6Tc: Steroids
Mechanisms of Action of Topical Steroids
Inhibition of Phospholipase A2: Reduces inflammation by decreasing the production of arachidonic acid, thereby inhibiting the production of prostaglandins.
Effects on Cellular Activity:
Inhibit cellular migration
Stabilize mast cells, reducing histamine release
Decrease fibroblast proliferation
Reduce vasodilatation and edema
Prevent scar tissue formation
Steroids and Their Functions
Produced by the adrenal cortex:
Glucocorticoids: Involved in glucose, protein, and bone metabolism; exhibit anti-inflammatory effects.
Mineralocorticoids: Maintain electrolyte balance.
Sex Hormones: Hormones related to reproduction.
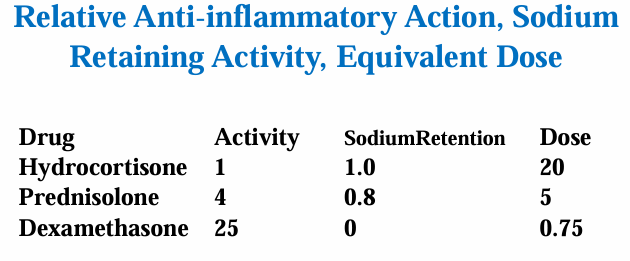
Natural Glucocorticoids: Corticosterone, hydrocortisone (Na retention creating water retention).
Synthetic Steroids: Developed to be potent anti-inflammatories with lower Na retention.
Corticosteroid Actions
Suppress inflammation, not a cure; prevents scarring and vascularization in ocular structures.
inhibit most aspects of the inflammatory response
Timelines of Action:
Early stage: Reduces heat, swelling, pain, and redness.
Late stage: Can inhibit wound healing and repair.
anti-inflammatory action: very valuable but hazardous
Uses of Corticosteroids in Ocular Disorders
Commonly prescribed for a range of acute ocular inflammatory disorders such as:
Viral Keratoconjunctivitis (VKC)
Chemical burns
Post-keratoplasty conditions
Anterior and posterior uveitis
Preferred usage: Topical therapy to avoid systemic side effects associated with oral steroids.
General Principles of Corticosteroid Use
Treatment Initiation: Start as soon as indicated.
Dosage Management: Must be adequate for inflammation suppression; frequent evaluation of dosage. Strong enough to suppress the inflammation.
Tapering: Long-term treatments must be tapered after symptoms subside to prevent relapses.
the premature halting of treatment can lead to relapse. Often the second episode is worse than the first.
Important Guidelines for Optometrists
Understanding immunological processes related to ocular inflammation:
immunological processes relevant to inflammatory conditions of the eye and their natural histories
Knowledge of typical presentations and differential diagnoses.
Immediate treatment for ocular emergencies.
Identification of risk factors and potential side effects, including increased intraocular pressure and cataract risk.
Generally, optometrists will be using topical steroids for conditions that resolve in the short term. Expert opinion should be sought for long-term steroid use.
no repeats for steroids
In selecting a corticosteroid preparation, optometrists should select the preparation that is most likely to effectively treat the condition of the patient with the least propensity for side effects.
Topical steroid preparations with a propensity for intraocular penetration, such as dexamethasone and prednisolone, should not be used for conditions that are responsive to less readily absorbed steroids
Topical Ocular Corticosteroids
Availability: Subject to prescription (S4) in Australia.
Examples include:
Fluorometholone: (e.g., Flarex, Flucon)
Hydrocortisone: (e.g., Hycor)
Dexamethasone: (e.g., Maxidex)
Prednisolone: (e.g., Minims)
Prednefrin: Prednisolone Plus phenylephrine
Potency and Pharmacologic Comparisons
Potency Ranking (weakest to strongest): FML < Flarex < Maxidex < Prednisolone < Prednefrine forte.
Most potent: Dexamethasone (Maxidex) as it is produced in the lowest concentration (0.1%)
high concentrations of a given agent are not more effective.
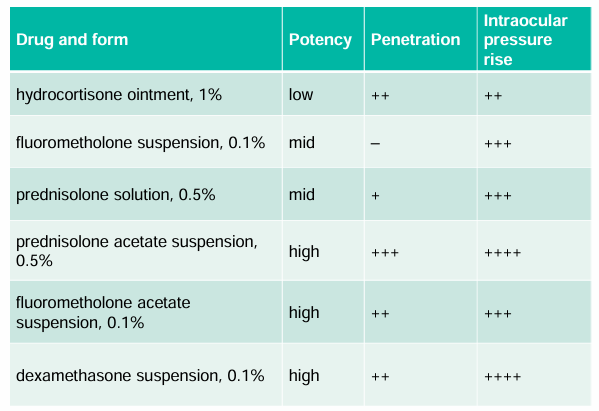
suspension = bottle must be shaken with use.
Fluorometholone (Flarex, FML)
weakest steroid available.
Action: Corticosteroid, relatively non-penetrating.
Use: Indicated for steroid-responsive inflammatory ocular conditions.
Contra/Caution: Use with caution in patients with:
Viral infections
Tuberculosis (TB)
Fungal infections
Prolonged use
Corneal thinning
Pregnancy
Children
Adverse Effects:
Increased risk of glaucoma
Cataract formation
Risk of superinfection
Less increase in intraocular pressure (IOP) compared to other steroids.
Pack:
0.1% concentration, 5ml, in suspension form.
Must shake well before use; acetate version is more effective and metabolized slower than alcohol forms.
Dose:
Administer 1-2 drops, 2-4 times per day.
If necessary, increase to 2 drops every 2 hours.
Gradual tapering is recommended, along with nasolacrimal occlusion techniques to minimize systemic absorption
Dexamethasone (Maxidex)
Action: Corticosteroid, stronger than phosphate derivatives due to alcohol derivatives.
Use: Indicated for intraocular inflammatory eye diseases.
Contra/Caution: Use with caution in patients with infections, prolonged use, corneal thinning, pregnancy, and children.
Adverse Effects: Includes glaucoma, cataract formation, risk of superinfection, and has the highest propensity to increase intraocular pressure (IOP).
Pack: Available in 0.1% concentration, 5ml.
Dose:
Severe: 1-2 drops every hour, decrease as inflammation subsides;
Mild: 1-2 drops every 4-6 hours, along with nasolacrimal occlusion, and taper as necessary.
Prednisolone (Prednefrin Forte)
Considered the most effective for anterior segment ocular inflammation.
Action: strong corticosteroid, prednisolone acetate; considered the most effective anti-inflammatory agent for anterior segment ocular inflammation.
Use: Severe inflammatory eye disease. Systemic: Oral forms available for asthma and chronic obstructive pulmonary disease (COPD).
Contra/Caution: Use with caution in patients with infections, glaucoma, pregnancy, lactation, and children.
Adverse Effects: Increased intraocular pressure (IOP), cataracts, and corneal thinning.
Pack: Available in 1% concentration, 10ml.
Dose: 2 drops every hour for 2 days, then 1-2 drops 2-4 times/day, tapering and using nasolacrimal occlusion as necessary.
Hydrocortisone (Hycor)
Action: 1st corticosteroid discovered, largely superseded, topical skin treatment.
Use: Inflammatory eye disease (including Herpes Zoster).
Contra/Caution: Use with caution in patients with infections (TB, fungal, viral), corneal thinning, prolonged use, cataract, diabetes, glaucoma, pregnancy, and children under 2 years. Interacts with topical ophthalmic agents (use 10 minutes apart). Has marked mineralocorticoid properties, may cause sodium and water retention and potassium loss.
Adverse Effects: Increased intraocular pressure (IOP), delayed healing, and cataracts.
Pack: Available in 0.5%, 1%; drops 10 ml; ointment 5g.
Dose: 2-4 times/day, with nasolacrimal occlusion and tapering as necessary.
Topical Steroid Monitoring
need to monitor the:
Corneal epithelium
IOP
lens
especially if used for >2 weeks.
Corticosteroid side effects
Corticosteroids & Cataracts
tend to be bilateral and subcapsular
Dose and duration specific
systemic use carriers greater risk
produces disulphide bonds and protein aggregation
Termination of therapy halts progression, in few cases the size of the opacity decreases
Children and diabetics are more susceptible.
Corticosteroids & IOP elevation
Individual variation in susceptibility exists, with 1-5% of people being steroid responders, and about 1/3rd of users showing a moderate increase in intraocular pressure (IOP).
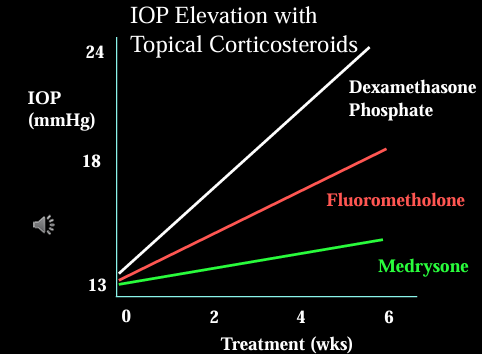
Duration and Dose: These factors are significant in IOP elevation, with a possible lag of 3-6 weeks after starting corticosteroid treatment.
Drug Variation: Different steroids have varied effects; dexamethasone and betamethasone are known to be more problematic. Soft-steroids are less likely to cause IOP increases.
Reversibility: Generally, IOP increases are reversible upon termination of treatment, although steroid-induced glaucoma may not respond to cessation of therapy.
Mechanisms of IOP Increase: The increase in IOP may be due to:
Accumulation of abnormal collagen and/or basement membrane material in the trabecular meshwork.
Lamellar thickening around trabecular structures.
Decreased phagocytic capacity of the trabecular cells, which increases outflow resistance.
What to do if IOP rises
tapering drug will usually decrease IOP
Switch to new “soft steroid” - steroids with less impact on IOP
Add a glaucoma drug if steroid use is continued: beta blocker and alpha agonist
Corticosteroids and infection
Reduce bodies immunologic defence mechanisms
Lower resistance to infection
Mask symptoms of infective disease
Exacerbation of existing bacterial & viral infections
Severe aggravation of herpes simplex and fungal eye infections
In ocular infection Tx, steroids can be beneficial to reduce inflammation and scarring
Avoid if scarring not likely
Must use with concurrent antibiotic/antiviral Tx if ulcer was infective
Other Corticosteroid Side Effects
Ocular: Mydriasis, ptosis, keratitis, corneal thinning, scleral thinning, uveitis, transient ocular discomfort.
Systemic: Electrolyte imbalance, weight gain, delayed wound healing, mood changes, muscle weakness / atrophy, risk of infections, osteoporosis.
Monitor closely if used for longer than 2 weeks.
Contraindications and Drug Interactions
Contraindicated in patients with conditions such as:
Glaucoma
Diabetes
Renal disease
Osteoporosis
Psychiatric disorders
Careful consideration when combined with other medications, particularly anticoagulants.
Additional Notes on Sports Regulations
Systemic corticosteroids are banned in sports; however, non-systemic preparations (including ophthalmic) are allowed with appropriate exemption registration.