327 Autism
327 Autism
Dr. Calum Hartley
Email: c.hartley@lancaster.ac.uk
Institution: Lancaster University
Disclaimers
Autistic Perspective: The presenter, Dr. Hartley, is not autistic but has extensive experience working with the autistic community.
Variability of Experiences: Individual experiences with autism may differ significantly from the information presented.
Scope of Lecture: It is acknowledged that it is impossible to cover all critical issues regarding autism in a single lecture.
Today’s Lecture Overview
What is autism?
Autism through the years.
How is autism assessed?
Interventions for autistic individuals.
What is Autism?
Definition and Characteristics of Autism
Neurodevelopmental Condition:
First identified by Kanner (1943).
Considered a lifelong condition.
Involves multiple contributing genes.
Identified differences in brain structure and function.
Sensory differences → can be overtimulating or something a person seeks to regulate.
Co-occurring conditions are common.
Increasing Prevalence:
Currently, autism is estimated to affect 1-2% of children worldwide (Maenner et al., 2021).
Is autism more frequent now?
Wider diagnostic criteria may contribute to the increasing rates.
→ used to be a narrow description and a person would have to meet all criteria and show every characteristic.
→ some aspects of the criteria have changed e.g. no longer expects people to have a mental or intellectual deficit.
Increased public and medical awareness leads to more diagnoses.
→ parents more aware so earlier diagnosis
Gender Differences:
Autism is more frequently diagnosed in boys than in girls.
Females are often chronically underdiagnosed (Bargiela et al., 2016).
Research predominantly conducted with male samples may skew findings.
Diagnosis tends to occur later for females than for males (Shattuck et al., 2009).
Recent studies are exploring the ‘female autism phenotype’ (Hull et al., 2020) which reveals differing language use and “masking” behaviors (social camouflaging; Hull et al., 2017).
→ masking can lead to mental helath issues such as depression and anxiety as it takes a lot of mental energy
girls are less liekly to have intellectual deficits
Spectrum Condition:
Autism is characterized as a spectrum condition, indicating that every autistic person is unique.
The intensity and nature of traits can vary significantly among individuals.
Multiple diagnostic categories existed until the DSM-V.

Learning Disabilities:
It is estimated that 30-60% of autistic children show signs of intellectual disability (e.g. Shaw et al., 2023).
Those with intellectual disabilities are generally diagnosed earlier in life.
Autistic individuals’ learning disabilities can limit information processing and the use of compensatory strategies.
Language Acquisition:
Language acquisition can often be delayed, though this is not always the case.
There is substantial variation among autistic children.
Approximately 30% are nonverbal or minimally verbal (5 words or less) by 9 years old (Anderson et al., 2007).
Some children may experience regressive symptoms.
A common area of difficulty is pragmatics, which can affect later outcomes.
Behavioral Characteristics
Behavioral characteristics vary greatly among individuals both in presence and intensity.
Evolution of Autism Understanding
Autism Through the Years
The American Psychiatric Association (APA) did not publish separate criteria for autism as a unique condition until 1980.
Historical Diagnostic Criteria
DSM III (1980): Infantile Autism
Symptoms must be evident before 30 months.
Features include pervasive lack of responsiveness to others, significant impairments in language development, peculiar speech patterns (if present), unusual responses to environmental aspects, and absence of schizophrenic symptoms.
DSM III-R (1987): Autistic Disorder
Defined by 8 of 16 criteria behaviors across 3 categories:
(a) social interaction
(b) verbal & non-verbal communication & imagination
(c) restricted interests & activities.
Assessing Autism
Retained criteria similar to DSM III-R with some adjustments:
(a) social interaction
(b) communication
(c) restricted/repetitive behaviors, interests, and activities
Introduced multiple diagnostic categories including:
Pervasive Developmental Disorders
Rett's Disorder
Childhood Disintegrative Disorder
Autism Spectrum Disorders
Autistic Disorder
PDD-NOS and Asperger Syndrome.
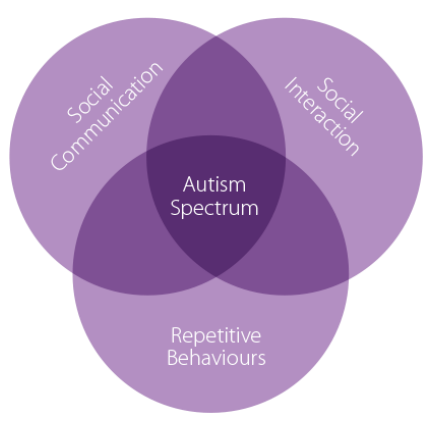
Diagnostic Definition in DSM V (2013) & V-TR (2022): Autism Spectrum Disorder
A. Persistent deficits in social communication and interaction across multiple contexts.
B. Restricted, repetitive patterns of behavior, interests, and activities.
C. Symptoms must be present early in childhood.
D. Symptoms must cause clinically significant impairment in important areas of functioning (e.g., social, occupational).
E. Disturbances should not be better explained by intellectual disability.
Major Changes in DSM V (2013) & V-TR (2022)
Severity Levels:
Determined by the degree of difficulties in communication and behavioral flexibility.
Level 1: “requiring support”
Level 2: “requiring substantial support”
Level 3: “requiring very substantial support”
Single Diagnosis:
Introduced a single ‘Autism Spectrum Disorder’ diagnosis rather than distinct diagnostic categories.
Reduction of Diagnostic Domains:
The number of characteristic domains reduced from three to two.
Inclusion of Sensory Behaviors:
For the first time, sensory behaviors were included in the diagnostic criteria.
Specifiers:
Helps describe difficulties of an individual holistically. Examples include:
“with/without accompanying intellectual impairment”
“with/without language impairment”
“associated with known medical/genetic condition”
“with another disorder”
Reasons for Changes in Diagnostic Criteria
Reduction from 3 to 2 domains:
Recognizes that difficulties in communication and social interactions represent a single set of characteristics rather than two.
Removal of Separate Diagnoses:
Validity concerns: Evidence indicates reliable distinctions exist between autistic and neurotypical development, whereas distinctions among conditions within the spectrum were less clear.
Appropriateness: Past diagnostic biases attached to socio-economic status affecting accessibility to support services were addressed.
Assessing Autism
Overview of Assessment
Diagnosis is primarily behavior-based rather than based on etiology.
Relies on a consensus of behavioral criteria distributed across the DSM.
Diagnoses typically occur during early childhood, though not exclusively.
Diagnostic Process
Requires evaluation by a multidisciplinary team, including:
Psychiatrist
Speech and language therapist
Psychologist
Assessment components include:
Behavioral reports gathered from various settings.
Autism-specific assessments regarding developmental and family history (e.g., Diagnostic Interview for Social and Communication Disorders).
Observational assessments of the child’s behavior (e.g., Autism Diagnostic Observation Schedule).
Autism Diagnostic Observation Schedule (ADOS-2)
The ADOS-2 is recognized as a ‘gold standard’ autism assessment tool.
This semi-structured interview tool presents children with various activities designed to elicit autism-related behaviors:
Language
Social communication
Play
Restricted behaviours
Diagnostic outcomes are based on the child's behaviour during the entire interaction, which is typically video recorded.
Interventions for Autistic Individuals
Background of Interventions
The overarching aim of interventions is to assist autistic individuals and their caregivers in overcoming challenges affecting learning, social interactions, and the quality of life.
No single intervention is deemed “best”; individuals often receive multiple concurrent interventions.
The efficacy of interventions can vary: a strategy that works well for one individual may not be effective for another.
Key Recommendations for Interventions
Interventions should be initiated as early as possible to take advantage of the neuroplasticity present in developing brains (Kolb & Gibb, 2011).
Following early influential studies (e.g., Lovaas, 1987; McEachin et al., 1993), it is often suggested that interventions need to be intensive (though consensus on this is not universally agreed).
A comprehensive approach is suggested, targeting broader development rather than isolated skills.
Types of Intervention
Pharmaceutical Interventions
More than 50% of autistic children in the US are prescribed medication (Cascade et al., 2008).
Medications may help reduce certain features of autism and alleviate challenging behaviors.
They can mitigate behaviors that might hinder the effectiveness of other interventions, but the effects are usually short-term.
Serious side effects may occur, including sedation, weight gain, dizziness, and involuntary movements.
Behavioral Interventions
These interventions utilize operant conditioning principles and represent early approaches aimed at enhancing outcomes across various domains (Ferster & Demyer, 1962).
They often involve presenting a stimulus, prompting the target behavior from the child, and providing extrinsic positive reinforcement (“discrete trial training”).
- Skills targeted are based on individual needs and taught through structured interactions before gradually introducing more diverse settings and partners.
Initial studies indicated that early intensive behavioral interventions could yield significant improvements in cognitive and academic outcomes (Lovaas, 1987; McEachin et al., 1993).
The principles of these early studies contributed to the establishment of Applied Behavior Analysis (ABA), which is the most prevalent and well-funded clinical approach, especially within the United States (Green et al., 2006; Stahmer et al., 2005).
ABA has faced notable ethical criticisms and has been associated with negative mental health outcomes in autistic adults (Kupferstein, 2018; Sanoval-Norton & Shkedy, 2019).
Developmental Interventions
Grounded in constructivist and social learning theories, these interventions postulate that children actively learn through exploration and interaction with others (Vygotsky, 1978).
Early challenges with prelinguistic social processes (e.g., joint attention) can disrupt the quality of caregiver-child interactions, impacting communicative development.
These interventions focus on enhancing basic social communication to lay a foundation for more complex skills in development.
Naturalistic Developmental Behavioral Interventions
Defined in 2015 (Schreibman et al., 2015), these approaches combine both developmental and behavioral principles.
Interaction occurs in play, where control of the interaction is shared between adult and child in a balanced manner.
Research by Kasari et al. (2014) indicates that fostering joint attention and symbolic play at ages 3-4 predicts improved spoken language by age 8.
Alternative Interventions
Various alternative treatments exist, including changes in diet, supplementation, homeopathy, chelation therapy, and massage.
A significant body of epidemiological evidence refutes the association between environmental triggers and the emergence of autistic traits.
Some alternative therapies carry substantial risks; an incident in 2005 highlighted the fatal outcome of an autistic child undergoing chelation therapy (Brown et al., 2006).
Evaluating Interventions
Key Research Findings by Sandbank et al. (2020)
Conducted a systematic review and meta-analysis encompassing seven early intervention types for autistic children up to the age of 8. The intervention types included:
Behavioral
Animal-assisted
Developmental
Sensory-based
Naturalistic Developmental Behavioral Interventions (NDBIs)
Technology-based
TEACCH (Treatment and Education of Autistic and Communication Handicapped Children)
The analysis involved data from 6,240 participants across 130 samples.
Effectiveness was evaluated across 15 outcome measures of autistic characteristics.
Key Findings
NDBIs emerged as the best-supported intervention type based on high-quality research (e.g., randomized controlled trials, direct measures), with benefits evident in social communication, play skills, and language.
Behavioral interventions, while extensively researched and commonly recommended (e.g., EIBI), presented limitations due to the overall low quality of supporting evidence.
- Developmental interventions showed effectiveness in enhancing social communication and interaction synchrony but did not necessarily improve language skills.
Limitations of Existing Intervention Evidence Base
Many participants were not randomly assigned to intervention conditions.
Outcome measures heavily relied on caregiver reports.
The boundedness of intervention effects: considerations of temporal and contextual factors.
Autistic Adults
Life outcomes for autistic individuals exhibit a wide variance; many require ongoing support into adulthood, with employment rates hovering around 50% (Howlin et al., 2004; Roux et al., 2013).
Language difficulties may improve over time, but persistent differences in social interaction and communication can remain and may become more pronounced.
Increasingly complex social demands are associated with heightened mental health challenges (Volmar et al., 2014).
Conversely, some autistic adults achieve impressive academic success and pursue high-level professional careers (Costello et al., 2021).
Lecture Summary
Autistic conditions are characterized as neurodevelopmental conditions marked by differences in social communication, interaction, and restricted/repetitive behaviors.
Assessment is based on the behavioral observations performed in early childhood, with guidelines derived from contemporary research (as outlined in the DSM V).
Numerous interventions exist to address the varied characteristics of autism, albeit with varying degrees of effectiveness.
The End
Next Week's Topic
Upcoming Lecture Topic: Eating Conditions
Speaker: Ruth Hurley
Institution: Lancaster University