any portal of entry
Laboratory Diagnosis
BIOHAZARD! Laboratory infections !!!
Serology: Microagglutination, recently ELISA and Western blot
At presentation often negative
Definitive is the 4x increase of titres
Culture: Slow, often negative. Needs special media
PCR: Promising, even good for subspecies determination
Others: Indirect immunofluorescence
Treatment and Prevention
Suspected case: exposure history + consistent clinical symptoms
Presumptive case:
suggestive clinical symptoms
antigen or DNA detection
single positive serum
Confirmed case:
recovery and identification of the isolate or paired serum show ≥4 fold increase in titre
Therapy:
Aminoglycosides (streptomycin, gentamicin)
Fluoroquinolones (ciprofloxacin, levofloxacin)
Doxycycline
Natural resistance to beta-lacatms due to beta-lactamase production
Preventions:
Currently no licensed vaccine (perviously a live, attenuated one)
Prevent contact
NOTE: a potential biological warfare
Pasteurella
Clinical Case Example
Patient: 42-year-old with a dog bite experiencing swelling and inflammation.
Identified as Pasteurella multocida from cultures after incision and antibiotic treatment.
Microbiology
Found in the oral and upper respiratory tract of animals/humans.
Gram-negative pleomorphic coccobacillus (bipolar staining).
Grows on blood agar
Transmission to Humans
Exists in various animals, and can transfer to humans by:
animal bites
scratches
licks on skin abrasions
contacts with mucus secretion
Human infections:
swelling, cellulitis
bacteriaemia
osteomyelitis
endocarditis
line infections
meningitis
pneumonia (relatively rare)
Lab Diagnosis and Treatment
Culture often negative; treatment should account for mixed infections from bites.
Recommended antibiotics include amoxicillin or doxycycline combined with metronidazole.
Further Readings and Contact
Refer to "Medical Microbiology, 8th ed., 2015, Elsevier."
For inquiries: pal.tibor2@pte.hu